
Abstract
Background
Tumors at the hepatocaval confluence can be treated with parenchyma-sparing surgery, also with minimally invasive approach.1,2 The “Liver Tunnel” was described for tumors involving the paracaval portion of Sg1 in contact or infiltrating the middle hepatic vein (MHV).3 A “Liver Tunnel” with laparoscopic approach is proposed.
Methods
A 48-year-old woman was referred for three synchronous colorectal liver metastases in the paracaval portion of Sg1 in contact with the inferior vena cava and the MHV, in Sg8 ventral and in Sg6, after an urgent left laparoscopic hemicolectomy for an obstructing carcinoma. A laparoscopic Sg1 resection extended to Sg8 ventral were planned after neoadjuvant chemotherapy. Estimated future liver remnant (FLR) was 75% (840 ml) of healthy liver (Fig. 1). In case of right hepatectomy extended to Sg1, estimated FLR was 25% (280 ml) of healthy liver.

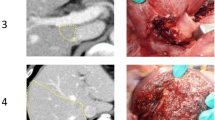
3D reconstruction and intraoperative images of Liver Tunnel (A) and Sg6 resection (B). Total liver volume: 1110 ml. Total resected liver volume 270 ml: Liver Tunnel 93 ml; Sg6 177 ml. Liver volumes were measured with HA3D™ technology with Medics3D software (Medics3D, Turin, Italy)
Results
Pneumoperitoneum is established, and four operative ports are placed. Sg1 is approached from the left, dividing the Glissonean pedicles and short hepatic veins. MHV is approached cranio-caudally from the dorsal side. The resection continues on the ventral side, according to our “Ultrasound Liver Map technique” with a cranio-caudal approach to the MHV.4 Sg8 ventral pedicles are divided and the resection completed with aid of indocyanine green negative staining. A Sg6 resection is then performed. Operative time was 480 min. Blood loss was 100 ml. The postoperative course was uneventful, and the patient was discharged on fourth postoperative day. The two parenchyma-sparing resections saved an estimated volume of 75% (840 ml) of healthy liver (Fig. 1). The estimated remnant liver volume after a right hepatectomy extended to Sg1 would have been only 25%.
Conclusions
Tumors at the hepatocaval confluence involving Sg1 can be removed with the “Liver Tunnel,” which can be performed with minimally invasive approach. The “Laparoscopic Liver Tunnel” pushes further the limit of minimally invasive parenchyma-sparing surgery for ill-located tumors with complex vascular relationship.
Similar content being viewed by others


References
Torzilli G, Garancini M, Donadon M, Cimino M, Procopio F, Montorsi M. Intraoperative ultrasonographic detection of communicating veins between adjacent hepatic veins during hepatectomy for tumours at the hepatocaval confluence. Br J Surg. 2010;97(12):1867–73. https://doi.org/10.1002/bjs.7230.
Lo Tesoriere R, Forchino F, Fracasso M, Russolillo N, Langella S, Ferrero A. Color Doppler intraoperative ultrasonography evaluation of hepatic hemodynamics for laparoscopic parenchyma-sparing liver resections. J Gastrointest Surg. 2022;26(10):2111–8. https://doi.org/10.1007/s11605-022-05430-w.
Torzilli G, Cimino M, Procopio F, et al. Conservative hepatectomy for tumors involving the middle hepatic vein and segment 1: the liver tunnel. Ann Surg Oncol. 2014;21(8):2699. https://doi.org/10.1245/s10434-014-3675-9.
Ferrero A, Lo Tesoriere R, Russolillo N. Ultrasound liver map technique for laparoscopic liver resections. World J Surg. 2019;43(10):2607–11. https://doi.org/10.1007/s00268-019-05046-3.
Acknowledgment
The authors thank the staff at Medics3d (www.medics3d.com) for 3D anatomical modeling and video animation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
Drs. Alessandro Ferrero, Roberto Lo Tesoriere, Rebecca Panconesi, Serena Langella, Andrea Pierluigi Fontana, and Nadia Russolillo have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 340728 kb)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ferrero, A., Lo Tesoriere, R., Panconesi, R. et al. Laparoscopic Liver Tunnel for Tumors at the Hepatocaval Confluence. Ann Surg Oncol 31, 772–773 (2024). https://doi.org/10.1245/s10434-023-14499-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-023-14499-9