
Abstract
Background
The availability of high-quality patient-reported outcome (PRO) data is crucial to guiding shared decision-making in the context of locally recurrent rectal cancer (LRRC), where potential treatment benefits must be balanced against the impact of both the disease and treatment on PROs, such as quality of life. This review aimed to identify the patient-reported outcome measures (PROMs) currently being reported in LRRC and to appraise the methodological quality of studies using these measures.
Methods
PubMed, Embase and CINAHL databases were searched, including studies published up until 14th September 2022. Studies in adults with LRRC reporting PROMS as a primary or secondary outcome measure were included. Data were extracted concerning the methodological quality of the reporting of PROMs using criteria informed by the CONSORT-PRO checklist and the psychometric properties of the PROMs identified using the COSMIN Risk of Bias checklist.
Results
Thirty-five studies including 1914 patients with LRRC were identified. None of the studies included in the review met all eleven criteria for the quality of reporting of PROMs. Seventeen PROMs and two clinician-reported outcome measures were identified, none of which have been validated for use in patients with LRRC.
Conclusions
None of the PROMs which are currently being used to report PROs in LRRC have been validated for use in this cohort of patients. Future studies in this disease area should focus on utilising PROMs that have undergone a robust development process including patients with LRRC, to produce data which is high quality, accurate and relevant.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
The availability of high-quality studies reporting patient-reported outcome (PRO) data utilising robustly developed patient-reported outcome measures (PROMs), offer several advantages to patient care, including their utility within shared decision-making discussions. Baseline PRO data has been shown to act as a prognostic factor for overall survival in cancer patients,1 including those with advanced malignancy.2,3 Integrating PROs into clinical care to monitor adverse effects of cancer treatment can also enhance patient quality of life,4 and has even been reported to improve survival.5,6 The interest in utilising PROMs from both a clinical and academic standpoint continues to grow given the potential utility of these outcome measures, including in patients with locally recurrent rectal cancer (LRRC). The inclusion of patient-reported outcomes (PROs) is particularly important in the context of advanced malignancy such as LRRC. LRRC can lead to debilitating symptoms such as pain, bleeding/discharge from the rectum, pelvic sepsis, urinary symptoms, lower limb symptoms and impaired sexual function. Surgical resection represents the only curative treatment option for patients with LRRC, with 5-year survival rates of 42.4% - 63% reported by specialist tertiary centres.7,8,9,10,11 Exenterative surgery has evolved, with ultra-radical techniques developed in recent years, which can offer potential cure to patients with LRRC, such as high sacrectomy and extended lateral pelvic sidewall excision (ELSiE), are generally accompanied by significant morbidity.12,13,14 In this context, balancing the patients’ existing symptoms, the potential survival benefits to be gained from treatment and their impact on PROs, is essential to enabling patients to make informed decisions regarding their care.
However, it is crucial that the methodological quality of the studies reporting PROs and the PROMs used are sufficient to produce valid and reliable results, particularly in complex disease settings. Validity is the degree to which a PROM measures the construct it purports to measure.15 In a clinical context, such as in measuring health-related quality of life (HrQoL) in patients with LRRC, a PROM can only be considered valid if there is evidence that it has been developed with input from patients with LRRC and provides a comprehensive assessment of HrQoL as the construct of interest, meaning that all aspects of HrQoL that are relevant to patients with LRRC are included. PROMs can be designed as disease-specific or generic, for instance, a generic PROM measures concepts which are broadly relevant to the population, whereas disease-specific PROMs measure concepts specific to a group of patients with a particular condition. To be considered valid in a specific group of patients, both disease-specific and generic PROMs should be shown to have content validity in the group of patients they have been designed for.
The existing evidence concerning PROs in LRRC possesses several limitations from a methodological standpoint, this includes heterogeneity in relation to the groups of patients included, with outcomes frequently reported in combined cohorts of patients with primary and recurrent disease,16,17,18,19 and heterogeneity in comparator groups. In addition to significant variability in the PROMs used and timing of PROM assessment.16,17,18,19 The majority of existing studies are retrospective in nature18 and the evidence is generally low in quality.16,17,18,19,20 Denys et al.’s review focused on patient-centred outcomes following pelvic exenteration for colorectal cancer, including both primary and recurrent disease, also found that the impact of urinary complications, discomfort or pain on sitting and functional disability are inadequately represented in the PROMs currently being used.19
This review sought to evaluate the methodological quality of the existing evidence concerning PROs in LRRC, utilising a systematic approach. The specific aims of the review were to identify the PROMs currently being used to report outcomes in patients with LRRC and to examine the methodological quality of the studies against criteria informed by the Consolidated Standards of Reporting Trials- Patient Reported Outcome (CONSORT-PRO) extension,21,22 and the psychometric properties of the PROMs identified using the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) Risk of Bias checklist.23,24
Methods
This systematic review was conducted using a pre-specified protocol in keeping with Cochrane guidelines,25 and reported in line with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) checklist.26 The review was registered on the international prospective register of systematic reviews, PROSPERO (reference: CRD42022332577).
Eligibility Criteria
Studies in adults (aged ≥ 18) with LRRC that included PROMs as a primary or secondary outcome measure were included. Studies in patients with LRRC undergoing any form of treatment with curative or palliative intent, were eligible for inclusion. Studies in patients with a history of only local excision for primary rectal cancer who developed a regrowth or recurrence were excluded. Only studies published in the English language were considered. Case reports, conference abstracts, study protocols, reviews and letters were excluded.
Information Sources
The search was undertaken using the PubMed, Embase and CINAHL databases, including studies published from 1966 (PubMed), 1980 (Embase) and 1981 (CINAHL) up until 14th September 2022. The search strategy can be found in the supplementary material. Reference searching was also undertaken to identify additional studies. Studies describing the psychometric properties of the PROMs identified from this search were retrieved from citations and through manual searching to enable evaluation of the psychometric properties of the PROMs identified.
Selection Process
Titles and abstracts of studies retrieved were exported to EndNote X9 (Clarivate Analytics, Philadelphia, USA) and duplicates removed. The titles and abstracts were uploaded to Rayyan online software and screened for relevance by two authors (NM and ER). The full text for potentially eligible studies were retrieved and assessed, any queries regarding the eligibility of a study were resolved through discussion with senior authors.
Data collection process
Data concerning the characteristics of the studies included and the quality of the reporting of PROMs against criteria informed by the CONSORT-PRO checklist were extracted independently by authors NM and ER into Excel®. The COSMIN Risk of Bias checklist23 was completed using the Excel® template available from the COSMIN website27 independently by authors NM and FH. Any differences in data extraction or ratings were discussed with senior authors to reach consensus.
Data Items
Quality of Reporting of PROMs
There are currently no checklists available via the Enhancing the QUAlity and Transparency Of health Research (EQUATOR) network regarding the inclusion of PRO data for observational studies. The CONSORT-PRO extension was developed to promote transparent reporting of trials including PROs as primary or secondary outcomes; facilitating the interpretation or PRO results for use in clinical practice.22 The CONSORT-PRO checklist was used to inform the evaluation of studies identified in relation to how the findings were reported and whether the methodology of the study and the PROMs used were sufficient to capture significant and meaningful findings.
PROM Psychometric Properties
The psychometric properties of the PROMs identified were evaluated using the COSMIN Risk of Bias checklist. The COSMIN Risk of Bias checklist for systematic reviews was developed to assess risk of bias of studies on measurement properties of PROMs,23 this information can be used to identify the most appropriate PROM for a specific purpose or study. There are ten criteria (see Figure 1), PROM development and content validity are the first to be assessed, if a PROM is deemed to have insufficient content validity, it should not undergo further assessment. Once sufficient evidence for content validity has been identified, the internal structure and remaining measurement properties are assessed. Studies are qualitatively summarised to give an overall rating of sufficient (+), insufficient (-), inconsistent (±), or indeterminate (?) for each measurement property.28 The quality of the evidence is rated using a modified Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.29

Summary of the COSMIN Risk of Bias Checklist. *Cross-cultural validity was not assessed in this review as the search strategy was not deemed suitable for identifying all studies describing this psychometric property. **The COSMIN panel determined that no gold standard exists for PROMs30 and therefore criterion validity was not assessed in this review.
Risk of Bias Assessment
Risk of bias was assessed using the Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) tool,31 and the revised tool to assess Risk of Bias in randomised trials (RoB 2).32
Data Synthesis
A basic descriptive analysis was undertaken to report the number of patients included in the studies identified and the proportion of patients with LRRC and who contributed to assessments with PROMs.
Results
Study Selection
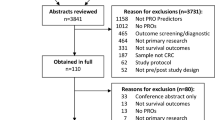
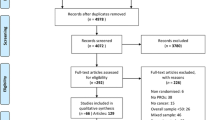
A total of 1475 references were identified; 147 duplicates and 5 animal studies were removed. Abstracts were screened for 1323 references and the full text for 56 references were retrieved. Thirty-one eligible references were included from the search strategy in addition to 4 references identified through manual searching (see Figure 2).

PRISMA flow diagram
Study Characteristics
A summary of the characteristics of the studies is presented in Table 1, including a total of 1914 patients with LRRC across the 35 studies included, of which PROM data was reported for 1104 (57.7%) patients. Twenty-one (63.6%) of the studies identified were published in the last decade. The studies were conducted mostly in Europe (n = 18, 51.4%), Australia (n = 13, 37.1%) or the USA (n = 4, 11.4%), with one study conducted in China (2.9%). Twenty-six (74.3%) studies recruited patients from a single centre. The majority were prospective cohort studies (n = 19, 54.3%) in addition to cross-sectional (n = 7, 20.0%), case-control (n = 5, 14.3%), retrospective cohort (n = 2, 5.7%) and randomised studies (n = 2, 5.7%). Eight (22.9%) of the studies identified included only patients with LRRC, in addition to two (5.7%) case control studies comparing patients with LRRC to other cohorts, with sample sizes of patients with LRRC ranging from 12 to 117 patients. The other 23 (69.7%) studies included combined cohorts of patients with primary and recurrent pelvic disease including LRRC, with sample sizes ranging from 12 to 710 patients in total. Median number of PROM assessments was two (IQR 1). In the 19 prospective, longitudinal studies identified, median follow-up was 12 months (IQR 15) the longest follow-up time point was 8 years.33
Risk of Bias
Risk of bias was high overall, with 32 (91.4%) studies highly or seriously biased (see supplementary Figures 1 and 2).
Results of Individual Studies
Quality of Reporting of PROMs
The assessment of the studies identified against criteria informed by the CONSORT-PRO checklist are illustrated in Figure 3. None of the studies included in the review met all eleven criteria for the quality of reporting of PROMs, with an overall median of 5.8 (58.3%) criteria. The least reported criteria were defining the PROM of interest (n = 3, 8.6%), describing the statistical approach to missing PRO data (n = 6, 17.1%), and detailing a PRO hypothesis (n = 6, 17.1%). The most commonly met criterion was the identification of a PRO as a primary or secondary outcome (n = 35, 100.0%).

Quality of Reporting of PROMS in LRRC
Characteristics of the PROMs Identified
Seventeen PROMs and two clinician-reported outcome measures (MSTS and Spitzer) were identified. The most commonly reported PROMs were the EORTC QLQ-C30 (n = 12, 32.3%),34,36,45,46,48,51,52,53,56,57,61,63 the SF-36 (n = 11, 31.4%),7,35,36,37,38,40,41,43,44,48,55 the FACT-C (n = 10, 28.6%)7,33,35,37,40,41,43,49,55,60 and the EORTC QLQ-CR29 (formerly CR38) (n = 8, 22.9%).34,36,48,51,52,57,61,63
Four of the PROMs identified were specific to patients with cancer (see Table 2), however, there were no disease-specific PROMs for patients with LRRC. The cancer-specific measures included the EORTC QLQ-C30 which is a measure of QoL in patients with cancer and the Functional Living Index – Cancer (FLIC) is a measure of functional state in adult patients with cancer. Two measures which are cancer-site specific were also identified; the EORTC-QLQ CR29 and FACT-C which are both measures of QoL in patients with primary colorectal cancer.
Seven PROMs which relate to forms of function or functional limitations were identified (Table 3), including bowel function, physical function, and sexual function. The Low Anterior Resection Syndrome (LARS) score is a measure to assess bowel dysfunction following low anterior resection for rectal cancer and the St. Mark’s Faecal Incontinence Score for adult patients with faecal incontinence. The Lower Extremity Functional Scale (LEFS) is a measure of lower extremity physical function designed for patients with lower extremity orthopaedic conditions. Four of the measures identified were measures of sexual function, including the Sexual Health Inventory for Men (SHIM) and the International Index of Erectile Function (IIEF) which are measures of erectile dysfunction developed for use in male patients with a history of erectile dysfunction and the Female Sexual Function Index (FSFI) measure of sexual function for female patients with a history of sexual arousal disorder and the Sexual function – Vaginal changes Questionnaire (SVQ) measure of sexual and vaginal problems developed for patients with a history of gynaecological cancer.
Six of the PROMs identified were generic measures (see Table 4), including three measures of QoL for use in adult patients; the 36-Item Short Form Survey (SF-36), EuroQoL (EQ-5D) and Assessment of Quality of Life (AQOL-4D), two measure of pain intensity; the Verbal Numerical Rating Scale (VNRS) and Visual Analogue Scale (VAS), and finally one measure of pain, the Brief Pain Inventory (BPI).
The three remaining measures included (see Table 5), were not patient-reported but clinician reported. Those included the Late Effects of Normal Tissue – Subjective, Objective, Management, and Analytic (LENT-SOMA) scoring system for late effects of radiotherapy, including a subjective scale to be completed by patients with the remainder being completed by clinicians. The Spitzer is a clinician-reported measure of QoL for patients with cancer or other chronic diseases and the Musculoskeletal Tumour Society Score (MSTS) is a clinician-reported measure of physical function for patients with musculoskeletal neoplasms.
PROM Psychometric Properties
The psychometric properties were only assessed for PROMs and not the LENT-SOMA or the clinician-reported outcome measures, Spitzer and MSTS.
Content Validity
None of the PROMs identified were developed specifically for patients with LRRC (Tables 2, 3, 4 and 5) and no studies were identified in which the psychometric properties of these PROMs were evaluated in patients with LRRC.
Internal Structure and Remaining Measurement Properties
Content validity is the most important measurement property of a PROM and therefore full review is not advised if a PROM does not meet criteria for content validity.
Discussion
There has been an expansion in PROMs reporting in LRRC, with several papers (n = 21, 63.6%) published in the last decade. However, despite this increase, these studies are methodologically limited due to the use of non-validated measures used to assess PROs in this cohort of patients. This systematic review did not identify a disease-specific PROM available for use in LRRC and none of the PROMs identified met the COSMIN criteria for content validity in the context of LRRC. The most used PROMS in LRRC were the FACT-C (n = 10, 28.6%), SF-36 (n = 11, 31.4%) EORTC QLQ-C30 (n = 12, 34.3%) and CR29 (n = 8, 22.9%), none of which have demonstrated content validity specifically for patients with LRRC.
Overall, the findings build on the existing evidence16,17,18,19 of variable methodological quality of reporting of PROMs within small sample sizes and mixed disease cohorts. This review focuses specifically on the methodological quality of PRO reporting using criteria informed by the CONSORT-PRO checklist; common weaknesses were identified in several domains, including defining the PRO of interest, describing the statistical approach to missing data and stating PRO-specific limitations and implications for generalisability. These results were comparable to those reported in Efficace et al.’s pooled analysis of randomised cancer trials utilising CONSORT-PRO,76 though methods of PRO data collection had higher levels of reporting in this current review. Ultimately, the key limitation identified is the lack of input from patients with LRRC in the PROMs currently being used, with none demonstrating content validity for use in this context. Content validity is the most important measurement property of a PROM; for PROMs to give meaningful results in LRRC, it is essential that they are relevant to patients with LRRC and present a comprehensive assessment of the construct of interest. Without addressing the lack of an appropriate PROM for use in patients with LRRC, the impact of addressing issues such as heterogeneity in the groups of patients included, the comparator groups used, and the timing of PROM assessment, is likely to be limited.
Harji et al. reported the development of the Locally Recurrent Rectal Cancer – Quality of Life (LRRC-QoL) conceptual framework through undertaking a systematic review and qualitative focus groups to identify the HrQoL issues relevant to patients with LRRC.18,77 The themes identified were symptoms, sexual function, psychological impact, role and social functioning, future perspective and healthcare service utilisation and delivery. Nineteen (54.3%) of the studies identified in this review have been published since this work,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51 using a median of two PROMS, with the EORTC QLQ-CR29 and FACT-C most used. The EORTC QLQ-CR29 and FACT-C have also both demonstrated robust psychometric properties, including content validity, in patients with primary colorectal cancer.78,79 When compared with the LRRC-QoL conceptual framework,77 the EORTC QLQ-CR29 covers 50% of the LRRC-specific domains, including symptoms, sexual function, and psychological impact. It does not however cover the domains of role functioning, or future perspective. The FACT-C covers 66.6% of the LRRC-specific domains identified in the LRRC-QoL conceptual framework including symptoms, psychological impact, role functioning, and future perspective, it does not cover sexual function. Neither the EORTC QLQ-CR29 or FACT-C cover issues relating to healthcare services, self-efficacy and body image, future plans, disease re-recurrence, gynaecological or locomotor symptoms. The evidence identified reporting outcomes utilising these PROMs should not be completely disregarded, as the EORTC QLQ-CR29 and FACT-C capture a proportion of the issues relevant to patients with LRRC. However, it should be interpreted with caution, as they are unlikely to capture the full scope and complexity of the range of issues patients with LRRC experience.18,77
A number of PROMs which measure issues relevant to patients with LRRC were identified in this review; urinary and sexual function were evaluated using specific questionnaires for this purpose by two studies,36,53 however, other questionnaires, such as the EORTC QLQ-CR29, also contain items concerning sexual and urinary function. No specific PROMs concerning stoma-related quality of life were used in the studies identified, despite being relevant to patients with LRRC.77 However, PROMs such as the EORTC QLQ-CR29 and FACT-C contain items specifically for patients with stomas. The increasing number of PROMs currently being used in LRRC reflects the lack of an existing disease-specific measure which adequately reports all the PROs relevant to this cohort of patients. The trend to include several PROMs is likely to reflect the greater understanding of the wider issues which affect patients with LRRC. However, the measures identified in this review are not valid for use in patients with LRRC and therefore this is not a psychometrically robust approach to addressing the lack of a LRRC disease-specific measure. Additionally, this approach potentially increases the burden of participation for patients, without sufficient methodological justification.
There are limitations related to the evidence included in this review, notably, most of the studies identified have a high risk of bias (n = 32, 91.4%) and their findings should generally be interpreted with caution. They also present a predominately Western perspective of PROs in LRRC and demonstrate a lack of multi-centre, international reporting of PROs in LRRC. Furthermore, 13 (37.1%) of the studies identified were conducted within a single centre, reporting cohorts of patients which may potentially overlap. It was not possible to assess the availability and quality of translated PROMs in this review, however, to further the success of initiatives such as the PelvEx collaborative in advancing international outcome reporting in this cohort of patients80 and integrating PRO data, it is essential that PROMs undergo a rigorous process of cross-cultural adaption.
There are several approaches which could be employed to address the lack of PROMs with content validity for patients with LRRC. It is possible to demonstrate the content validity of existing PROMS specifically for LRRC, however, given the narrow breadth of relevant HrQoL issues captured by existing measures, this approach will require significant revision to make these measures applicable to LRRC.77 Employing a modular approach to PROM assessment to LRRC is an alternative approach, provided both the core cancer and site-specific measures are appropriately revised and validated for use in LRRC. Development of a new disease-specific PROMs for use in patients with LRRC, to capture concerns that are specific to patients with LRRC which can be used to more accurately monitor the impact of particular treatments on PROs such as HrQoL is likely to be the most realistic and valid approach.81 The development of the LRRC-QoL PROM will build on the development of the LRRC-QoL conceptual framework.77 The LRRC-QoL is the first disease-specific PROM developed for use in patients with LRRC82 and has been designed to be used in combination with EORTC QLQ-C30, in a modular fashion, which would allow comparison across patient groups. Recruitment to a study to externally validate the LRRC-QoL for use internationally is currently underway (ISRCTN13692671) and includes a robust cross-cultural adaptation process to produce versions of the LRRC-QoL for use in several countries.
Conclusion
This systematic review highlights key methodological issues in the current state of reporting of PROs in LRRC, finding that none of the PROMs currently being used in LRRC are able to provide meaningful results within this context. Future studies in this disease area should focus on utilising PROMs that have undergone a robust development process with the inclusion of patients with LRRC, to ensure high quality, accurate results which are relevant to this patient group. The development of a disease-specific PROM for patients with LRRC or undertaking content validity studies of existing PROMs are approaches which could be employed to enable this, in addition to undertaking cross-cultural adaptation to enable international reporting of outcomes. Greater emphasis should also be placed on the way in which PROMs data are reported and analysed, particularly in defining the PRO of interest and in handling missing PROM data, to ensure that results are reliable.
References
Movsas B, Moughan J, Sarna L, et al. Quality of life supersedes the classic prognosticators for long-term survival in locally advanced non-small-cell lung cancer: an analysis of RTOG 9801. J Clin Oncol. 2009;27(34):5816–22.
Coates A, Porzsolt F, Osoba D. Quality of life in oncology practice: Prognostic value of EORTC QLQ-C30 scores in patients with advanced malignancy. Eur J Cancer. 1997;33(7):1025–30.
Maisey NR, Norman A, Watson M, Allen MJ, Hill ME, Cunningham D. Baseline quality of life predicts survival in patients with advanced colorectal cancer. Eur J Cancer. 2002;38(10):1351–7.
Absolom K, Warrington L, Hudson E, et al. Phase III randomized controlled trial of eRAPID: eHealth intervention during chemotherapy. J Clin Oncol. 2021;39(7):734–47.
Denis F, Basch E, Septans A-L, et al. Two-year survival comparing web-based symptom monitoring vs routine surveillance following treatment for lung cancer. JAMA. 2019;321(3):306–7.
Basch E, Deal AM, Dueck AC, et al. Overall survival results of a trial assessing patient-reported outcomes for symptom monitoring during routine cancer treatment. JAMA. 2017;318(2):197–8.
Huang Y, Steffens D, Koh CE, Young JM, Solomon MJ. Differences in surgical outcomes and quality of life outcomes in pelvic exenteration between locally advanced versus locally recurrent rectal cancer. Dis Colon Rectum. 2022;65(12):1475–82.
Palmer G, Martling A, Cedermark B, Holm T. A population-based study on the management and outcome in patients with locally recurrent rectal cancer. Ann Surg Oncol. 2007;14(2):447–54.
Hagemans JAW, van Rees JM, Alberda WJ, et al. Locally recurrent rectal cancer; long-term outcome of curative surgical and non-surgical treatment of 447 consecutive patients in a tertiary referral centre. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2019:S0748-7983(0719)30917-30915
Westberg K, Palmer G, Hjern F, Johansson H, Holm T, Martling A. Management and prognosis of locally recurrent rectal cancer—a national population-based study. Eur J Surg Oncol : J Eur Soc Surg Oncol Br Assoc Surg Oncol. 2018;44(1):100–7.
You YN, Roses RE, Chang GJ, et al. Multimodality salvage of recurrent disease after local excision for rectal cancer. Dis Colon Rectum. 2012;55(12):1213–9.
Nielsen MB, Laurberg S, Holm T. Current management of locally recurrent rectal cancer. Colorectal Dis. 2011;13(7):732–42.
Heriot AG, Byrne CM, Lee P, et al. Extended radical resection: the choice for locally recurrent rectal cancer. Dis Colon Rectum. 2008;51(3):284–91.
Harris CA, Solomon MJ, Heriot AG, et al. The outcomes and patterns of treatment failure after surgery for locally recurrent rectal cancer. Ann Surg. 2016;264(2):323–9.
Mokkink LB, Terwee CB, Patrick DL, et al. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J Clin Epidemiol. 2010;63(7):737–45.
Thaysen HV, Jess P, Laurberg S. Health-related quality of life after surgery for primary advanced rectal cancer and recurrent rectal cancer—a review. Colorectal Dis Off J Assoc Coloproctol Great Br Irel. 2012;14:797–803.
Glyn T, Frizelle F. Quality of life outcomes in patients undergoing surgery for locally recurrent rectal cancer. Semin Colon Rectal Surg. 2020;31(3):100767.
Harji DP, Griffiths B, Velikova G, Sagar PM, Brown J. Systematic review of health-related quality of life issues in locally recurrent rectal cancer. J Surg Oncol. 2015;111:431–8.
Denys A, van Nieuwenhove Y, Van de putte D, et al. Patient-reported outcomes after pelvic exenteration for colorectal cancer: A systematic review. Colorectal Dis. 2021;24(4):353–68.
Collaborative TP. Palliative pelvic exenteration: a systematic review of patient-centered outcomes. Eur J Surg Oncol. 2019;45(10):1787–95.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–7.
Calvert M, Blazeby J, Altman DG, et al. Reporting of patient-reported outcomes in randomized trials: the CONSORT PRO extension. JAMA. 2013;309(8):814–22.
Mokkink LB, de Vet HCW, Prinsen CAC, et al. COSMIN risk of Bias checklist for systematic reviews of patient-reported outcome measures. Qual Life Res. 2018;27(5):1171–9.
Terwee CB, Prinsen CAC, Chiarotto A, et al. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Qual Life Res. 2018;27(5):1159–70.
Higgins JPTTJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions. In: Higgins JPT TJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, ed. 2nd Edition ed: Cochrane 2022; 2022: www.training.cochrane.org/handbook.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
COSMIN. COSMIN Tools. 2021; https://www.cosmin.nl/tools/guideline-conducting-systematic-review-outcome-measures/?portfolioCats=19. Accessed 28.04.2021, 2021.
Terwee CB, Mokkink LB, Knol DL, Ostelo RWJG, Bouter LM, de Vet HCW. Rating the methodological quality in systematic reviews of studies on measurement properties: a scoring system for the COSMIN checklist. Qual Life Res. 2012;21(4):651–7.
GRADE Handbook. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach. 2013; https://gdt.gradepro.org/app/handbook/handbook.html. Accessed 11/01/2022, 2022.
Mokkink LB, Terwee CB, Knol DL, et al. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: a clarification of its content. BMC Med Res Methodol. 2010;10:22.
Sterne JAC, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919.
Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
You YN, Habiba H, Chang GJ, Rodriguez-bigas MA, Skibber JM. Prognostic value of quality of life and pain in patients with locally recurrent rectal cancer. Ann Surg Oncol. 2011;18(4):989–96.
Westerduin E, Elfeki H, Frontali A, et al. Functional outcomes and quality of life after redo anastomosis in patients with rectal cancer—an international multicenter comparative cohort study. Dis Colon Rectum. 2021;64(7):822–32.
Alahmadi R, Steffens D, Solomon MJ, Lee PJ, Austin KKS, Koh CE. Elderly patients have better quality of life but worse survival following pelvic exenteration: a 25-year single-center experience. Ann Surg Oncol. 2021;28:5226–35.
McCarthy ASE, Solomon MJ, Koh CE, Firouzbakht A, Jackson SA, Steffens D. Quality of life and functional outcomes following pelvic exenteration and sacrectomy. Colorectal Dis. 2020;22(5):521–8.
van Ramshorst GH, Young JM, Solomon MJ. Complications and impact on quality of life of vertical rectus abdominis myocutaneous flaps for reconstruction in pelvic exenteration surgery. Dis Colon Rectum. 2020;63(9):1225–33.
Denost Q, Solomon M, Tuech J-J, et al. International variation in managing locally advanced or recurrent rectal cancer: prospective benchmark analysis. Br J Surg. 2020;107(13):1846–54.
Smith T, O’Cathail SM, Silverman S, et al. Stereotactic body radiation therapy reirradiation for locally recurrent rectal cancer: outcomes and toxicity. Adv Radiat Oncol. 2020;5(6):1311–9.
Brown KGM, Solomon MJ, Lau YC, Steffens D, Austin KKS, Lee PJ. Sciatic and femoral nerve resection during extended radical surgery for advanced pelvic tumours: long-term survival, functional, and quality-of-life outcomes. Ann Surg. 2021;273(5):982–8.
Steffens D, Solomon MJ, Young JM, et al. Cohort study of long-term survival and quality of life following pelvic exenteration. BJS Open. 2018;2(5):328–35.
Lim S-YJ, Koh EC, Liu JH, Solomon SHM, Johnstone SHC. The price we pay for radical curative pelvic exenterations: prevalence and management of pain. Dis Colon Rectum. 2018;61(3):314–9.
Choy I, Young JM, Badgery-Parker T, et al. Baseline quality of life predicts pelvic exenteration outcome. ANZ J Surg. 2017;87(11):935–9.
Quyn JA, Solomon JM, Lee MP, Badgery-Parker MT, Masya ML, Young MJ. Palliative pelvic exenteration: clinical outcomes and quality of life. Dis Colon Rectum. 2016;59(11):1005–10.
Cameron MG, Kersten C, Vistad I, et al. Palliative pelvic radiotherapy for symptomatic rectal cancer – a prospective multicenter study. Acta Oncol. 2016;55(12):1400–7.
Pellino G, Sciaudone G, Candilio G, Selvaggi F. Effect of surgery on health-related quality of life of patients with locally recurrent rectal cancer. Dis Colon Rectum. 2015;58(8):753–61.
Li W, Ye X, Yang X, et al. Microwave ablation as palliative treatment of locally recurrent colorectal cancer. Indian J Cancer. 2015;52(Suppl 2):e61-63.
Thaysen HV, Jess P, Rasmussen PC, Nielsen MB, Laurberg S. Health-related quality of life after surgery for advanced and recurrent rectal cancer—a nationwide prospective study. Colorectal Dis. 2014;16(7):O223–33.
Beaton J, Carey S, Solomon MJ, Tan K-K, Young J. Preoperative body mass index, 30-day postoperative morbidity, length of stay and quality of life in patients undergoing pelvic exenteration surgery for recurrent and locally-advanced rectal cancer. Ann Coloproctol. 2014;30(2):83–7.
Pusceddu C, Sotgia B, Melis L, Fele RM, Meloni GB. Painful pelvic recurrence of rectal cancer: percutaneous radiofrequency ablation treatment. Abdom Imaging. 2013;38(6):1225–33.
Traa MJ, Orsini RG, Oudsten BLD, et al. Measuring the health-related quality of life and sexual functioning of patients with rectal cancer: does type of treatment matter? Int J Cancer. 2014;134(4):979–87.
Holman FA, Martijnse IS, Traa MJ, et al. Dynamic article: vaginal and perineal reconstruction using rectus abdominis myocutaneous flap in surgery for locally advanced rectum carcinoma and locally recurrent rectum carcinoma. Dis Colon Rectum. 2013;56(2):175–85.
Brændengen M, Tveit KM, Bruheim K, Cvancarova M, Berglund Å, Glimelius B. Late patient-reported toxicity after preoperative radiotherapy or chemoradiotherapy in nonresectable rectal cancer: results from a randomized phase III study. Int J Radiat Oncol, Biol, Phys. 2011;81(4):1017–24.
Haapamäki MM, Pihlgren V, Lundberg O, Sandzén B, Rutegård J. Physical performance and quality of life after extended abdominoperineal excision of rectum and reconstruction of the pelvic floor with gluteus maximus flap. Dis Colon Rectum. 2011;54(1):101–6.
Austin KKS, Young JM, Solomon MJ. Quality of life of survivors after pelvic exenteration for rectal cancer. Dis Colon Rectum. 2010;53(8):1121–6.
Zoucas E, Frederiksen S, Lydrup M-L, Månsson W, Gustafson P, Alberius P. Pelvic exenteration for advanced and recurrent malignancy. World J Surg. 2010;34(9):2177–84.
Palmer G, Martling A, Lagergren P, Cedermark B, Holm T. Quality of life after potentially curative treatment for locally advanced rectal cancer. Ann Surg Oncol. 2008;15(11):3109–17.
Miner TJ, Jaques DP, Paty PB, Guillem JG, Wong WD. Symptom control in patients with locally recurrent rectal cancer. Ann Surg Oncol. 2003;10(1):72–9.
Mannaerts GHH, Rutten HJT, Martijn H, Hanssens PEJ, Wiggers T. Effects on functional outcome after IORT-containing multimodality treatment for locally advanced primary and locally recurrent rectal cancer. Int J Radiat Oncol Biol Phys. 2002;54(4):1082–8.
Esnaola NF, Cantor SB, Johnson ML, et al. Pain and quality of life after treatment in patients with locally recurrent rectal cancer. J Clin Oncol : Off J Am Soc Clin Oncol. 2002;20(21):4361–7.
Camilleri-Brennan J, Steele RJC. The impact of recurrent rectal cancer on quality of life. Eur J Surg Oncol (EJSO). 2001;27(4):349–53.
Mannaerts GHH, Schijven MP, Hendrikx A, Martijn H, Rutten HJT, Wiggers T. Urologic and sexual morbidity following multimodality treatment for locally advanced primary and locally recurrent rectal cancer. Eur J Surg Oncol (EJSO). 2001;27(3):265–72.
Guren MG, Wiig JN, Dueland S, et al. Quality of life in patients with urinary diversion after operation for locally advanced rectal cancer. Eur J Surg Oncol (EJSO). 2001;27(7):645–51.
Trotter JM, Edis AJ, Blackwell JB, et al. Adjuvant VHF therapy in locally recurrent and primary unresectable rectal cancer. Australas Radiol. 1996;40(3):298–305.
Scheithauer W, Rosen H, Kornek GV, Sebesta C, Depisch D. Randomised comparison of combination chemotherapy plus supportive care with supportive care alone in patients with metastatic colorectal cancer. BMJ (Clinical Research ed). 1993;306(6880):752–5.
Wanebo HJ, Gaker DL, Whitehill R, Morgan RF, Constable WC. Pelvic recurrence of rectal cancer. Options for curative resection. Ann Surg. 1987;205(5):482–95.
Life EQo. Quality of Life of Cancer Patients Translations. Questionnaires https://qol.eortc.org/questionnaire/eortc-qlq-c30/. Accessed 19.05.2022, 2022.
ePROVIDE™. Instruments https://eprovide.mapi-trust.org/advanced-search. Accessed 19.05.2022, 2022.
Life EQo. Colorectal. Questionnaires https://qol.eortc.org/questionnaire/qlq-cr29/. Accessed 19.05.2022, 2022.
FACIT. FACT-C Languages. 2021; https://www.facit.org/measure-languages/FACT-C-Languages. Accessed 19.05.2022, 2022.
ESCP. The LARS Score - Therese Juul https://www.escp.eu.com/news/focus-on/beyond-colorectal-cancer/1579-lars-score. Accessed 19.09.2022, 2022.
RAND. 36-Item Short Form Survey (SF-36). RAND Medical Outcomes Study 2022; https://www.rand.org/health-care/surveys_tools/mos/36-item-short-form.html. Accessed 19.05.2022, 2022.
EuroQol. EQ-5D-5L / Self-complete version on paper. EQ-5D-5L 2022; https://euroqol.org/eq-5d-instruments/eq-5d-5l-available-modes-of-administration/self-complete-on-paper/. Accessed 19.05.2022, 2022.
Life AAoQo. AQoL Available Languages. 2014; http://www.aqol.com.au/index.php/aqol-translations. Accessed 19.05.2022, 2022.
Center MAC. The Brief Pain Inventory. Symptom Assessment Tools 2022; https://www.mdanderson.org/research/departments-labs-institutes/departments-divisions/symptom-research/symptom-assessment-tools/brief-pain-inventory.html. Accessed 19.05.2022, 2022.
Efficace F, Fayers P, Pusic A, et al. Quality of patient-reported outcome reporting across cancer randomized controlled trials according to the CONSORT patient-reported outcome extension: a pooled analysis of 557 trials. Cancer. 2015;121(18):3335–42.
Harji DP, Koh C, Solomon M, Velikova G, Sagar PM, Brown J. Development of a conceptual framework of health-related quality of life in locally recurrent rectal cancer. Colorectal Dis : Off J Assoc Coloproctol Great Br Irel. 2015;17(11):954–64.
Ward W, Hahn E, Mo F, Hernandez L, Tulsky D, Cella D. Reliability and validity of the functional assessment of cancer therapy-colorectal (FACT-C) quality of life instrument. Qual Life Res. 1999;8(3):181–95.
Whistance RN, Conroy T, Chie W, et al. Clinical and psychometric validation of the EORTC QLQ-CR29 questionnaire module to assess health-related quality of life in patients with colorectal cancer. Eur J Cancer. 2009;45(17):3017–26.
Collaborative TP. Factors affecting outcomes following pelvic exenteration for locally recurrent rectal cancer. J Br Surg . 2018;105(6):650–7.
Pfennings LEMA, van der Ploeg HM, Cohen L, Polman CH. A comparison of responsiveness indices in multiple sclerosis patients. Qual Life Res. 1999;8(6):481–9.
Harji DP. The Development and Validation of a Patient-Reported Outcome Measure of Health-Related Quality of Life in Locally Recurrent Rectal Cancer, University of Leeds; 2017.
Funding
Funding for this work was provided by Bowel Research UK and Pelican Cancer Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Prof. Galina Velikova, Honoraria: Pfizer, Novartis, Eisai, Advisory boards: Consultancy fees from AstraZeneca, Roche, Novartis, Pfizer, Seagen, Eisai, Sanofi Institutional grant from Pfizer.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
McKigney, N., Houston, F., Ross, E. et al. Systematic Review of Patient-Reported Outcome Measures in Locally Recurrent Rectal Cancer. Ann Surg Oncol 30, 3969–3986 (2023). https://doi.org/10.1245/s10434-023-13388-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-023-13388-5