
Abstract
Background: Partial tears of the anterior cruciate ligament (ACL) are common and usually present with symptomatic instability. The remnant fibers are usually removed and a traditional ACL reconstruction is done. But with increased understanding of ACL double bundle anatomy, the remnant tissue preservation along with a single bundle augmentation of the torn bundle is also suggested. The purpose of this study was to evaluate the results of selective anatomic augmentation of symptomatic partial ACL tears. Our hypothesis is that this selective augmentation of partial ACL tears could restore knee stability and function.
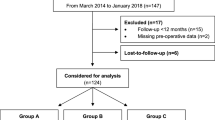
Materials and Methods: Consecutive cases of 314 ACL reconstructions, 40 patients had intact ACL fibers in the location corresponding to the anteromedial (AM) or posterolateral (PL) bundle and were diagnosed as partial ACL tears perioperatively All patients underwent selective augmentation of the torn bundle, while keeping the remaining fibers intact using autogenous hamstring graft. A total of 38 patients (28 males, 10 females) were available with a minimum of 3 years followup. 26 cases had AM bundle tears and 12 cases had PL bundle tears respectively. Patients were assessed with International Knee Documentation Committee (IKDC) 2000 Knee Evaluation Form, Lysholm score; instrumented knee testing was performed with the arthrometer (KT 2000). Statistical analysis was performed to compare the preoperative and postoperative objective evaluation.
Results: At 3 years followup, 31.6% patients were graded A, 65.8% were graded B and 2.6% was graded C at IKDC objective evaluation. Manual laxity tests, Lysholm’s score, mean side to side instrumental laxity and Tegner activity score improved significantly. 76% patients returned to preinjury level of sports activity after augmentation.
Conclusion: The results of anatomic single bundle augmentation in partial ACL tears are encouraging with excellent improvement in functional scores, side to side laxity and return to sports activity.
Similar content being viewed by others


References
Noyes FR, Bassett RW, Grood ES, Butler DL. Arthroscopy in acute traumatic hemarthrosis of the knee. Incidence of anterior cruciate tears and other injuries. J Bone Joint Surg Am 1980;62:687–95, 757.
Zantop T, Brucker PU, Vidal A, Zelle BA, Fu FH. Intraarticular rupture pattern of the ACL. Clin Orthop Relat Res 2007;454:48–53.
Jacquot L, Selmi TA, Servien E, Neyret P. Recent knee ligament injuries (Le’sions ligamentaires re’centes du genou) (article in french). EMC (Elsevier Masson SAS, Paris), Musculoskeletal, 14-080-A-20, 2003: page 20.
Liljedahl SO, Lindvall N, Wetterfors J. Early diagnosis and treatment of acute ruptures of the anterior cruciate ligament; a clinical and arthrographic study of forty-eight cases. J Bone Joint Surg Am 1965;47:1503–13.
Ochi M, Adachi N, Deie M, Kanaya A. Anterior cruciate ligament augmentation procedure with a 1 incision technique: Anteromedial bundle or posterolateral bundle reconstruction. Arthroscopy 2006;22:463. el-5.
Siebold R, Fu FH. Assessment and augmentation of symptomatic anteromedial or posterolateral bundle tears of the anterior cruciate ligament. Arthroscopy 2008;24:1289–98.
Sonnery-Cottet B, Lavoie F, Ogassawara R, Scussiato RG, Kidder JF, Chambat P. Selective anteromedial bundle reconstruction in partial ACL tears: A series of 36 patients with mean 24 months followup. Knee Surg Sports Traumatol Arthrosc 2010;18:47–51.
Bak K, Scavenius M, Hansen S, Norring K, Jensen KH, Jorgensen U. Isolated partial rupture of the anterior cruciate ligament. Long term followup of 56 cases. Knee Surg Sports Traumatol Arthrosc 1997;5:66–71.
Buckley SL, Barrack RL, Alexander AH. The natural history of conservatively treated partial anterior cruciate ligament tears. Am J Sports Med 1989;17:221–5.
Barrack RL, Buckley SL, Bruckner JD, Kneisl JS, Alexander AH. Partial versus complete acute anterior cruciate ligament tears. The results of nonoperative treatment. J Bone Joint Surg Br 1990;72:622–4.
Noyes FR, Mooar LA, Moorman CT 3rd, McGinniss GH. Partial tears of the anterior cruciate ligament. Progression to complete ligament deficiency. J Bone Joint Surg Br 1989;71:825–33.
Fruensgaard S, Johannsen HV. Incomplete ruptures of the anterior cruciate ligament. J Bone Joint Surg Br 1989;71:526–30.
Danylchuk KD, Finlay JB, Krcek JP. Microstructural organization of human and bovine cruciate ligaments. Clin Orthop Relat Res 1978;131:294–8.
Delincé P, Krallis P, Descamps PY, Fabeck L, Hardy D. Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869–76.
Smith DB, Carter TR, Johnson DH. High failure rate for electrothermal shrinkage of the lax anterior cruciate ligament: A multicenter followup past 2 years. Arthroscopy 2008;24:637–41.
Chen J, Chen S, Weitao Z, Yinghui H, Yunxia L. Technique of arthroscopic anterior cruciate ligament reconstruction with preserved residual fibers as a graft envelope. Tech Knee Surg 2008;7:70–7.
Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br 1961;43:752–7.
Sabat D, Kumar V. Nerve injury during hamstring graft harvest: A prospective comparative study of three different incisions. Knee Surg Sports Traumatol Arthrosc 2013;21:2089–95.
van Eek CF, Schreiber VM, Liu TT, Fu FH. The anatomic approach to primary, revision and augmentation anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 2010;18:1154–63.
Van Dyck P, Vanhoenacker FM, Gielen JL, Dossche L, Van Gestel J, Wouters K, et al. Three tesla magnetic resonance imaging of the anterior cruciate ligament of the knee: Can we differentiate complete from partial tears? Skeletal Radiol 2011;40:701–7.
Van Dyck P, De Smet E, Veryser J, Lambrecht V, Gielen JL, Vanhoenacker FM, et al. Partial tear of the anterior cruciate ligament of the knee: Injury patterns on MR imaging. Knee Surg Sports Traumatol Arthrosc 2012;20:256–61.
Sonnery-Cottet B, Chambat P. Arthroscopic identification of the anterior cruciate ligament posterolateral bundle: The figure-of-four position. Arthroscopy 2007;23:1128.e1-3.
Borbon CA, Mouzopoulos G, Siebold R. Why perform an ACL augmentation? Knee Surg Sports Traumatol Arthrosc 2012;20:245–51.
Liu W, Maitland ME, Bell GD. A modeling study of partial ACL injury: Simulated KT-2000 arthrometer tests. J Biomech Eng 2002;124:294–301.
Crain EH, Fithian DC, Paxton EW, Luetzow WF. Variation in anterior cruciate ligament scar pattern: Does the scar pattern affect anterior laxity in anterior cruciate ligament-deficient knees? Arthroscopy 2005;21:19–24.
Bray RC, Leonard CA, Salo PT. Vascular physiology and long term healing of partial ligament tears. J Orthop Res 2002;20:984–9.
Buda R, Ferruzzi A, Vannini F, Zambelli L, Di Caprio F. Augmentation technique with semitendinosus and gracilis tendons in chronic partial lesions of the ACL: Clinical and arthrometric analysis. Knee Surg Sports Traumatol Arthrosc 2006;14:1101–7.
Ochi M, Adachi N, Uchio Y, Deie M, Kumahashi N, Ishikawa M, et al. A minimum 2-year followup after selective anteromedial or posterolateral bundle anterior cruciate ligament reconstruction. Arthroscopy 2009;25:117–22.
Serrano-Fernandez JM, Espejo-Baena A, Martin-Castilla B, De La Torre-Solis F, Mariscal-Lara J, Merino-Ruiz ML. Augmentation technique for partial ACL ruptures using semitendinosus tendon in the over-the-top position. Knee Surg Sports Traumatol Arthrosc 2010;18:1214–8.
Chouteau J, Testa R, Viste A, Moyen B. Knee rotational laxity and proprioceptive function 2 years after partial ACL reconstruction. Knee Surg Sports Traumatol Arthrosc 2012;20:762–6.
Lee BI, Kwon SW, Kim JB, Choi HS, Min KD. Comparison of clinical results according to amount of preserved remnant in arthroscopic anterior cruciate ligament reconstruction using quadrupled hamstring graft. Arthroscopy 2008;24:560–8.
Sonnery-Cottet B, Panisset JC, Colombet P, Cucurulo T, Graveleau N, Hulet C, et al. Partial ACL reconstruction with preservation of the posterolateral bundle. Orthop Traumatol Surg Res 2012;98 8 Suppl 1:S165–70.
Yoon KH, Bae DK, Cho SM, Park SY, Lee JH. Standard anterior cruciate ligament reconstruction versus isolated single-bundle augmentation with hamstring autograft. Arthroscopy 2009;25:1265–74.
Demirag B, Ermutlu C, Aydemir F, Durak K. A comparison of clinical outcome of augmentation and standard reconstruction techniques for partial anterior cruciate ligament tears. Eklem Hastalik Cerrahisi 2012;23:140–4.
Pujol N, Colombet P, Potel JF, Cucurulo T, Graveleau N, Hulet C, et al. Anterior cruciate ligament reconstruction in partial tear: Selective anteromedial bundle reconstruction conserving the posterolateral remnant versus single-bundle anatomic ACL reconstruction: Preliminary 1-year results of a prospective randomized study. Orthop Traumatol Surg Res 2012;98 8 Suppl:S171–7.
Maestro A, Suarez-Suarez MA, Rodrfguez-López L, Villa-Vigil A. Stability evaluation after isolated reconstruction of anteromedial or posterolateral bundle in symptomatic partial tears of anterior cruciate ligament. Eur J Orthop Surg Traumatol 2013;23:471–80.
Adachi N, Ochi M, Uchio Y, Sumen Y. Anterior cruciate ligament augmentation under arthroscopy. A minimum 2-year followup in 40 patients. Arch Orthop Trauma Surg 2000;120:128–33.
Park SY, Oh H, Park SW, Lee JH, Lee SH, Yoon KH. Clinical outcomes of remnant-preserving augmentation versus double-bundle reconstruction in the anterior cruciate ligament reconstruction. Arthroscopy 2012;28:1833–41.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sabat, D., Kumar, V. Partial tears of anterior cruciate ligament: Results of single bundle augmentation. IJOO 49, 129–135 (2015). https://doi.org/10.4103/0019-5413.152394
Published:
Issue Date:
DOI: https://doi.org/10.4103/0019-5413.152394
Key words
- Anteromedial bundle
- partial anterior cruciate ligament tear
- posterolateral bundle
- selective augmentation