
Summary
Synopsis
Trandolapril is a non-sulfhydryl prodrug which, after oral administration, is hydrolysed in the liver to its active diacid, trandolaprilat. Trandolaprilat inhibits the angiotensin converting enzyme (ACE) and displays similar pharmacodynamic properties to other ACE inhibitors, improving haemodynamic and cardiac parameters in patients with essential hypertension.
Trandolapril 2 to 4mg once daily effectively controls blood pressure for at least 24 hours in patients with mild to moderate hypertension. In a small number of double-blind comparative trials, trandolapril had similar antihypertensive efficacy to that of atenolol, enalapril, hydrochlorothiazide, lisinopril and sustained release nifedipine, but was more effective than captopril. Combined therapy with trandolapril and hydrochlorothiazide or sustained release nifedipine had a significantly greater antihypertensive effect than either drug treatment alone. Further comparative trials are warranted to confirm these preliminary findings.
The tolerability profile of trandolapril is similar to that of other ACE inhibitors, most adverse events being generally mild and transient in nature, and trandolapril lacks adverse effects on carbohydrate and lipid metabolism.
Thus, trandolapril, with its favourable pharmacological profile and antihypertensive activity similar to that of agents currently used to treat patients with mild to moderate hypertension, is likely to provide a well tolerated option for the treatment of this disease. The results of ongoing and future clinical trials will determine its potential as a cardioprotective agent in patients following myocardial infarction.
Pharmacodynamic Properties
Trandolaprilat showed high affinity for angiotensin converting enzyme (ACE) in in vitro and ex vivo studies, in which it was a more potent inhibitor of this enzyme than quinaprilat, enalaprilat and captopril. In normotensive and hypertensive individuals, single oral doses of trandolapril ≥2mg inhibited plasma ACE activity by 85 to 100% within 2 to 4 hours of administration.
Trandolapril increased total and active plasma renin levels in normotensive and hypertensive individuals, whereas plasma aldosterone levels were generally reduced.
A single dose of trandolapril effectively reduced systolic and diastolic blood pressure throughout a 24-hour postdose period in patients with essential hypertension. Multiple-dose administration (1 to 8 mg/day for up to 12 months) provided satisfactory blood pressure control, while having little or no effect on heart rate, cardiac output or stroke volume. Significant reductions in left ventricular mass index, interventricular septal and posterior wall thicknesses, and afterload were observed during long term treatment (6 to 12 months), as was an improvement in left ventricular contractility and arterial compliance in patients with essential hypertension and left ventricular hypertrophy. Trandolapril 1 mg/day caused a similar reduction in left ventricular mass to that produced by enalapril 10 mg/day after 6 months.
Long term trandolapril administration significantly prolonged survival in animal models of hypertension and congestive heart failure, and the formation of vascular fibrinoid necrosis and occurrence of stroke were both prevented by trandolapril in spontaneously hypertensive stroke-prone rats.
Trandolapril 2 mg/day for 2 months reduced renal plasma flow (13%), without significantly altering renal vascular resistance, and a dose of 0.5 to 2.5 mg/day for 2 to 8 weeks had no significant effect on renal perfusion rate or plasma levels of creatinine or uric acid in hypertensive patients. No adverse effects on carbohydrate or lipid metabolism were observed in healthy volunteers or patients with essential hypertension with or without non-insulin-dependent diabetes.
Pharmacokinetic Properties
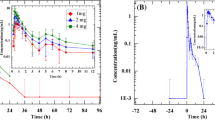
After oral administration, trandolapril is rapidly absorbed and converted to its active diacid, trandolaprilat, by nonspecific hydrolysis in the liver. Peak plasma concentrations (Cmax) of trandolapril in healthy volunteers were reached in approximately 1 hour (tmax), whereas tmax for trandolaprilat was about 4 to 6 hours. Cmax values were dose-proportional. After a single 2mg dose values ranged between 1.7 and 2.9 μg/L for trandolapril and 2.5 and 2.9 μg/L for trandolaprilat. Cmax values for trandolapril and trandolaprilat appeared higher in patients with mild to moderate hypertension after a single 2mg dose, but were similar to values in healthy volunteers during multiple-dose administration (1 to 2mg once daily for up to 10 days). Steady-state was achieved after 4 days and modest drug accumulation (accumulation index 1.5 to 2) was evident during therapy for 7 to 10 days.
While the absolute bioavailability of trandolapril after a single oral 2mg dose was only 9.5%, that of trandolaprilat was 40 to 60%, suggesting adequate absorption. Concomitant food intake reduced the rate of trandolapril absorption, but did not affect its bioavailability, or that of trandolaprilat.
Approximately 82% of a radiolabelled dose of trandolapril is excreted within 48 hours: about 33% in urine and 66% in faeces. Excretion is accounted for by trandolapril (negligible in urine) and trandolaprilat, their glucuronide conjugates and inactive diketopiperazine derivatives. The mean elimination half-life of trandolapril is about 0.7 to 1.3 hours, while trandolaprilat shows a biphasic elimination pattern, the prolonged terminal elimination phase (16 to 24 hours) probably representing the strong binding of trandolaprilat to ACE. Impaired renal function decreases the excretion of trandolaprilat, and hepatic impairment may decrease excretion of both trandolapril and trandolaprilat. Thus, initial dosage reduction is recommended in patients with severe renal or hepatic impairment. The dosage may then be increased as necessary to achieve a therapeutic response.
Therapeutic Use
In noncomparative and placebo-controlled studies, trandolapril 0.5 to 8 mg/day for 2 weeks and up to 12 months significantly reduced blood pressure in patients with mild to moderate hypertension. Maximal blood pressure reduction was achieved with a single daily dose of trandolapril 2mg and the antihypertensive effect was maintained for 12 months in patients treated with trandolapril 2 or 4 mg/day. The addition of a thiazide diuretic or calcium antagonist improved the response rate in a further 13% of patients not showing a satisfactory response to monotherapy with trandolapril.
The small number of double-blind comparative trials (mostly single comparisons) which have compared the antihypertensive efficacy of trandolapril (0.5 to 4 mg/day) with that of other ACE inhibitors and antihypertensive agents indicate that it is as effective as enalapril (2.5 to 20 mg/day) and lisinopril (10 mg/day), and more effective than captopril (100 mg/day) in reducing blood pressure to normalised levels (≤160/90mm Hg), or achieving a satisfactory blood pressure reduction (≥20/10mm Hg) in hypertensive patients. Trandolapril (2 to 4 mg/day) also appeared to be as effective as atenolol (100 to 200 mg/day), hydrochlorothiazide (25 mg/day) or sustained release nifedipine (40 mg/day), and antihypertensive activity was further enhanced during combined treatment with trandolapril and hydrochlorothiazide or sustained release nifedipine.
Trandolapril appeared equally effective in elderly (≥ 65 years) and younger hypertensive patients, as well as in obese hypertensive patients or those with glucose intolerance, non-insulin-dependent diabetes mellitus or renal dysfunction.
Tolerability
Trandolapril has been well tolerated in patients with mild to moderate hypertension in clinical trials of up to 12 months’ duration (> 2200 recipients), showing a similar adverse effect profile to that of other ACE inhibitors. The overall incidence of adverse events in a large multicentre study (n = 786) was 10.9%, cough being the most common (2.9%). Other adverse events included headache (1.9%), dizziness (1.8%), weakness (1.4%), palpitations (0.4%), hypotension (0.5%), nausea (0.6%), gastrointestinal disorders (0.5%), pruritus (0.4%) and rash (0.5%). Adverse events were generally mild and transient. However, treatment withdrawal due to severe events was necessary in 4.5% of patients in a large scale study (47/1049).
In large-scale comparative trials, trandolapril was at least as well tolerated as atenolol, enalapril, lisinopril and hydrochlorothiazide, and was better tolerated than captopril and sustained release nifedipine.
Dosage and Administration
In patients with mild to moderate hypertension, the recommended starting dosage of trandolapril is 2mg once daily. If necessary to achieve maximum response, this may be increased to 4mg once daily. In patients with severe renal or hepatic impairment, trandolapril should be initiated at a dosage of 0.5mg once daily.
Similar content being viewed by others


References
Dzau VJ. Circulating versus local renin-angiotensin system in cardiovascular homeostasis. Circulation 1988; 77 Suppl. 1: 14–7
Williams GH. Converting enzyme inhibitors in the treatment of hypertension. N Engl J Med 1988; 319 Suppl. 23: 1517–25
Bardelay C, Mach E, Worcel M, et al. Angiotensin-converting enzyme in rat brain and extraneural tissues visualized by quantitive autoradiography using 3H-trandolaprilate. J Cardiovasc Pharmacol 1989; 14: 511–8
Chevillard C, Jouquey S, Bree F, et al. Compared properties of trandolapril, enalapril and of their diacid metabolites. J Cardiovasc Pharmacol. In press
Hamon G, Jouquey S, Chevillard C, et al. Evidence that the prodrug trandolapril, a new ACE inhibitor, also displays a direct ACE inhibitory activity [abstract]. Br J Pharmacol 1992; 105 Suppl.: 201
Miyazaki M, Kawamoto T, Okunishi H, et al. Potent tissue angiotensin converting enzyme (ACE) inhibition and prolonged hypotensive effect of trandolapril (RU44570) [abstract]. J Hypertens 1992; 10 Suppl.: 277
Natoff IL, Redshaw S. Angiotensin-converting enzyme inhibitors — cilazapril and other bicyclic hexahydropyridazines. Drugs Future 1987; 12: 475–83
Vidal M, Vanhoutte PM. Endothelium-dependent effects of the converting enzyme inhibitor trandolapril [abstract no. 2410]. FASEB J 1988; 2
Illiano S, Mombouli JV, Nagao T, et al. Potentiation by trandolapril of the endothelium-dependent hyperpolarization induced by bradykinin. J Cardiovasc Pharmacol. In press
Vidal M, Joly G, Mombouli JV, et al. The endothelium and vascular effects of the angiotensin converting enzyme inhibitor trandolaprilat. J Cardiovasc Pharmacol. In press
Okunishi H, Kawamoto T, Kobayashi T, et al. Prolonged and tissue-selective inhibition of vascular angiotensin-converting enzyme by trandolapril: relevance to its antihypertensive action in spontaneously hypertensive rats. Pharm Pharmacol Lett 1992; 2: 180–3
Chevillard C, Brown NL, Mathieu M-N, et al. Compared effects of oral trandolapril and enalapril on tissue ACE activity in rats [abstract]. Fundam Clin Pharmacol 1987; 1: 369
Chevillard C, Brown NL, Mathieu M-N, et al. Differential effects of oral trandolapril and enalapril on rat tissue angiotensin-converting enzyme. Eur J Pharmacol 1988; 147: 23–8
Chevillard C, Brown NL, Jouquey S, et al. Cardiovascular actions and tissue-converting enzyme inhibitory effects of chronic enalapril and trandolapril treatment of spontaneously hypertensive rats. J Cardiovasc Pharmacol 1989; 14: 297–301
Brown NL, Badel M-Y, Benzoni F, et al. Angiotensin-converting enzyme inhibition, anti-hypertensive activity and hemodynamic profile of trandolapril (RU 44570). Eur J Pharmacol 1988; 148: 79–91
Sakonjo H, Nakanishi J-I, Fukuda Y, et al. Pharmacological action of a novel angiotensin converting enzyme (ACE) inhibitor, RU 44570, namely (−)-(2S,3aR,7aS)-l-[(S)-N-(S)-1-ethoxycarbonyl-3-phenylpropyl]alanyl]hexahydro-2-indolinecarboxylic acid: in vivo ACE inhibiting effect and antihypertensive effect in various hypertensive models of rats [in Japanese]. Pharmacometrics 1993; 45: 15–25
De Ponti F, Marelli C, D’Angelo L, et al. Pharmacological activity and safety of trandolapril (RU 44570) in healthy volunteers. Eur J Clin Pharmacol 1991; 40: 149–53
Mooser V, Nussberger J, Waeber B, et al. Enhanced activation of renin during repeated administration of the converting enzyme inhibitor RU-44570 [abstract]. Clin Pharmacol Ther 1988; 43: 180
Mooser V, Nussberger J, Juillerat L, et al. Reactive hyperreninemia is a major determinant of plasma angiotensin II during ACE inhibition. J Cardiovasc Pharmacol 1990; 15: 276–82
Patat A, Surjus A, Le Go A, et al. Safety and tolerance of single oral doses of trandolapril (RU 44.570), a new angiotensin converting enzyme inhibitor. Eur J Clin Pharmacol 1989; 36: 17–23
Yasuhara H, Kai K, Uchida E, et al. Phase I study of the RU 44570, an angiotensin-converting enzyme inhibitor (I). Single dose administration/food interaction in healthy volunteers [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 3–26
Arner P, Engfeldt P, Mouren M, et al. Pharmacokinetics and pharmacodynamics of a new once-daily ACE inhibitor trandolapril after repeated oral administration in patients with mild or moderate hypertension [abstract]. J Hypertens 1992; 10 Suppl.: 180
Arner P, Wade A, Engfeldt P, et al. Pharmacokinetics and pharmacodynamics of trandolapril after repeated administration of 2mg to young and older patients with mild-to-moderate hypertension. J Cardiovasc Pharmacol. In press
Kohno M, Horio T, Yokokawa K, et al. Acute effects of RU 44570 (trandolapril) on hemodynamic and endocrine responses during exercise in patients with essential hypertension [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 171–9
Bevan EG, Mclnnes GT, Aldigier JC, et al. Effect of renal function on the pharmacokinetics and pharmacodynamics of trandolapril. Br J Clin Pharmacol 1993; 35: 128–35
New horizons in antihypertensive therapy: Gopten (trandolapril). Ludwigshafen: Knoll AG, 1992
Lacourciere Y, Bourgeois J, Provencher P, et al. Antihypertensive effect of trandolapril administered once (OD) or twice daily (BID) on office and 24-hour ambulatory blood pressures [abstract]. J Hypertens 1992; 10 Suppl. 4: 254
Mancia G, De Cesaris R, Fogari R, et al. Evaluation of the antihypertensive effect of once-a-day trandolapril by 24-hour ambulatory blood pressure monitoring. Am J Cardiol 1992; 70: 60–6
Kownator S, Vaur L, Chevrier J, et al. Durée d’action clinique du trandolapril chez l’hypertendu léger à modéré [abstract]. Archives des Maladies du Coeur et des Vaisseaux 1992; 85: 64
De Luca N, Rosiello G, Lamenza F, et al. Reversal of cardiac and large artery structural abnormalities induced by long-term antihypertensive treatment with trandolapril. Am J Cardiol 1992; 70: 52D–9D
Guller B, Hall J, Reeves R. Cardiac effects of trandolapril in hypertension. Am Heart J 1993; 125: 1536–41
van Os JS, Woittiez AJJ. Efficacy of trandolapril in essential hypertension [abstract]. Neth J Med 1990; 37: A33
Leonetti G, Fogari R, Mazzola C, et al. Effects of blood pressure reduction with trandolapril and enalapril on left ventricular hypertrophy and exercise tolerance. J Hypertens 1993; 11 Suppl. 5: S356–7
Asmar RG, Benetos A, Darne BM, et al. Converting enzyme inhibition: dissociation between antihypertensive and arterial effects. J Hum Hypertens 1992; 6: 381–5
Giudicelli JF. ACE inhibition-induced survival prolongation and organ protection in SHR-SPS: dose effect relationship [abstract]. 15th Congress of the European Society of Cardiology; 1993 August 29: Nice
Richer C, Mulder P, Fornes P, et al. Long-term treatment with trandolapril opposes cardiac remodelling and prolongs survival after myocardial infarction in rats. J Cardiovasc Pharmacol 1992; 20: 147–56
Richer C, Doussau M-P, Giudicelli J-F. Systemic and regional hemodynamic profile of five angiotensin I converting enzyme inhibitors in the spontaneously hypertensive rat. Am J Cardiol 1987; 59: 12–7
Gaillard CA, van Es PN, de Leeuw PW. Disparate renal hemodynamic effects of trandolapril (T) and enalapril (E) in essential hypertensives (EH) [abstract]. Pharm World Sci 1993; 15: E4
Ito K, Kosugi Y, Nakagawa M, et al. Effect of RU 44570 (trandolapril) on renal function in patients with essential hypertension [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 181–90
Hidaka H, Watanabe T, Kurokawa K. Effect of RU 44570 (trandolapril) on the blood pressure and serum lipids in patients with essential hypertension [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 191–204
Predel H-G, Rohden C, Heine O, et al. Influence of the non-sulfhydryl angiotensin-converting enzyme inhibitor trandolapril on lipid and carbohydrate metabolism related to exercise capacity in healthy subjects. Am Heart J 1993; 125: 1532–5
Bauduceau B, Vaur L, Rezvani Y, et al. Action of trandolapril on blood glucose control and microalbuminuria in hypertensive diabetics [in French]. Ann Cardiol Angeiol 1994; 43: 84–8
Lenfant B, Mouren M, Bryce T, et al. Trandolapril: pharmacokinetics of single oral doses in male healthy volunteers. J Cardiovasc Pharmacol. In press
Mannhold R. Trandolapril. Drugs Today 1992; 28: 479–86
Danielson B, Querin S, Larochelle P, et al. Pharmacokinetics and pharmacodynamics of 2mg trandolapril after repeated administration to patients with chronic renal failure and to healthy subjects [abstract]. J Hypertens 1992; 10 Suppl. 4: 197
Danielson B, Querin S, LaRochelle P, et al. Pharmacokinetics and pharmacodynamics of trandolapril after repeated administration of 2mg to patients with chronic renal failure and healthy control subjects. J Cardiovasc Pharmacol. In press
Urae A, Urae R, Kagawa Y, et al. Phase I study of the RU 44570, an angiotensin-converting enzyme inhibitor (III). Pharmacokinetics and pharmacodynamics study in healthy volunteers [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 41–52
Yasuhara H, Kai K, Uchida E, et al. Phase I study of the RU 44570, an angiotensin-converting enzyme inhibitor (II). Multiple-dose administration in healthy volunteers [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 27–40
Lenfant B, Surjus A, Mouren M, et al. Effect of food on the bioavailability of trandolapril and its active metabolite trandolaprilat after oral administration to healthy volunteers [abstract]. J Hypertens 1992; 10 Suppl. 4: 258
Bree F, Nguyen P, Tillement JP, et al. How do trandolapril, a new ACE inhibitor, and trandolaprilat, the major and active metabolite, bind to human blood constituents? [abstract]. J Hypertens 1992; 10 Suppl. 4: 188
Wade A, Arner P, Sultan E, et al. Pharmacokinetics and pharmacodynamics of 2mg trandolapril after repeated administration in elderly patients with mild to moderate essential hypertension [abstract]. J Hypertens 1992; 10 Suppl. 4: 353
Hui KK, Duchin KL, Kripalani KJ, et al. Pharmacokinetics of fosinopril in patients with various degrees of renal function. Clin Pharmacol Ther 1991; 49: 457–67
Sica DA, Cutler RE, Oarmer RJ, et al. Comparison of the steady-state pharmacokinetics of fosinopril, lisinopril and enalapril in patients with chronic renal insufficiency. Clin Pharmacokinet 1991; 20: 420–7
Arakawa K, Iimura O, Abe K, et al. Efficacy and safety of RU 44570 (trandolapril), a novel angiotensin enzyme inhibitor, in patients with essential hypertension — multicenter open pilot study [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 65–77
Backhouse CI, Orofiamma B, Pauly NC. Long-term therapy with trandolapril, a new nonsulfhydryl ACE inhibitor, in hypertension: a multicenter international trial. J Cardiovasc Pharmacol. In press
Belcaro G, Cesarone MR, De Sanctis MT, et al. Evaluation and quantification of the microcirculatory effects of trandolapril in hypertensives by laser-doppler flowmetry [abstract]. J Hypertens 1992; 10 Suppl. 4: 183
Cesarone MR, De Sanctis G, Laurora G, et al. The effects of trandolapril on 24h ambulatory blood pressure in patients with mild to moderate essential hypertension [abstract]. J Hypertens 1992; 10 Suppl. 4: 1992
Iimura O, Abe K, Kuramoto K, et al. Clinical evaluation of RU44570 (trandolapril), a novel angiotensin converting enzyme inhibitor, in patients with severe hypertension [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 105–19
Poirier L, Bourgeois J, Lacourciere Y. Once-daily trandolapril compared with the twice-daily formulation in the treatment of mild to moderate hypertension: assessment by conventional and ambulatory blood pressures. J Clin Pharmacol 1993; 33: 832–6
Pauly NC, Safar ME. Placebo-controlled comparison of short-term efficacy and safety of 2, 4 and 8mg trandolapril in patients with mild to moderate hypertension — double-blind international mulitcentre trial [abstract]. J Hypertens 1992; 10 Suppl. 4: 299
De Bruijn JHB, Orofiamma BA, Pauly NC. Efficacy and tolerance of trandolapril (0.5 to 2mg) administered for 4 weeks in patients with mild-to-moderate hypertension. J Cardiovasc Pharmacol. In press
De Bruijn JHB, Pauly NC. Placebo controlled dose-ranging study of the efficacy and safety of 0.5, 1 and 2mg trandolapril in patients with mild to moderate hypertension — a double-blind multicentre international trial [abstract]. J Hypertens 1992; 10 Suppl. 4: 198
Pauly NC. Comparison of the efficacy and safety of trandolapril and captopril for 16 weeks in mild to moderate essential hypertension. J Cardiovasc Pharmacol. In press
Arakawa K, Saruta T, Iimura O, et al. Clinical evaluation of angiotensin converting enzyme inhibitor, trandolapril (RU 44570) in patients with essential hypertension — multi-centred double-blind comparative study in comparison with enalaprilat maleate [in Japanese]. Rinsho Hyoka 1992; 20: 477–511
de Leeuw PW, Pauly NC. Double-blind comparison of efficacy and safety of trandolapril 4mg and enalapril 20mg in patients with mild to moderate hypertension [abstract]. J Hypertens 1992; 10 Suppl. 4: 199
Meyer BH, Pauly NC. Double-blind comparison of efficacy and safety of trandolapril 2mg and hydrochlorothiazide 25mg in patients with mild to moderate essential hypertension. J Cardiovasc Pharmacol. In press
Steiner G, Pauly NC. Comparison of the efficacy and safety of trandolapril and nifedipine SR in mild-to-moderate hypertension. J Cardiovasc Pharmacol. In press
Pauly NC, Safar ME. Double-blind comparison of efficacy and safety of trandolapril 4mg and captopril 100mg in patients with mild to moderate essential hypertension [abstract]. J Hypertens 1992; 10 Suppl. 4: 299
Meyer BH, Pauly NC. Double-blind comparison of efficacy and safety of trandolapril 2mg and hydrochlorothiazide 25mg in patients with mild to moderate essential hypertension [abstract]. J Hypertens 1992; 10 Suppl. 4: 274
Arakawa K, Iimura O, Abe K, et al. Effect of RU 44570 (trandolapril), a novel angiotensin converting enzyme inhibitor, in patients with essential hypertension — monotherapy and combination therapy with thiazides [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 79–104
Arakawa K, Iimura O, Abe K, et al. Clinical evaluation of RU 44570 (trandolapril), a novel angiotensin converting enzyme inhibitor, in the long-term treatment of patients with essential hypertension [in Japanese]. Rinsho Iyaku 1992; 8 Suppl. 7: 141–69
Steiner G, Pauly NC. Double-blind comparison of efficacy and safety of trandolapril, nifedipine SR and their combination — a multicentre international trial [abstract]. J Hypertens 1992; 10 Suppl. 4: 330
Gaillard CA, de Leeuw PW. Clinical experiences with trandolapril. Am Heart J 1993; 125: 1542–6
Meyer BH, Muller FO, Heyns A du P, et al. Does trandolapril interact with warfarin? [abstract]. J Hypertens 1992; 10 Suppl. 4: 274
Meyer BH, Muller FO, Luus HG, et al. Pharmacokinetic interaction study between trandolapril, a new ACE inhibitor, and furosemide [abstract]. J Hypertens 1992; 10 Suppl. 4: 274
Patat A, Surjus A, Mouren M, et al. Is there a pharmacokinetic or pharmacodynamic interaction between trandolapril, a new ACE inhibitor and digoxin? [abstract]. J Hypertens 1992; 10 Suppl. 4: 299
Tremblay D, Patat A, Rey E, et al. Absence of interaction between trandolapril and nifedipine [abstract]. J Hypertens 1992; 10 Suppl. 4: 342
Berne C, Pollare T, Lithell H. Effects of antihypertensive treatment on insulin sensitivity with special reference to ACE inhibitors. Diabetes Care 1991; 14 Suppl. 4: 39–47
Black HR. Metabolic considerations in the choice of therapy for the patient with hypertension. Am Heart J 1991; 121: 707–15
Christlieb AR. Treatment selection considerations for the hypertensive diabetic patient. Arch Intern Med 1990; 150: 1167–74
Author information
Authors and Affiliations
Additional information
Various sections of the manuscript reviewed by: H.R. Brunner, Division d’Hypertension, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland; L. Burrell, Department of Medicine, University of Melbourne, Heidelberg, Victoria, Australia; P.W. de Leeuw, Department of Medicine, University Hospital Maastricht, Maastricht, The Netherlands; F. De Ponti, Department of Internal Medicine and Therapeutics, University of Pavia, Pavia, Italy; J-L. Freslon, Département de Pharmacodynamie, Université de Bordeaux II, Bordeaux, France; T. Ishizaki, Clinical Research Institute, National Medical Center, Tokyo, Japan; C.I. Johnson, Department of Medicine, University of Melbourne, Heidelberg, Victoria, Australia; T. Kawamoto, Department of Pharmacology, Osaka Medical College, Takatsuki, Japan; G.T. McInnes, University Department of Medicine and Therapeutics, Gardiner Institute, Western Infirmary, Glasgow, Scotland; T. Ogihara, Department of Geriatric Medicine, Osaka University Medical School, Osaka, Japan; H. Okunishi, Department of Pharmacology, Osaka Medical College, Takatsuki, Japan; P.A. Phillips, Department of Medicine, Austin and Repatriation Hospital, Heidelberg, Victoria, Australia; P. Sleight, Department of Cardiovascular Medicine, University of Oxford, Oxford, England; M.H. Weinberger, Hypertension Research Center, Indiana University, Indianapolis, Indiana, USA.
Rights and permissions
About this article
Cite this article
Wiseman, L.R., McTavish, D. Trandolapril. Drugs 48, 71–90 (1994). https://doi.org/10.2165/00003495-199448010-00007
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003495-199448010-00007