
Abstract
Objective
To synthesize and appraise economic evaluations of vision screening to detect vision impairment in children.
Methods
Literature searches were conducted on seven electronic databases, grey literature, and websites of agencies conducting health technology assessments. Studies were included if they (1) were full, comparative economic evaluations that used cost-utility, cost-benefit, cost-effectiveness, cost-consequence, or cost-analysis methods; (2) described screening services designed to detect amblyopia, strabismus, or uncorrected refractive errors in children under 6 years of age; and (3) published after 1994. High-quality studies were synthesized descriptively. Currencies were reported in 2019 Canadian dollars. Quality was assessed with the Pediatric Quality Appraisal Questionnaire (PQAQ).
Results
Vision screening services were conducted by paid staff, volunteers, or health care professionals in schools or clinics. Thirteen studies were published from five countries: China (n = 1), United States (n = 4), United Kingdom (n = 1), Canada (n = 1), and Germany (n = 6). Analytical techniques included cost-utility/cost-effectiveness combination (n = 2), cost-effectiveness analysis (n = 7), cost-utility analysis (n = 1), cost-benefit analysis (n = 1), cost-consequence analysis (n = 1), and cost analysis (n = 1). Incremental cost-effectiveness ratios ranged from C$1,056 to C$151,274 per additional case detected/prevented and from C$9,429 to C$30,254,703 per additional QALY gained, depending on the type of screening service and comparator. Six studies were determined to be of high quality.
Conclusion
Vision screening to detect amblyopia for young children may be cost-effective compared with no screening if amblyopia reduced quality of life. Studies varied significantly in the type of screening services and comparators used. Methodological limitations were common. Future studies would be aided immensely by prospective studies on the impact of amblyopia on the health-related quality of life of young children and guidelines on the effective conduct of vision screening.
Résumé
Objectif
Synthétiser et évaluer des évaluations économiques de dépistages visuels visant à détecter la déficience visuelle chez les enfants.
Méthode
Nous avons interrogé sept bases de données électroniques, la littérature grise et les sites Web d’organismes effectuant des évaluations des technologies de la santé. Nous avons inclus les études correspondant aux critères suivants : (1) évaluations économiques comparatives exhaustives utilisant l’analyse coûts-utilité, coûts-bénéfices, coûts-efficacité ou coûts-conséquences ou l’analyse des coûts; (2) décrivant des services de dépistage visant à détecter l’amblyopie, le strabisme ou les anomalies de la réfraction non corrigées chez les enfants de moins de six ans; et (3) publiées après 1994. Nous avons fait la synthèse descriptive des études de haute qualité. Les devises ont été converties en dollars canadiens de 2019. Nous avons évalué la qualité des études à l’aide de l’outil PQAQ (Pediatric Quality Appraisal Questionnaire).
Résultats
Les services de dépistage visuel étaient offerts par du personnel rémunéré, des bénévoles ou des professionnels de santé dans des écoles ou des cliniques. Treize études ont été publiées dans cinq pays : Chine (n = 1), États-Unis (n = 4), Royaume-Uni (n = 1), Canada (n = 1) et Allemagne (n = 6). Les techniques d’analyse employées étaient la combinaison analyse coûts-utilité/analyse coûts-efficacité (n = 2), l’analyse coûts-efficacité (n = 7), l’analyse coûts-utilité (n = 1), l’analyse coûts-avantages (n = 1), l’analyse coûts-conséquences (n = 1) et l’analyse des coûts (n = 1). Les rapports coût-efficacité différentiels s’échelonnaient entre 1 056 $ CA et 151 274 $ CA par cas supplémentaire détecté/prévenu et entre 9 429 $ CA et 30 254 703 $ CA par année de vie pondérée par la qualité (AVPQ) supplémentaire gagnée, selon le type de service de dépistage et le comparateur. Six études ont été jugées être de haute qualité.
Conclusion
Comparativement à l’absence de dépistage, les dépistages visuels pour détecter l’amblyopie chez les jeunes enfants peuvent être efficaces par rapport à leur coût lorsque l’amblyopie réduit la qualité de vie. Le type de services de dépistage et les comparateurs utilisés variaient considérablement d’une étude à l’autre. Les contraintes méthodologiques étaient courantes. Les études futures seraient grandement favorisées par des études prospectives des incidences de l’amblyopie sur la qualité de vie liée à la santé chez les jeunes enfants et par des lignes directrices sur l’exécution efficace des dépistages visuels.
Similar content being viewed by others

Introduction
Amblyopia and refractive errors are the most common vision impairments affecting children worldwide, with a prevalence of 3–5% for amblyopia and 10% for refractive errors (Drover et al., 2008; Pai et al., 2012; Pascolini & Mariotti, 2012). These conditions may affect quality of life and add financial burden (Kandel et al., 2017; Langelaan et al., 2007; Resnikoff et al., 2008; Saw et al., 2007).
To enable the early detection of vision impairment from amblyopia and refractive errors, recommendations for routine vision screening and comprehensive eye exams (CEEs) are common across industrialized nations. In Canada and the United States, routine CEEs and vision screening are recommended by professional pediatric and optometry associations at similar regular intervals throughout childhood (American Optometric Association, 2021; Amit, 2009; Canadian Paediatric Society, 2018; Committee on Practice & Ambulatory Medicine Section on Ophthalmology, 2003). In Australia, health departments in each state and territory have their guidelines regarding vision screening for children (Murdoch Childrens Research Institute, 2009). Vision screening may be required for children turning 4 years of age as part of a health check (Services Australia, n.d). In the United Kingdom, vision screening is recommended by the United Kingdom National Screening Committee in schools for children aged 4 to 5 years (Public Health England, 2017).
In Ontario, Canada, annual CEEs are performed primarily by optometrists and ophthalmologists, and are paid for through the Ontario Health Insurance Program (OHIP), for children and seniors who are legal residents of the province. The Eye See… Eye Learn program, funded by the Ontario Association of Optometrists and the Ontario Ministry of Health (MOH), provides free prescription glasses after a CEE by a participating optometrist to 4-year-old children needing them (Ontario Association of Optometrists, 2015, 2017). In the 2016/2017 academic year, the Eye See… Eye Learn program reported only a 20% participation among eligible children in junior kindergarten (~ aged 4 years). Of these, 47% were first-time eye exams (Ontario Association of Optometrists, 2017). These numbers suggest that children with visual problems may not be identified in a timely manner. To improve early detection, the Ontario Ministry of Health introduced a requirement for universal vision screening programs into the Ontario Public Health Standards in 2017. The requirement stipulates the provision of vision screening by public health units in kindergartens of public schools across Ontario (Ministry of Health and Long-Term Care, 2017), but its cost-effectiveness has not been evaluated.
Several health units in Ontario have faced challenges with the rollout of school-based screening because of rising health care costs and provincial budgeting constraints further exacerbated by the COVID-19 pandemic (Personal Communication). Evidence on the cost-effectiveness of vision screening in the local context will enable health units to make informed decisions on delivering effective vision screening programs without sacrificing other important health programs.
In the face of limited resources and the growing demand on health care spending, policy makers have been increasingly drawn to economic evaluations to support decisions about resource allocation (National Institute for Health & Care Excellence, 2014). To inform the structure and model inputs of economic evaluations, systematic reviews are recommended as best practice in guidelines for health technology assessment (Akers et al., 2009). The purpose of this study is to synthesize and appraise economic evaluations of vision screening to detect amblyopia and refractive errors in children under 6 years of age. This review will inform the design and conduct of a future economic evaluation of vision screening programs in Ontario, Canada.
Methods
Data sources and search strategy
A literature search was carried out using seven electronic databases: MEDLINE (Ovid, PubMed, and Medline in Process), EMBASE (Ovid), The Cochrane Library, the Cost-effectiveness analysis Registry (CEA), Global Health CEA Registry (GHCEA), Paediatric Economic Database Evaluation (PEDE), and EconLit (EBSCO). The following grey literature sources were also searched: Programs for Assessment of Technology in Health (PATH), International Network of Agencies for Health Technology Assessment (INAHTA), Ontario Health Technology Advisory Committee (OHTAC), Health Economics Research Centre (HERC), and ProQuest Dissertations and Theses Global. The websites of agencies that routinely conduct health technology assessments included in the search were as follows: Canadian Agency of Drugs and Technologies in Health (CADTH), National Institute for Health and Care Excellence (NICE) Evidence search and Guidelines, and the European Network for Health Technology Assessment (EUnetHTA). Reference lists of key articles were searched. Citation tracking using the Web of Science database and personal knowledge skills were also employed.
Appropriate search strategies were developed for each database using text words and subject headings for the target disorders (amblyopia, strabismus, and refractive error), service (vision screening), and study type (cost-utility analysis, cost-effectiveness analysis, cost-consequence analysis, cost analysis, cost minimization, and cost-benefit analysis methods). The search strategy was supplemented with validated search filters from the InterTASC Information Specialists’ Sub-Group for economic evaluations and validated using The Peer Review of Electronic Search Strategy (PRESS) checklist (ISSG Search Filter Resource n.d.; McGowan et al., 2016).
Study selection
A study was included if it: (1) was a full, comparative economic evaluation; (2) used any one of the analytic methods (cost-utility analysis, cost-benefit analysis, cost-effectiveness analysis, cost-minimization analysis, cost-consequence analysis, and cost-analysis); and (3) evaluated screening services for children under the age of 6 years to detect amblyopia, strabismus (as a risk factor for amblyopia), and/or uncorrected refractive errors. A study was excluded if: (1) the full text was unavailable; (2) it was a review, commentary, case series, case report, editorial, letter, or conference abstract; or (3) it was published before 1995. Studies before 1995 were excluded because in that year, the first instrument-based screening tools—the Medical Technology and Innovations (MTI) Photoscreener and Nikon Retinomax K-Plus Autorefractor (Nikon Corp, Melville, New York, USA)—became commercially available (Ottar et al., 1995; Silverstein & Donahue, 2018), which revolutionized paediatric vision screening. It was anticipated that studies published after that year would include the newer screening technology to facilitate comparisons. Studies using traditional screening tools were included as they may still be relevant in some jurisdictions. No country or language restrictions were applied. Two reviewers (AA and YK) assessed the identified studies independently. Disagreements were discussed to achieve consensus. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart was developed (Moher et al., 2009).
Data extraction and synthesis
Key aspects of studies were extracted, and results presented in summary tables and text. Currencies reported were converted into Canadian dollars for the year of pricing (or year of study conduct or publication if year of pricing was not reported). Bank of Canada annual average exchange rates were used (Bank of Canada, 2017; Cochrane Handbook for Systematic Reviews of Interventions, 2011; Statistics Canada, 2018, 2020). Prices were then inflated to 2019 Canadian dollars using consumer price indices (CPI) for eye care services from Statistics Canada (Statistics Canada, 2018, 2020). For studies before 2008, health care services CPI were applied because CPI were not reported for eye care services until 2008.
Quality assessment and risk of bias
The quality of the included studies was assessed with the Pediatric Quality Appraisal Questionnaire (PQAQ), a comprehensive instrument demonstrating face and content validity, and strong interrater and test–retest reliability in the appraisal of pediatric economic evaluations (Ungar & Santos, 2003). It is made up of 57 items in 14 domains: (1) Economic evaluation, (2) Comparators, (3) Target population, (4) Time horizon, (5) Perspective, (6) Costs and resource use, (7) Outcomes, (8) Quality of life, (9) Analysis, (10) Discounting, (11) Incremental analysis, (12) Sensitivity analysis, (13) Conflict of interest, and (14) Conclusions. Forty-six of the 57 items can be scored to rate the quality of studies. Items were scored independently between 0 and 1. An unweighted mean was calculated for each domain using all scorable items within the domain. The domain scores ranged between 0 and 1, with higher scores indicating better quality. Two reviewers (AA and YK) conducted quality assessments independently, and discrepancies were resolved through discussion.
Results
Literature sample
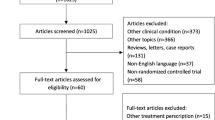
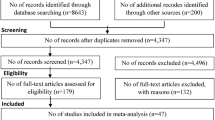
The initial search was conducted on July 13, 2018. A total of 671 publications were identified, of which 13 met the inclusion criteria (Arnold et al., 2005; Carlton et al., 2008; Drover, 2006; Gandjour et al., 2003; Joish et al., 2003; Konig & Barry, 2004; König & Barry, 2002; Konig et al., 2000, 2002; Miller et al., 2003; Rein et al., 2012; Schlichtherle et al., 2000; Wang et al., 2019). None of the studies published before 1995 met the study inclusion criteria. Figure 1 is a PRISMA flowchart describing the process for selecting studies and the reasons for exclusion (Moher et al., 2009). The search strategy developed for Medline is provided in Appendix 1.

PRISMA flow diagram
Quality appraisal
The mean domain quality scores for each included study are summarized in Table 1, with details in Appendices 2 and 3. Key characteristics of all 13 studies are summarized in Table 2. Tables 3 and 4 provide characteristics and outcomes of high-quality studies. Appendices 4 and 5 provide similar details of studies determined to be low quality per the PQAQ. With one exception, studies had an average domain score in the intermediate (0.34 to 0.66; n = 6) or highest quality (0.67 to 1.00; n = 6) range. Some items within a domain were not scored because they were not applicable to the study in question. The three highest scoring domains were Target population (subscore mean 0.92, SD 0.16), Discounting (subscore mean 0.75, SD 0.52), and Outcomes (subscore mean 0.73, SD 0.30). The lowest scoring domains were Analysis (subscore mean 0.54, SD 0.23), Incremental analysis (subscore mean 0.53, SD 0.44), and Costs and resource use (subscore mean 0.36, SD 0.31). Studies using cost-utility and cost-effectiveness techniques generally scored higher because of their inclusion of both costs and consequences/effects (e.g., QALYs). Also, cost-utility and cost-effectiveness analyses lend themselves better to formal modeling techniques, specifically decision analysis and Markov modeling.
Low scores were received for the Analysis, Incremental analysis, and Costs and resource use domains for several reasons. Low Analysis scores were because of the lack of an explicit description of the valuation of costs (n = 2), the omission of a health outcome (n = 1), or assumptions instead of measurements of utility scores (n = 3). Analysis was low because studies did not include appropriate units for the indicated analytic technique, the valuation and aggregation of costs and outcomes were not described, and the sources and quantities of resources and their unit costs were not reported with details of statistical tests and confidence intervals where relevant. Incremental analysis scores were low because of missing incremental estimates (costs and consequences) or ratios with confidence intervals or limits (n = 5). Last, the Costs and resource use score was low because the studies lacked transparency which could be achieved by describing the identification, measurement, and valuation of all costs (Canadian Agency for Drugs & Technologies in Health, 2017). Also, included studies had missing costs such as future salary and productivity losses of the child (n = 13) or the parents (n = 2) and missing sources for either volume or unit costs (n = 3).
Sample characteristics
The 13 included studies were published from 2000 to 2019 from five countries: China (n = 1), USA (n = 4), UK (n = 1), Canada (n = 1), and Germany (n = 6). Seven studies used automated or instrument-based screening tools, i.e., autorefractors and photoscreeners such as the Nikon Retinomax. Appendix 6 provides a list of screening instruments used in the included studies. Although cost-utility analysis is considered the gold standard because of its use of a universal generic measure of effectiveness (QALY) (Canadian Agency for Drugs & Technologies in Health, 2017), only three included studies employed this technique. Cost-effectiveness analysis was used more frequently (n = 7). Cost benefit, cost consequence, and cost analysis were used in three studies. In the three studies using cost-utility analyses, assumptions had to be made about health utilities and QALYs based on expert opinion and/or reported correlations between health utility and visual acuity (Konig & Barry, 2004) because the literature is missing values for child populations. Most studies (n = 7) used a third-party payer perspective instead of the broader societal perspective that incorporates all costs and health benefits regardless of the payer. Two studies did not specify a perspective. Seven studies used modeling techniques—a decision tree (n = 4) or Markov model (n = 2), or both (n = 1). Where discounting was applied (n = 5), it ranged from 3% to 5% and was applied to either costs (n = 1) or effects (n = 1), or both (n = 3). The original currency, costs, and incremental cost-effectiveness ratios (ICERs) of included studies are reported in Appendix 7. The ICER is the incremental cost associated with one additional unit of effect (e.g., additional QALY gained, case detected or prevented) and calculated as follows: ICER = (difference in average costs in an alternative strategy relative to another strategy)/ (difference in average effects in an alternative strategy relative to another strategy).
Descriptive synthesis of high-quality studies
Six studies published in the USA (n = 1), the UK (n = 1), and Germany (n = 4) were determined to be high quality with an average PQAQ domain score between 0.67 and 1.00 inclusive (Carlton et al., 2008; Gandjour et al., 2003; Konig & Barry, 2004; König & Barry, 2002; Konig et al., 2002; Rein et al., 2012). These studies described different vision testing services conducted by paid staff (Rein et al., 2012), volunteers (Rein et al., 2012), teacher’s assistants (Rein et al., 2012) and/or health care professionals (Carlton et al., 2008; Gandjour et al., 2003; Konig & Barry, 2004; König & Barry, 2002; Konig et al., 2002; Rein et al., 2012) including general practitioners, pediatricians (Gandjour et al., 2003; Konig et al., 2002), orthoptists (Carlton et al., 2008; Gandjour et al., 2003; Konig & Barry, 2004; König & Barry, 2002; Konig et al., 2002), and ophthalmologists (Gandjour et al., 2003). Screening was conducted in kindergartens, preschool, or clinics (Carlton et al., 2008; Gandjour et al., 2003; Konig & Barry, 2004; König & Barry, 2002; Konig et al., 2002; Rein et al., 2012). Children who failed screening were referred to ophthalmologists (Gandjour et al., 2003; Konig & Barry, 2004; König & Barry, 2002; Konig et al., 2002; Rein et al., 2012) or optometrists (Carlton et al., 2008). One study included services targeting high-risk children separately from services targeting all children regardless of risk (Gandjour et al., 2003). Another study included services with different combinations of tools and visual acuity thresholds that informed the decision to refer (König & Barry, 2002).
In terms of outcomes, three studies reported effectiveness as “case detected” (Gandjour et al., 2003; König & Barry, 2002; Konig et al., 2002), and one as QALYs (Konig & Barry, 2004). Two studies reported effects as both amblyopia cases prevented and QALYs (Carlton et al., 2008; Rein et al., 2012). One study considered costs from a societal payer perspective (Rein et al., 2012), four from a third-party payer perspective (Carlton et al., 2008; Konig & Barry, 2004; König & Barry, 2002; Konig et al., 2002), and one from both societal and third-party payer perspectives (Gandjour et al., 2003).
Cost-effectiveness in studies considering a societal payer perspective
Cost-effectiveness reported in incremental cost per additional case detected
Gandjour et al. (2003), compared three alternative strategies for children up to 4 years of age to the screening of only high-risk children under the age of 1 year by an ophthalmologist in Germany (HOPH). The three alternative strategies included (1) universal screening by an ophthalmologist (OPH) which yielded an incremental cost of DM2,571 (C$4,502) per additional case detected; (2) screening all children aged 3 to 4 years by a general practitioner or paediatrician (PGP) which yielded an incremental cost of DM6,445 (C$9,774) per additional case detected; and (3) screening all children aged 3 to 4 years by an orthoptist (ORT). In this comparison of ORT vs. HOPH, ORT was dominated by HOPH, meaning that it was more costly and less effective compared to HOPH. While the ORT program screened all children, the HOPH program screened only high-risk children, which explains the significantly higher costs in the ORT program. In these cases, ICERs are not calculated as per health technology assessment reporting guidelines (Canadian Agency for Drugs & Technologies in Health, 2017). A willingness-to-pay (WTP) threshold, which represents the maximum amount for which society would be willing to pay for particular health outcomes (i.e. cost per additional case of amblyopia detected in this study), was not defined in this study.
Cost-effectiveness reported in incremental cost per additional QALY gained
Rein et al. (2012) compared three strategies to no screening (NS) in a US population using trained staff, volunteers, and teacher’s assistants at a WTP of US$25,000 per additional QALY gained and reported the incremental cost per additional QALY gained as follows: (1) acuity/stereopsis screening in kindergarten (KA/S)— US$15,385 (C$28,322); (2) acuity/stereopsis screening in kindergarten and preschool (PKA/S)—US$17,727 (C$32,635); and (3) preschool photoscreening followed by kindergarten acuity/stereopsis screening (PPKA/S)—US$22,083 (C$40,654). All three strategies were cost-effective, with the first—acuity/stereopsis screening in kindergarten (KA/S)—being most cost-effective. Comparing each strategy to the next most costly, acuity/stereopsis screening in kindergarten and preschool (PKA/S) was cost-effective at an incremental cost of US$21,111 (C$38,864) per additional QALY gained compared to acuity/stereopsis screening in kindergarten (KA/S). Preschool photoscreening followed by kindergarten acuity/stereopsis screening (strategy 3) was not cost-effective compared to acuity/stereopsis in kindergarten and preschool (strategy 2) at an incremental cost of US$70,000 (C$128,865) per additional QALY gained.
Cost-effectiveness in studies considering third-party payer perspectives
Cost-effectiveness reported in costs per additional case prevented
Carlton et al. evaluated seven strategies (no screening, and screening at 3, 4, and 5 years with and without autorefraction) and compared each with the next most costly strategy based on a UK population with costs incurred by the National Health Service (Carlton et al., 2008). Screening at 3 years without autorefraction (3WOA) yielded an incremental cost of £3368 (C$10,392) per additional case prevented compared with no screening. Screening at 4 years (4WOA) compared with screening at 3 years yielded an incremental cost of £6,295 (C$18,932) per additional case prevented, while screening with autorefraction at age 4 years (4WA) compared with no autorefraction (4WOA) yielded an incremental cost of £6,348 (C$19,315) per additional case prevented. Screening at age 5 years with autorefraction (5WA) compared with screening at age 4 years (4WA) yielded an incremental cost of £57,673 (C$151,274) per additional case prevented. Screening at age 5 years without autorefraction (5WOA) and at age 3 years with autorefraction (3WA) was more costly and less effective than the next most costly strategy. A WTP threshold was not defined.
In the study by Rein et al., amblyopia cases prevented were not expressed as an ICER. However, 49% of amblyopia cases were prevented in the KA/S strategy, 76% in PKA/S, and 82% in PPKA/S.
Cost-effectiveness reported in costs per additional case detected
Konig et al. published two studies in 2002 for the German context from the perspective of the German Social Health Insurance (König & Barry, 2002; Konig et al., 2002). In the first study (Konig et al., 2002), three strategies—no screening (UC), screening of all children aged 3 years in kindergarten by orthoptists (ORTH), and screening of children aged 3 years in kindergarten not under treatment by an orthoptist (ORTH +)—were compared with the next most costly strategy. Screening of all children aged 3 years (ORTH) compared with no screening (UC) yielded an incremental cost of DM924 (C$1,178) per additional case detected. Screening of children not under treatment (ORTH +) compared with all children by orthoptists (ORTH) yielded an incremental cost of DM829 (C$1,056) per additional case detected. In the second study (König & Barry, 2002), 10 alternative screening options were modelled comprising screening with different visual acuity thresholds for referrals, and alternative sets of screening tests and tools. For each screening option, uncooperative children were modelled in two ways: (1) with immediate referral to an ophthalmologist; and (2) re-screening after a year. Visual acuity testing with a pass threshold of at least 0.6 (20/32) visual acuity in both eyes (MVA2-2), compared with decreasing the pass threshold to a visual acuity of at least 0.5 (20/40) in both eyes and re-screening a year later (MVA1-2), produced an incremental cost of DM1,058 (C$1,348) per additional case detected. Compared with MVA2-2, including more tests in addition to visual acuity tests (MVA4-2) produced an incremental cost of DM1,359 (C$1,732) per additional case detected. Finally, compared with MVA4-2, immediate referrals to an ophthalmologist instead of rescreening a year later produced an incremental cost of DM13,448 (C$17,138) per additional case detected. A WTP threshold was not defined in both studies.
Cost-effectiveness reported in cost per additional QALY gained
Carlton et al. (2008) examined seven strategies (no screening, screening at 3, 4, and 5 years old using cover tests with and without autorefraction). Comparing each strategy with the next most costly, screening at 3 years without autorefraction (3WOA) compared with no screening yielded an incremental cost of £503,842 (C$1,532,380) per additional QALY gained. Screening at 4 years without autorefraction (4WOA) compared with screening at 3 years without autorefraction (3WOA) yielded an incremental cost of £941,872 (C$3,245,549) per additional QALY gained, while screening with autorefraction at age 4 years (4WA) compared with without autorefraction (4WOA) yielded an incremental cost of £949,750 (C$2,846,443) per additional QALY gained. Screening at age 5 years with autorefraction (5WA) compared with screening at 4 years (4WA) yielded an incremental cost of £8,628,530 (C$30,254,703) per additional QALY gained. Screening at age 5 years without autorefraction (5WOA) and age 3 years with autorefraction (3WA) were dominated, indicating that these two strategies were not cost-effective relative to the next most costly strategy, 4WOA. A WTP threshold was not defined. In Canada, the WTP is typically reported as a range between C$20,000 and C$100,000 per QALY gained (Laupacis et al., 1992). With a WTP between C$20,000 and C$100,000 per QALY gained, none of the strategies was considered cost-effective compared with its comparator.
Last, Konig and Barry (2004) in 2004 compared the costs incurred by the German Social Health Insurance Funds and benefits of screening the vision of all children aged 3 years by orthoptists in German kindergartens (OS) to usual care screening (in which amblyopia could be detected by an ophthalmologist in the absence of orthoptic screening) to detect amblyopia. The incremental cost was determined to be DM7,397 (C$9,429) per additional QALY gained.
Discussion
A wide range in ICERs was reported in the included high-quality studies. From a societal perspective, cost-effectiveness was reported as ranging from C$4,502 to C$9,774 per additional case detected (Gandjour et al., 2003) and from C$28,322 to C$40,654 per additional QALY gained (Rein et al., 2012). From a third-party payer perspective, cost-effectiveness ranged from C$10,392 to C$151,274 per additional case prevented (Carlton et al., 2008), C$1,056 to C$17,138 per additional case detected (König & Barry, 2002; Konig et al., 2002), and C$9,429 to C$30,254,703 per additional QALY gained (Carlton et al., 2008; Konig & Barry, 2004). From both perspectives compared with no screening, screening programs were found to be cost-effective at a WTP threshold greater than C$10,392 per additional case prevented (Carlton et al., 2008), or greater than C$1,178 per additional case detected (Carlton et al., 2008; König & Barry, 2002; Konig et al., 2002). Considering cost per additional QALY gained, screening programs compared with no screening were less likely to be cost-effective with incremental costs ranging from C$28,322 to C$1,532,380 per additional QALY gained (Carlton et al., 2008; Rein et al., 2012). Despite the high quality of included studies, this wide range in ICERs is an indication that uncertainty persisted due to the vastly different ways vision screening services were organized within similar target age groups, differences in the study designs (e.g. the choice of comparator and the diverse outcomes considered), and the various country contexts (e.g. variation in prevalence and in how health care is organized, delivered, and subsidized). The variation in the organization of screening stems partly from the lack of guidelines on best practices for conducting vision screening programs in most jurisdictions. The variation in ICERs may also be caused by the lack of evidence on the impact of amblyopia on quality of life, resulting in a wide range of utility estimates used by different studies. While it is difficult to take a definitive stance on cost-effectiveness overall, the literature suggests that vision screening to detect amblyopia for children under 6 years may be a cost-effective approach compared with no screening if amblyopia reduces quality of life.
The results of the included studies may not be generalizable to populations at high-risk of developing vision disorders because of differences in the prevalence of target conditions, availability, and costs of follow-up care in high-risk vs general populations. The included studies suggest that if amblyopia reduces quality of life, vision screening interventions in large populations using tools with high accuracy may be cost-effective. Therefore, investing in interventions that are affordable and accessible such as those offered in kindergartens and preschools in communities of low socioeconomic status by trained lay-persons (e.g. volunteers and teacher’s assistants) using screening tools with high accuracy may be cost-effective relative to no screening. Autorefractors and photoscreeners are expensive tools compared with traditional tools (e.g. visual acuity charts and stereopsis tests). However, these tools can screen large numbers of children in the shortest possible time with high accuracy, a system that reduces the costs per child. Underserved communities may benefit from optometry exams in schools or supported referrals to eye care professionals by primary care physicians. To prevent children falling between the gaps, greater subsidies for prescription glasses and surveillance systems that allow primary and eye care professionals to identify children that miss follow-up appointments may be beneficial. Additionally, educational campaigns on key vision health topics in native languages may be effective in underserved communities. Indigenous and immigrant communities may especially benefit from the provision of culturally sensitive services which could be achieved by employing local community members as screeners, local champions to support awareness campaigns, and translators. Future economic evaluations should be designed to address the needs of underserved communities by considering relevant variables that account for the higher prevalence, and limited access to and costs of follow-up care and treatment.
One methodological limitation with the included cost-utility analyses was the lack of accurate health state utilities for amblyopia and refractive errors measured in children because of the absence of an appropriate, validated tool. Therefore, studies resorted to the use of proxies (Carlton et al., 2008; Griebsch et al., 2005; Konig & Barry, 2004; Rein et al., 2012), assumptions of no impact of the conditions on health utilities (Carlton et al., 2008), or the same health utilities in children as adults with other types of vision impairment besides amblyopia and refractive errors (Konig & Barry, 2004). These different assumptions on the impact of amblyopia and refractive errors on quality of life in children have led to significant variability in the results of cost-utility analyses. Assuming no impact on health utility is unsubstantiated because it implies an indifference to vision impairment caused by amblyopia and refractive errors despite indications in the literature of the adverse psychosocial impact of amblyopia and refractive errors on individuals (Horwood et al., 2005; Sabri et al., 2006; Senra et al., 2015). One study has reported no association between amblyopia and educational, social activities, employment, health outcomes, and psychosocial domains (Rahi et al., 2006). Only four published studies have attempted to derive health utility weights in children for vision impairment (Boulton et al., 2006; Carroll & Downs, 2009; Petrou & Kupek, 2009; Saw et al., 2003). No studies have been conducted to derive health utility weights in children with vision impairment caused by amblyopia and refractive errors. Another methodological limitation was the lack of reporting or justification of a time horizon. This raises concerns whether all relevant costs and outcomes were captured. Adopting lifetime horizons for economic evaluations in pediatric populations may require several assumptions because of the uncertainty regarding costs and effects in the future.
To the best of our knowledge, no other review of the literature has been published on the cost-effectiveness of vision screening to detect amblyopia or refractive errors in young children. Yet, several reviews on the efficacy and/or effectiveness of vision screening in preschools have noted methodological limitations precluding definitive conclusions on the effectiveness of vision screening programs (Chou et al., 2011; Evans et al., 2018; Jonas et al., 2017; Lagrèze, 2010; Mathers et al., n.d.).
A few limitations in the conduct of this review are worthy of note. Some relevant studies may not have been identified by the search strategy because of poor or no indexing, or because they were included in electronic databases not covered in our search strategy. This is unlikely, however, because our search strategy included a comprehensive number of electronic databases with limited geographical bias. We also validated the search strategy against an initial test set of key articles. To move toward a more definitive conclusion regarding the cost-effectiveness of vision screening programs to detect amblyopia and refractive errors in this population, a meta-analysis would be helpful. A meta-analysis was not conducted because of the heterogeneity in the included studies and disagreement regarding methods for pooling incremental cost-effectiveness (including utility estimates) or cost benefit ratios extracted from multiple economic evaluations (Cochrane Handbook for Systematic Reviews of Interventions, 2011; van Mastrigt et al., 2016).
Conclusion
This systematic review and quality appraisal of the literature on economic evaluations of vision screening strategies in children demonstrated significant variability in types of screening services and the type and quality of methods used, yielding highly variable results. Strategies for enhancing the quality of economic evaluations of vision screening strategies and guidelines on conducting effective vision screening programs are required. Most importantly, prospective studies on the impact of amblyopia and/or refractive errors on the health-related quality of life of young children to generate reliable utilities for use in cost-utility analysis are needed.
Availability of data and material
Not applicable.
Code availability
Not applicable.
References
Akers, J., Aguiar-Ibáñez, R., & Baba-Akbari Sari, A. (2009). Centre for Reviews and Dissemination (CRD)'s guidance for undertaking reviews in health care. Retrieved from York (UK): https://www.york.ac.uk/media/crd/Systematic_Reviews.pdf.
American Optometric Association. (2021). Recommended eye examination frequency for pediatric patients and adults. Retrieved from https://www.aoa.org/healthy-eyes/caring-for-your-eyes/eye-exams?sso=y.
Amit, M. C. P. S. (2009). Vision screening in infants, children and youth. Paediatr Child Health, 14(4), 246–251. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/20357924.
Arnold, R. W., Armitage, M. D., Gionet, E. G., Balinger, A., Kovtoun, T. A., Machida, C., & Coon, L. J. (2005). The cost and yield of photoscreening: Impact of photoscreening on overall pediatric ophthalmic costs. Journal of Pediatric Ophthalmology and Strabismus, 42(2), 103–111.
Bank of Canada. (2017). Historical noon and closing rates: Annual average rates. Retrieved from https://www.bankofcanada.ca/rates/exchange/legacy-noon-and-closing-rates/.
Boulton, M., Haines, L., Smyth, D., & Fielder, A. (2006). Health-related quality of life of children with vision impairment or blindness. Developmental Medicine & Child Neurology, 48(8), 656–661. https://doi.org/10.1017/S0012162206001381
Canadian Agency for Drugs and Technologies in Health. (2017). Guidelines for the economic evaluation of health technologies: Canada. Retrieved from Ottawa: https://www.cadth.ca/about-cadth/how-we-do-it/methods-and-guidelines/guidelines-for-the-economic-evaluation-of-health-technologies-canada.
Canadian Paediatric Society. (2018). Caring for Kids. Information for parents from Canada's Paediatricians. Schedule of well-child visits. Retrieved from https://www.caringforkids.cps.ca/handouts/schedule_of_well_child_visits.
Carlton, J., Karnon, J., Czoski-Murray, C., Smith, K. J., & Marr, J. (2008). The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4–5 years: A systematic review and economic evaluation. Health Technology Assessment, 12(25), iii-xi–194.
Carroll, A. E., & Downs, S. M. (2009). Improving decision analyses: Parent preferences (utility values) for pediatric health outcomes. Journal of Pediatrics, 155(1), 21-25.e21-25. https://doi.org/10.1016/j.jpeds.2009.01.040
Chou, R., Dana, T., & Bougatsos, C. (2011). Screening for visual impairment in children ages 1–5 years: Update for the USPSTF. Pediatrics, 127(2), e442–e479. https://doi.org/10.1542/peds.2010-0462
Cochrane handbook for systematic reviews of interventions. (2011). [5.1.0]. In J. P. T. Higgins & S. Green (Eds.). Retrieved from www.handbook.cochrane.org.
Committee on Practice and Ambulatory Medicine Section on Ophthalmology . (2003). Eye examination in infants, children, and young adults by pediatricians. Ophthalmology, 110(4), 860–865. https://doi.org/10.1016/S0161-6420(03)00414-7
Drover, J. R. (2006). A new screening program for the detection of amblyopia and other early visual disorders in toddlers and preschool children. (PhD). Memorial University of Newfoundland, St John's, Newfoundland. Retrieved from https://research.library.mun.ca/view/theses_dept/Psychology.date.html#group_2006 (ISBN: 978–0–494–30430–3).
Drover, J. R., Kean, P. G., Courage, M. L., & Adams, R. J. (2008). Prevalence of amblyopia and other vision disorders in young Newfoundland and Labrador children. Canadian Journal of Ophthalmology, 43(1), 89–94. https://doi.org/10.3129/i07-187
Evans, J. R., Morjaria, P., & Powell, C. (2018). Vision screening for correctable visual acuity deficits in school-age children and adolescents. Cochrane database of Systematic Reviews (Online), 2(2), Cd005023. https://doi.org/10.1002/14651858.CD005023.pub3
Gandjour, A., Schlichtherle, S., Neugebauer, A., Russmann, W., & Lauterbach, K. W. (2003). A cost-effectiveness model of screening strategies for amblyopia and risk factors and its application in a German setting. Optometry & Vision Science, 80(3), 259–269.
Griebsch, I., Coast, J., & Brown, J. (2005). Quality-Adjusted life-years lack quality in pediatric care: A critical review of published cost-utility studies in child health. Pediatrics, 115(5), e600–e614. https://doi.org/10.1542/peds.2004-2127
Horwood, J., Waylen, A., Herrick, D., Williams, C., & Wolke, D. (2005). Common visual defects and peer victimization in children. Investigative Ophthalmology & Visual Science, 46(4), 1177–1181. https://doi.org/10.1167/iovs.04-0597
ISSG Search Filter Resource [Internet]. Glanville J, Lefebvre C, Manson P, Robinson S and Shaw N, editors. York (UK): The InterTASC Information Specialists' Sub-Group; 2006 [updated 7 Sept 2021; cited 7 Sept 2021]. Available from https://sites.google.com/a/york.ac.uk/issg-search-filters-resource/home
Joish, V. N., Malone, D. C., & Miller, J. M. (2003). A cost-benefit analysis of vision screening methods for preschoolers and school-age children. Journal of AAPOS, 7(4), 283–290. https://doi.org/10.1016/mpa.2003.S1091853103001162
Jonas, D. E., Amick, H. R., Wallace, I. F., Feltner, C., Vander Schaaf, E. B., Brown, C. L., & Baker, C. (2017). Vision Screening in children aged 6 months to 5 years: Evidence report and systematic review for the US Preventive Services Task Force. JAMA, 318(9), 845–858. https://doi.org/10.1001/jama.2017.9900
Kandel, H., Khadka, J., Goggin, M., & Pesudovs, K. (2017). Impact of refractive error on quality of life: A qualitative study. Clinical and Experimental Ophthalmology, 45(7), 677–688. https://doi.org/10.1111/ceo.12954
König, H. H., & Barry, J. C. (2002). Economic evaluation of different methods of screening for amblyopia in kindergarten. Pediatrics, 109(4). Retrieved from https://www.scopus.com/inward/record.uri?eid=2-s2.0-0036551017&partnerID=40&md5=4aac7a65259645c8a64387c21afd3a42.
Konig, H. H., & Barry, J. C. (2004). Cost-utility analysis of orthoptic screening in kindergarten: A Markov model based on data from Germany. Pediatrics, 113(2), e95–108. Retrieved from http://pediatrics.aappublications.org/content/pediatrics/113/2/e95.full.pdf.
Konig, H. H., Barry, J. C., Leidl, R., & Zrenner, E. (2000). Cost-effectiveness of orthoptic screening in kindergarten: A decision-analytic model. Strabismus, 8(2), 79–90.
Konig, H. H., Barry, J. C., Leidl, R., & Zrenner, E. (2002). Economic evaluation of orthoptic screening: Results of a field study in 121 German kindergartens. Investigative Ophthalmology & Visual Science, 43(10), 3209–3215.
Lagrèze, W. A. (2010). Vision screening in preschool children: Do the data support universal screening? Deutsches Ärzteblatt International, 107(28–29), 495–499. https://doi.org/10.3238/arztebl.2010.0495
Langelaan, M., de Boer, M. R., van Nispen, R. M., Wouters, B., Moll, A. C., & van Rens, G. H. (2007). Impact of visual impairment on quality of life: A comparison with quality of life in the general population and with other chronic conditions. Ophthalmic Epidemiology, 14(3), 119–126. https://doi.org/10.1080/09286580601139212
Laupacis, A., Feeny, D., Detsky, A. S., & Tugwell, P. X. (1992). How attractive does a new technology have to be to warrant adoption and utilization? Tentative guidelines for using clinical and economic evaluations. Cmaj, 146(4), 473–481. Retrieved from https://pubmed.ncbi.nlm.nih.gov/1306034.
Mathers, M., Keyes M Fau - Wright, M., & Wright, M. A review of the evidence on the effectiveness of children's vision screening. (1365–2214 (Electronic)).
McGowan, J., Sampson, M., Salwedel, D. M., Cogo, E., Foerster, V., & Lefebvre, C. (2016). PRESS - Peer Review of Electronic Search Strategies: 2015 Guidleine Explanation and Elaboration (PRESS E&E). Retrieved from Ottawa:
Miller, J. M., Dobson, V., Harvey, E. M., & Sherrill, D. L. (2003). Cost-efficient vision screening for astigmatism in Native American preschool children. Investigative Ophthalmology and Visual Science, 44(9), 3756–3763. https://doi.org/10.1167/iovs.02-0970
Ministry of Health and Long Term Care. (2017). Standards for public health programs and services. In Consultation document.
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ: British Medical Journal, 339(7716), 332–336. Retrieved from http://www.jstor.org.myaccess.library.utoronto.ca/stable/25672329.
Murdoch Childrens Research Institute. (2009). National Children's Vision Screening Project. Final Report. Retrieved from https://www.iapb.org/wp-content/uploads/Final-Report-Vision-Screening-May-2009.pdf.
National Institute for Health and Care Excellence. (2014). Developing NICE guidelines: The manual. Retrieved from https://www.nice.org.uk/media/default/.../developing-nice-guidelines-the-manual.pdf.
Ontario Association of Optometrists. (2015). Eye See...Eye Learn.
Ontario Association of Optometrists. (2017). Eye See... Eye Learn 2016–17 Fourth Quarter Report. Retrieved from.
Ottar, W. L., Scott, W. E., & Holgado, S. I. (1995). Photoscreening for amblyogenic factors. Journal of Pediatric Ophthalmology and Strabismus, 32(5), 289–295.
Pai, A. S. I., Rose, K. A., Leone, J. F., Sharbini, S., Burlutsky, G., Varma, R., … Mitchell, P. (2012). Amblyopia prevalence and risk factors in Australian preschool children. Ophthalmology, 119(1), 138–144. https://doi.org/10.1016/j.ophtha.2011.06.024
Pascolini, D., & Mariotti, S. P. (2012). Global estimates of visual impairment: 2010. British Journal of Ophthalmology, 96(5), 614–618. https://doi.org/10.1136/bjophthalmol-2011-300539
Petrou, S., & Kupek, E. (2009). Estimating Preference-Based Health Utilities Index Mark 3 utility scores for childhood conditions in England and Scotland. Medical Decision Making, 29(3), 291–303. https://doi.org/10.1177/0272989X08327398
Public Health England. (2017). Vision screening for 4 to 5 year olds. Retrieved from https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/653434/vision_screening_parent_leaflet.pdf.
Rahi, J. S., Cumberland, P. M., & Peckham, C. S. (2006). Does amblyopia affect educational, health, and social outcomes? Findings from 1958 British birth cohort. BMJ, 332(7545), 820–825. https://doi.org/10.1136/bmj.38751.597963.AE
Rein, D. B., Wittenborn, J. S., Zhang, X., Song, M., Saaddine, J. B., & Vision Cost-effectiveness Study, G. (2012). The potential cost-effectiveness of amblyopia screening programs. J Pediatr Ophthalmol Strabismus, 49(3), 146–155; quiz 145, 156. https://doi.org/10.3928/01913913-20110823-02.
Resnikoff, S., Pascolini, D., Mariotti, S. P., & Pokharel, G. P. (2008). Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bulletin of the World Health Organization, 86(1), 63–70. https://doi.org/10.2471/blt.07.041210
Sabri, K., Knapp, C. M., Thompson, J. R., & Gottlob, I. (2006). The VF-14 and psychological impact of amblyopia and strabismus. Investigative Ophthalmology & Visual Science, 47(10), 4386–4392. https://doi.org/10.1167/iovs.05-1365
Saw, S. M., Gazzard, G., Au Eong, K. G., & Koh, D. (2003). Utility values and myopia in teenage school students. British Journal of Ophthalmology, 87(3), 341–345. https://doi.org/10.1136/bjo.87.3.341
Saw, S. M., Cheng, A., Fong, A., Gazzard, G., Tan, D. T., & Morgan, I. (2007). School grades and myopia. Ophthalmic & Physiological Optics, 27(2), 126–129. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=med5&AN=17324201.
Schlichtherle, S., Gandjour, A., Neugebauer, A., Rüssmann, W., & Lauterbach, K. W. (2000). The cost-effectiveness of screening strategies for amblyopia: A preliminary report. Strabismus, 8(4), 291–295. https://doi.org/10.1076/stra.8.4.291.685
Senra, H., Barbosa, F., Ferreira, P., Vieira, C. R., Perrin, P. B., Rogers, H., … Leal, I. (2015). Psychologic adjustment to irreversible vision loss in adults: A systematic review. Ophthalmology, 122(4), 851–861. https://doi.org/10.1016/j.ophtha.2014.10.022
Services Australia. Healthy Start for School. Retrieved from https://www.servicesaustralia.gov.au/individuals/services/centrelink/family-tax-benefit/what-can-affect-your-payment/healthy-start-school#:~:text=A%20health%20check%20is%20an,from%20when%20they%20turn%203.
Silverstein, E., & Donahue, S. P. (2018). Preschool vision screening: Where we have been and where we are going. American Journal of Ophthalmology, 194, xviii-xxiii. https://doi.org/10.1016/j.ajo.2018.07.022.
Statistics Canada. (2018). Consumer Price Index, by province (monthly) CANSIM, table 326–0020 and Catalogue nos. 62–001-X and 62–010-X. Retrieved from http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/cpis01a-eng.htm.
Statistics Canada. (2020). Table 18–10–0005–01 Consumer Price Index, annual average, not seasonally adjusted. Retrieved from https://www150.statcan.gc.ca/t1/tbl1/en/cv.action?pid=1810000501#timeframe.
Ungar, W. J., & Santos, M. T. (2003). The Pediatric Quality Appraisal Questionnaire: An instrument for evaluation of the pediatric health economics literature. Value in Health, 6(5), 584–594. https://doi.org/10.1046/j.1524-4733.2003.65253.x
van Mastrigt, G. A., Hiligsmann, M., Arts, J. J., Broos, P. H., Kleijnen, J., Evers, S. M., & Majoie, M. H. (2016). How to prepare a systematic review of economic evaluations for informing evidence-based healthcare decisions: A five-step approach (part 1/3). Expert Review of Pharmacoeconomics & Outcomes Research, 16(6), 689–704. https://doi.org/10.1080/14737167.2016.1246960
Wang, L., Congdon, N., Hogg, R. E., Zhang, S., Li, M., Shi, Y., … Iyer, M. (2019). The cost-effectiveness of alternative vision screening models among preschool children in rural China. Acta Ophthalmologica, 97(3), e419–e425. https://doi.org/10.1111/aos.13954
Funding
This study was supported by a Collaborative Health Research Project grant from the Canadian Institutes of Health Research and the Natural Sciences and Engineering Research Council of Canada (to Daphne Maurer and Agnes Wong), a research grant from the Physicians’ Services Incorporated Foundation (to Agnes Wong and Daphne Maurer), the Ophthalmology Research Fund from The Hospital for Sick Children (to Agnes Wong), and the Vision Science Research Program University of Toronto (to Afua Asare). Wendy J. Ungar is supported by a tier 1 Canada Research Chair in Economic Evaluation and Technology Assessment in Child Health. Natasha Saunders is supported by a CIHR-SickKids New Investigator Award, Centre for Addiction and Mental Health Discovery Fund, Department of Pediatrics at The Hospital for Sick Children, and an Honorarium from Archives of Diseases in Childhood.
Author information
Authors and Affiliations
Contributions
YK was one of two independent reviewers of abstracts and articles identified in the search. All the other authors provided mentorship and direction in various aspects of the manuscript (study design, inclusion and exclusion criteria, manuscript structure and content, etc.) as part of AOA’s PhD thesis research committee at the Institute of Health Policy, Management and Evaluation, University of Toronto.
Corresponding author
Ethics declarations
Ethics approval
Approved by the University of Toronto and SickKids Research Ethics Board (REB).
Consent to participate
Not applicable.
Consent for publication.
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Asare, A.O., Wong, A.M.F., Maurer, D. et al. Economic evaluations of vision screening to detect amblyopia and refractive errors in children: a systematic review. Can J Public Health 113, 297–311 (2022). https://doi.org/10.17269/s41997-021-00572-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.17269/s41997-021-00572-x
Keywords
- Economic evaluation
- Vision screening
- Amblyopia
- Refractive errors
- Pediatrics
- Systematic review
- Vision impairment
- Eye exams
- School screening
- Preschool
- Kindergarten