
Abstract
Abstract
DTaP3-CB (Triacelluvax™)1. is an acellular pertussis (aP) vaccine containing 3 antigens from purified Bordetella pertussis bacteria combined with diphtheria and tetanus toxoids (DT). In addition to purified filamentous haemagglutinin and pertactin, DTaP3-CB contains pertussis toxin which has been genetically rather than chemically detoxified.
As shown in randomised, double-blind clinical trials in infants, DTaP3-CB elicits an immune response similar to or greater than that of whole cell (DTwP) vaccines. Results of a large multicentre study comparing DTaP3-CB with 12 acellular and 1 DTwP vaccine indicate that DTaP3-CB, like all acellular vaccines, induces variable immune responses to different pertussis antigens; however, antibody titres to pertussis toxin are normally higher after immunisation with the genetically detoxified vaccine than with other 3- or 4-component vaccines. When given as a fourth or fifth booster dose, DTaP3-CB produced a significant immune response in infants primed with 3 doses of either a DTaP or DTwP vaccine. Virtually all infants immunised with DTaP3-CB had a serological response to diphtheria and tetanus toxoids.
Data from 2 very large efficacy studies indicate that DTaP3-CB has high and long lasting protective efficacy against culture-confirmed pertussis which is greater than that of a 2-component vaccine (DTaP2-SB) and the whole cell DTwP-CON vaccine after a 3-, 5- and 12-month immunisation schedule and after a 2-, 4- and 6-month schedule with the DTwP-CON vaccine. However, the DTwP-CON whole cell vaccine has been noted for its low immunogenicity in 1 study and low efficacy and immunogenicity in another study. On the other hand, DTaP3-CB vaccine has similar efficacy to DTaP3-SB (after immunisation at 2, 4 and 6 months), DTaP5-CON and DTwP-EVANS against culture-confirmed pertussis with ≥21 days cough in infants immunised according to a 3-, 5- and 12-month schedule.
Infants immunised with DTaP3-CB experienced significantly fewer adverse events such as pain, redness, swelling and irritability than infants given DTwP. DTaP3-CB has a similar tolerability profile to other acellular vaccines and is associated with similar rates of local tenderness, irritability, fever (≥40°C) and persistent crying. Comparative trials have shown that infants immunised with DTaP3-CB had a lower incidence of pain at the site of injection and fever (≥38°C) compared with other acellular vaccines, although this may have little clinical significance.
Concomitant administration of DTaP3-CB with hepatitis B, oral polio or Haemophilus influenzae type B vaccines did not affect the immunogenicity of these other paediatric vaccines.
Conclusion: Data from clinical trials with DTaP3-CB vaccine indicate that this vaccine induces high and long lasting efficacy. It is at least as efficacious as most whole cell vaccines and generally similar in efficacy to the most efficacious acellular pertussis vaccines containing 3 or more pertussis antigens. DTaP3-CB is better tolerated than whole cell vaccines and has a similar tolerability profile to other acellular vaccines; the possible lower risk of severe adverse events remains to be confirmed. The low reactogenicity of DTaP3-CB is likely to make it well tolerated and therefore well accepted for the immunisation of infants, thereby enabling wider implementation of vaccination programmes.
Immunogenicity
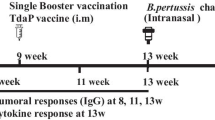
The immunogenicity of the diphtheria-tetanus-acellular pertussis (DTaP) vaccine, DTaP3-CB (Triacelluvax™)1 has been compared with that of whole cell pertussis (DTwP) and chemically detoxified acellular vaccines in several randomised, double-blind clinical trials. Infants were generally immunised at 2, 4 and 6 months of age and then in 3 further studies given a fourth booster dose at 15 to 20 months and in 1 study given a fifth booster dose at 4 to 6 years.
The immunogenicity of DTaP3-CB vaccine was similar to the whole cell vaccine DTwP-EVANS and greater than that of whole cell vaccines DTwP-CB, DTwP-CON and DTwP-LP Geometric mean titres (GMT) for DTaP3-CB were significantly higher for all 3 pertussis antigens [pertussis toxin (PT), filamentous haemaglutinin (FHA) and pertactin] when compared with DTwP-CON and DTwP-CB and significantly higher for the pertussis FHA antigen when compared with DTwP-LP.
Immunogenicity varied considerably among acellular vaccines with no single vaccine being the most or least immunogenic for all pertussis antigens in a US study comparing 13 vaccines. DTaP3-CB had significantly higher GMT to PT than most acellular vaccines, despite a lower antigen concentration. Conversely, GMT to FHA and pertactin, normally lower compared to other acellular vaccines, were consistent, in this case, with the lower antigen concentration for these 2 antigens in the DTaP3-CB vaccine. At least 95% of infants immunised with DTaP3-CB had serological responses to at least 1 antigen.
DTaP3-CB vaccine induced high level cell-mediated immune response to at least 1 of the 3 pertussis antigen components in the vaccine in the majority of infants (83%) 1 month after the third immunisation.
Infants immunised with DTaP3-CB had similar rates of serological response to diphtheria and tetanus toxoids compared with children given the diphtheria and tetanus vaccine alone.
DTaP3-CB was highly immunogenic when administered to 15- to 20-month-old infants primed with 3 doses of either DTaP3-CB or a whole cell vaccine. Similar results were noted when DTaP3-CB was administered as a fifth booster dose to 4- to 6-year-old children previously immunised with 3 primary doses and a fourth booster dose of DTaP3-CB.
DTaP3-CB acellular vaccine was administered concomitantly with the hepatitis B vaccine (HBV) and had no effect on the immunogenicity of HBV in a subset of 1237 infants enrolled in the Italian pertussis efficacy trial (n = 15 601). Similar results were seen in other trials for the oral polio virus (OPV) and Haemophilus influenzae (Hib) vaccines, which are normally administered concomitantly with acellular pertussis vaccines in infants.
Protective Efficacy
DTaP3-CB vaccine efficacy was 84% for infants followed for approximately 18 months beginning 1 month after a third vaccine dose in the randomised double-blind DT-controlled, phase III Italian efficacy trial (n = 15 601). In the randomised, double-blind, Swedish efficacy trial DTaP3-CB vaccine showed similar efficacy to DTaP3-SB, DTaP5-CON and DTwP-EVANS and was more effective than DTaP2-SB and DTwP-CON in preventing culture-confirmed pertussis infection. However, the DTwP-CON whole cell vaccine has been noted for its low immunogenicity in 1 study and low immunogenicity and protective efficacy in another study. When all cases of pertussis were included irrespective of cough duration, DTaP3-CB was less effective than DTaP5-CON and DTwP-EVANS.
As shown in the extended follow-up of the Italian efficacy trial, children immunised with 3 doses of DTaP3-CB at 2, 4 and 6 months are still protected at approximately 3 years of age. This extended follow-up also demonstrated that the cumulative vaccine efficacy was slightly greater for 4302 infants immunised with DTaP3-CB (86%) than for 4327 infants immunised with DTaP3-SB (81%).
Tolerability
Adverse events commonly reported after administration of DTaP3-CB vaccine in 2- to 6-month-old infants are swelling and tenderness at the injection site, irritability and fever (>38°C). However, these rates are markedly lower than those in infants immunised with whole cell pertussis vaccines. In a phase II trial performed in Italy, 240 infants immunised with DTaP3-CB had significantly lower rates of fever (>38°C), mild fretfulness and redness, swelling and pain 48 hours after immunisation than 240 infants immunised with DTwP-CB.
The incidence of adverse events varied among acellular vaccines, with no vaccine being the most or least reactogenic for all symptoms. However, comparative trials have shown that infants immunised with DTaP3-CB had a lower incidence of pain at the site of injection and fever (≥38°C) compared with other acellular vaccines, although this may not be clinically significant.
More severe adverse reactions such as fever (>39°C), persistent crying, redness and swelling >1cm and moderate pain were uncommon in infants vaccinated with DTaP3-CB.
As far as serious reactions are concerned, infants vaccinated with DTaP3-CB in a large Swedish efficacy trial (n = 72 698) produced lower relative risk estimates for convulsions within 48 hours and hypotonic-hyporesponsive episodes 72 hours after vaccination than those given DTaP2-SB and DTaP5-CON vaccines.
DTaP3-CB is generally well tolerated as a fourth and fifth booster dose in children aged 15 to 20 months and 4 to 6 years of age.
Dosage and Administration
DTaP3-CB is available as a trivalent vaccine in combination with diphtheria and tetanus toxoids and is administered as an intramuscular injection into the thigh or buttock. The recommended vaccination schedule in infants aged ≥6 weeks consists of 3 doses given at 2, 4 and 6 months of age, or alternatively at 3, 5 and 12 months. A fourth booster dose is recommended at 12 to 24 months of age depending on the primary immunisation schedule, and another booster at 4 to 6 years. DTaP3-CB can be given as a booster dose in infants previously immunised with either 3 doses of the DTaP3-CB or a whole cell vaccine. DTaP3-CB can be administered concomitantly but at a different injection site with Hib, HBV, measles, mumps and rubella (MMR) or OPV vaccines. To date no data has been reported on the concomitant administration of DTaP3-CB and MMR vaccines.
Immunisation with DTaP3-CB is contraindicated if the infant is known to have a hypersensitivity to any of the vaccine components or has experienced encephalopathy within 7 days of a previous pertussis immunisation. Immunisation should be delayed if the infant has an acute febrile illness. As with any other vaccine, children should remain under medical supervision for at least 30 minutes after immunisation with DTaP3-CB.








Similar content being viewed by others

Notes
Use of trade name is for product identification purposes only, and does not imply endorsement.
References
Rappuoli R. Acellular pertussis vaccines: a turning point in infant and adolescent vaccination. Infect Agent Dis 1996 Jan; 5: 21–8
Wintermeyer SM, Nahata MC, Kyllonen KS. Whole-cell and acellular pertussis vaccines. Ann Pharmacother 1994 Jul-Aug; 28: 925–39
Boughton C. Whooping cough: new acellular pertussis vaccines. Curr Ther 1996 Sep; 37: 49–52
Trollfors B. Acute respiratory infections in children. Curr Opin Infect Dis 1994 Apr; 7: 157–61
Patel SS, Wagstaff AT. Acellular pertussis vaccine (Infanrix™ -DTPa; SB-3): a review of its immunogenicity, protective efficacy and tolerability in the prevention of Bordetella pertussis infection. Drugs 1996 Aug; 52: 254–75
Annunziato PW, Pichichero ME. New developments in pertussis vaccines. Clin Immunother 1995 Apr; 3: 287–96
Trollfors B, Taranger J. Towards better pertussis vaccines. Ann Med 1997 Apr; 29: 87–9
Higgins G. Whole-cell DTP vaccines make way for new wave of acellular products. Inpharma 1996 Aug 10; 1049: 3–4
Edwards KM, Meade BD, Decker MD, et al. Comparison of 13 acellular pertussis vaccines: overview and serologic response. Pediatrics 1995 Sep; 96 (Pt 2): 548–57
Edwards KM. Acellular pertussis vaccines:- a solution to the pertussis problem. J Infect Dis 1993; 168(1): 15–20
American Academy of Pediatrics. Acellular pertussis vaccine: recommendations for use as the inital series in infants and children. Pediatrics 1997; 99(2): 282–8
Olin P, Rasmussen F, Gustafsson L, et al. Randomised controlled trial of two-component, three-component, and five-component acellular pertussis vaccines compared with whole-cell pertussis vaccine. Lancet 1997 Nov 29; 350: 1569–77
Podda A, De Luca EC, Contu B, et al. Comparative study of a whole-cell pertussis vaccine and a recombinant acellular pertussis vaccine. J Pediatr 1994 Jun; 124: 921–6
Black SB, Shinefield HR, Bergen R, et al. Safety and immunogenicity of Chiron/Biocine® recombinant acellular pertussis-diphtheria-tetanus vaccine in infants and toddlers. Pediatr Infect Dis J 1997 Jan; 16: 53–8
Santos OP, Madrid B, Di ME, et al. Immunogenicity in Filipino infants of the Biocine® acellular pertussis vaccine containing the genetically detoxified pertussis toxin molecule [abstract]. 7th International Congress for Infectious Diseases; 1996 Jun 10; Hong Kong, 314–5
Cassone A, Ausiello CM, Urbani F, et al. Cell-mediated and antibody responses to Bordetella pertussis anitgens in children vaccinated with acellular or whole-cell pertussis vaccines. Arch Pediatr Adolesc Med 1997 Mar; 151: 283–9
Greco D, Salmaso S, Mastrantonio P, et al. A controlled trial of two acellular vaccines and one whole-cell vaccine against pertussis. N Engl J Med 1996 Feb 8; 334: 341–8
Olin P, Hallander HO, Gustafsson L, et al. Measuring protection; a case study of pertussis vaccines-Swedish trial II: secondary non-randomized comparisons between two schedules of infant vaccination. In: Plotkin S, Brown F, Horaud F, editors. Preclinical and clinical development of new vaccines. Dev Biol Stand. Vol. 95. Basel: Karger, 1998: 211–20
Podda A, Bona G, Canciani G, et al. Effect of priming with diphtheria and tetanus toxoids combined with whole-cell pertussis vaccine or with acellular pertussis vaccine on the safety and immunogenicity of a booster dose of an acellular pertussis vaccine containing a genetically inactivated pertussis toxin in fifteen-to twenty-one-month-old children. J Pediatr 1995 Aug; 127: 238–43
Pichichero ME, Deloria MA, Rennels MB, et al. A safety and immunogenicity comparison of 12 acellular pertussis vaccines and one whole-cell pertussis vaccine given as a fourth dose in 15- to 20-month-old children. Pediatrics 1997 Nov; 100: 772–88
Pizza M, Covacci A, Bartoloni A, et al. Mutants of pertussis toxin suitable for vaccine development. Science 1989; 246: 497–500
Nencioni L, Pizza MG, Bugnoli M, et al. Characterization of genetically inactivated pertussis toxin mutants: candidates for a new vaccine against whooping cough. Infect Immun 1990; 58(5): 1308–15
Meade BD, Deforest A, Edwards KM, et al. Description and evaluation of serologic assays used in a multicenter trial of acellular pertussis vaccines. Pediatrics 1995 Sep; 96 (Pt 2): 570–5
Podda A, Mokatrin A, Phillips L. Immunogenicity of concomittant vaccines administered during biocine DTaP clinical trials. Emeryville (CA): Chiron Biocine.1996 (Data on file)
Giuliano M, Mastrantonio P, Giammanco A, et al. Antibody responses and persistence in the two years after immunization with two acellular vaccines and one whole-cell vaccine against pertussis. J Pediatr 1998 Jun; 132: 983–8
Miller J, Silverberg R, Saito T, et al. An agglutinative reaction for Haemophilus pertussis. J Pediatr 1943; 22: 644–51
Pichichero M, Edwards K, Anderson E, et al. Safety and immunogenicity of six acellular pertussis vaccines and one whole-cell pertussis vaccine given as a fifth dose in four-to six-year old children. Pediatrics 2000; 105(1): ell
Salmaso S, Piscitelli A, Rapicetta M, et al. Immunogenicity of hepatitis B vaccines among infant recipients of acellular and whole cell pertussis DTP vaccines. Vaccine 1998 Apr; 16: 643–6
Podda A. Marketing Authorisation Application Triacelluvax™. Clinical Expert Report. Overall Clinical Summary. Siena (Italy): Chiron Biocine, 1997 (Data on file)
Greco D. Covariates for safety and immune responses to pertussis vaccinations in the Italian trial [abstract]. 7th International Congress for Infectious Diseases; 1996 10 Jun; Hong Kong; 1–2
Salmaso S, Mastrantonio P, Wassilak SGF, et al. Persistence of protection through 33 months of age provided by immunization in infancy with two three-component acellular pertussis vaccines. Vaccine 1998 Aug; 16: 1270–5
Black S, Shinefield H, Ray P, et al. Safety of Biocine DTaP vaccine in infancy [abstract]. Pediatr Res 1994 Apr; 35 (Pt 2): 174A
Christy C, Pichichero ME, Reed GF, et al. Effect of gender, race, and parental education on immunogenicity and reported reactogenicity of acellular and whole-cell pertussis vaccines. Pediatrics 1995 Sep; 96 (Pt 2): 584–7
Decker MD, Edwards KM, Steinhoff MC, et al. Comparison of 13 acellular pertussis vaccines: adverse reactions. Pediatrics 1995 Sep; 96 (Pt 2): 557–66
Tozzi AE, Ciofi degli-A ML, Wassilak SGF, et al. Predictors of adverse events after the administration of acellular and whole-cell diphtheria-tetanus-pertussis vaccines. Vaccine 1998 Jan-Feb; 16: 320–2
Pichichero ME. Acellular pertussis vaccines: towards an improved safety profile. Drug Saf 1996 Nov; 15: 311–24
Rosenthal S, Chen R, Hadler S. The safety of acellular pertussis vaccine vs whole-cell pertussis vaccine: a postmarketing assessment. Arch Pediatr Adolesc Med 1996 May; 150: 457–60
Deloria MA, Blackwelder WC, Decker MD, et al. Association of reactions after consecutive acellular or whole-cell pertussis vaccine immunizations. Pediatrics 1995 Sep; 96 (Pt 2): 592–4
Rennels MB, Deloria MA, Pichichero ME, et al. Entire thigh swelling after 4th dose of 10 different DTaP vaccines: relationship to other reactions and to vaccine contents [abstract]. Pediatr Res 1998 Apr; 43 (Pt 2): 156
Chiron S.p.A. Summary of Product characteristics. Siena (Italy): Chiron Biocine, 1997 (Data on file)
Weigl JAI, Bock HL, Clemens R, et al. Safety and efficacy of acellular pertussis vaccines: the Mainz Study and other recent studies. Ann Acad Med Singapore 1997 May; 26: 320–5
Lopez AL, Blumberg DA. An overview of the status of acellular pertussis vaccines in practice. Drugs 1997 Aug; 54: 189–96
Griffith AH. Permanent brain damage and pertussis vaccination: is the end of the saga in sight? Vaccine 1989; 7(3): 199–210
Cowan LD, Griffin MR, Howson CP, et al. Acute encephalopathy and chronic neurological damage after pertussis vaccine. Vaccine 1993 Nov; 11: 1371–9
Gangarosa EJ, Galazka AM, Wolfe CR, et al. Impact of anti-vaccine movements on pertussis control: the untold story. Lancet 1998 Jan 31; 351: 356–61
Podda A, De Luca EC, Titone L, et al. Acellular pertussis vaccine composed of genetically inactivated pertussis toxin: safety and immmunogenicity in 12- to 24- and 2- to 4-month old children. J Pediatr 1992; 120(5): 680–5
Kosecka U, Marshall JS, Crowe SE, et al. Pertussis toxin stimulates hypersensitivity and enhances nerve-mediated antigen uptake in rat intestine. Am J Physiol 1994; 267 (5 Pt 1): G745–53
Munoz JJ, Peacock MG, Hadlow WJ. Anaphylaxis or so-called encephalopathy in mice sensitized to an antigen with the aid of pertussigen (pertussis toxin). Infect Immun 1987; 55(4): 1004–8
Bonati M, Tamburlini G. Components of acellular pertussis vaccines [letter]. Lancet, 1996 Mar 16; 347: 764–5
Gustafsson L, Hallander HO, Olin P. A controlled trial of a two-component acellular, a five-component acellular, and a whole-cell pertussis vaccine. N Engl J Med 1996 Feb 8; 334: 349–55
Author information
Authors and Affiliations
Corresponding author
Additional information
Various sections of the manuscript reviewed by: S. Black, Pediatric Vaccine Study Group, Kaiser Permanente Medical Center, Oakland, California, USA; A. Cassone, Department of Bacteriology and Medical Mycology, Instituto Superiore di Sanita, Rome, Italy; K. Edwards, Department of Pediatrics, Vanderbilt University Medical School, Nashville, Tennessee, USA; S. Halperin, Department of Pediatrics, Dalhousie University, Halifax, Nova Scotia, Canada; M. Pichichero, Division of Infectious Diseases, The Strong Childrens Medical Center, New York, USA; S. Slamaso, Laboratory of Epidemiology and Biostatistics, Instituto Superiore di Sanita, Rome, Italy.
Data Selection
Sources: Medical literature published in any language since 1966 on diphtheria-tetanus-acellular-pertussis vaccine, identified using AdisBase (a proprietary database of Adis International, Auckland, New Zealand) and Medline. Additional references were identified from the reference lists of published articles. Bibliographical information, including contributory unpublished data, was also requested from the company developing the drug.
Search strategy: AdisBase search terms were ‘Diphtheria-tetanus-acellular-pertussis-vaccine’. Medline search terms were ‘Diphtheria-tetanus-acellular-pertussis-vaccine in children. Searches were last updated 11 February 2000.
Selection: Studies in children who were immunised with diptheria-tetanus-acellular-pertussis vaccine-Chiron/Biocine. Inclusion of studies was based mainly on the methods section of the trials. When available, large, well controlled trials with appropriate statistical methodology were preferred.
Index terms: diphtheria-tetanus-acellular-pertussis vaccine, pertussis, diphtheria, tetanus, immunisation, children, therapeutic use.
Rights and permissions
About this article
Cite this article
Matheson, A.J., Goa, K.L. Diphtheria-Tetanus-Acellular Pertussis Vaccine Adsorbed (Triacelluvax™; DTaP3-CB). Pediatr-Drugs 2, 139–159 (2000). https://doi.org/10.2165/00148581-200002020-00007
Published:
Issue Date:
DOI: https://doi.org/10.2165/00148581-200002020-00007