
Abstract
Background:
Accurate tibial and femoral tunnel placement has a significant effect on outcomes after anterior cruciate ligament reconstruction (ACLR). Postoperative radiographs provide a reliable and valid way for the assessment of anatomical tunnel placement after ACLR. The aim of this study was to examine the radiographic location of tibial and femoral tunnels in patients who underwent arthroscopic ACLR using anatomic landmarks. Patients who underwent arthroscopic ACLR from January 2014 to March 2016 were included in this retrospective cohort study.
Materials and Methods:
45 patients who underwent arthroscopic ACLR, postoperative radiographs were studied. Femoral and tibial tunnel positions on sagittal and coronal radiographic views, graft impingement, and femoral roof angle were measured. Radiological parameters were summarized as mean ± standard deviation and proportions as applicable. Interobserver agreement was measured using intraclass correlation coefficient.
Results:
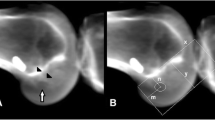
The position of the tibial tunnel was found to be at an average of 35.1% ± 7.4% posterior from the anterior edge of the tibia. The femoral tunnel was found at an average of 30% ± 1% anterior to the posterior femoral cortex along the Blumensaat’s line. Radiographic impingement was found in 34% of the patients. The roof angle averaged 34.3° ± 4.3°. The position of the tibial tunnel was found at an average of 44.16% ± 3.98% from the medial edge of the tibial plateau. The coronal tibial tunnel angle averaged 67.5° ± 8.9°. The coronal angle of the femoral tunnel averaged 41.9° ± 8.5°.
Conclusions:
The femoral and tibial tunnel placements correlated well with anatomic landmarks except for radiographic impingement which was present in 34% of the patients.
Similar content being viewed by others


References
MARS Group, Wright RW, Huston LJ, Spindler KP, Dunn WR, Haas AK, et al. Descriptive epidemiology of the Multicenter ACL Revision Study (MARS) cohort. Am J Sports Med 2010;38:1979–86.
Morgan JA, Dahm D, Levy B, Stuart MJ; MARS Study Group. Femoral tunnel malposition in ACL revision reconstruction. J Knee Surg 2012;25:361–8.
Samitier G, Marcano AI, Alentorn-Geli E, Cugat R, Farmer KW, Moser MW. Failure of anterior cruciate ligament reconstruction. Arch Bone Jt Surg 2015;3:220–40.
Topliss C, Webb J. An audit of tunnel position in anterior cruciate ligament reconstruction. Knee 2001;8:59–63.
Westermann R, Sybrowsky C, Ramme A, Amedola A, Wolf BR. Three-dimensional characterization of the anterior cruciate ligament’s femoral footprint. J Knee Surg 2014;27:53–8.
Ziegler CG, Pietrini SD, Westerhaus BD, Anderson CJ, Wijdicks CA, Johansen S, et al. Arthroscopically pertinent landmarks for tunnel positioning in single-bundle and double-bundle anterior cruciate ligament reconstructions. Am J Sports Med 2011;39:743–52.
Pinczewski LA, Salmon LJ, Jackson WF, von Bormann RB, Haslam PG, Tashiro S. Radiological landmarks for placement of the tunnels in single-bundle reconstruction of the anterior cruciate ligament. J Bone Joint Surg Br 2008;90:172–9.
Sullivan JP, Matava MJ, Flanigan DC, Gao Y, Britton CL, Amendola A; MOON Group, et al. Reliability of tunnel measurements and the quadrant method using fluoroscopic radiographs after anterior cruciate ligament reconstruction. Am J Sports Med 2012;40:2236–41.
Wright RW, Haas AK, Huston LJ, Ross JR, Harris D, Patel K, et al. Radiographic findings in revision anterior cruciate ligament reconstructions from the mars cohort. J Knee Surg 2013;26:239–47.
Howell SM, Gittins ME, Gottlieb JE, Traina SM, Zoellner TM. The relationship between the angle of the tibial tunnel in the coronal plane and loss of flexion and anterior laxity after anterior cruciate ligament reconstruction. Am J Sports Med 2001;29:567–74.
Howell SM, Hull ML. Checkpoints for judging tunnel and anterior cruciate ligament graft placement. J Knee Surg 2009;22:161–70.
Sudhahar TA, Glasgow MM, Donell ST. Comparison of expected vs. actual tunnel position in anterior cruciate ligament reconstruction. Knee 2004;11:15–8.
Jepsen CF, Lundberg-Jensen AK, Faunoe P. Does the position of the femoral tunnel affect the laxity or clinical outcome of the anterior cruciate ligament-reconstructed knee? A clinical, prospective, randomized, double-blind study. Arthroscopy 2007;23:1326–33.
Lee MC, Seong SC, Lee S, Chang CB, Park YK, Jo H, et al. Vertical femoral tunnel placement results in rotational knee laxity after anterior cruciate ligament reconstruction. Arthroscopy 2007;23:771–8.
Author information
Authors and Affiliations
Corresponding author
Additional information
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
Rights and permissions
About this article

Cite this article
Nema, S.K., Balaji, G., Akkilagunta, S. et al. Radiologic assessment of femoral and tibial tunnel placement based on anatomic landmarks in arthroscopic single bundle anterior cruciate ligament reconstruction. IJOO 51, 286–291 (2017). https://doi.org/10.4103/ortho.IJOrtho_219_16
Published:
Issue Date:
DOI: https://doi.org/10.4103/ortho.IJOrtho_219_16