
Abstract
Background
Surgical outcome after pancreatoduodenectomy for duodenal adenocarcinoma could differ from pancreatoduodenectomy for other cancers, but large multicenter series are lacking. This study aimed to determine surgical outcome in patients after pancreatoduodenectomy for duodenal adenocarcinoma, compared with other periampullary cancers, in a nationwide multicenter cohort.
Methods
After pancreatoduodenectomy for cancer between 2014 and 2019, consecutive patients were included from the nationwide, mandatory Dutch Pancreatic Cancer Audit. Patients were stratified by diagnosis. Baseline, treatment characteristics, and postoperative outcome were compared between groups. The association between diagnosis and major complications (Clavien–Dindo grade III or higher) was assessed via multivariable regression analysis.
Results
Overall, 3113 patients, after pancreatoduodenectomy for cancer, were included in this study: 264 (8.5%) patients with duodenal adenocarcinomas and 2849 (91.5%) with other cancers. After pancreatoduodenectomy for duodenal adenocarcinoma, patients had higher rates of major complications (42.8% vs. 28.6%; p < 0.001), postoperative pancreatic fistula (International Study Group of Pancreatic Surgery [ISGPS] grade B/C; 23.1% vs. 13.4%; p < 0.001), complication-related intensive care admission (14.3% vs. 10.3%; p = 0.046), re-interventions (39.8% vs. 26.6%; p < 0.001), in-hospital mortality (5.7% vs. 3.1%; p = 0.025), and longer hospital stay (15 days vs. 11 days; p < 0.001) compared with pancreatoduodenectomy for other cancers. In multivariable analysis, duodenal adenocarcinoma was independently associated with major complications (odds ratio 1.14, 95% confidence interval 1.03–1.27; p = 0.011).
Conclusion
Pancreatoduodenectomy for duodenal adenocarcinoma is associated with higher rates of major complications, pancreatic fistula, re-interventions, and in-hospital mortality compared with patients undergoing pancreatoduodenectomy for other cancers. These findings should be considered in patient counseling and postoperative management.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
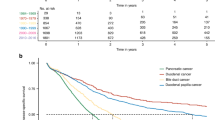
Duodenal adenocarcinoma is a rare disease with a rising incidence.1 Locoregional duodenal and other periampullary cancers are primarily treated by pancreatoduodenectomy and, potentially, adjuvant chemotherapy.1,2,3 Tumor morphology of duodenal adenocarcinoma demonstrates an intestinal-type differentiation, resembling colorectal cancer, while most other periampullary cancers have a pancreaticobiliary-type differentiation.4 Better overall survival has been reported for patients with duodenal adenocarcinoma compared with patients with other periampullary cancers.4,5
Mortality after pancreatoduodenectomy has decreased over the last decades. Reported in-hospital mortality rates are < 5% in specialized centers,6,7 which is partially due to centralization of the operation, with pancreatoduodenectomy being increasingly performed in high-volume centers,8 and better management of major complications such as postoperative pancreatic fistula (POPF) and their sequalae, abdominal sepsis, and post-pancreatectomy hemorrhage (PPH).9,10 While mortality rates for pancreatoduodenectomy have decreased considerably, postoperative morbidity rates can still reach up to 67%.11,12,13
In surgical series on pancreatoduodenectomy, outcomes for patients with duodenal adenocarcinoma are often combined with other periampullary cancers because of their low incidence.14,15,16 This results in limited knowledge of postoperative mortality and complication rates after pancreatoduodenectomy for duodenal adenocarcinoma. However, adequate identification of perioperative risk factors is pivotal for clinicians to better select patients with duodenal adenocarcinoma for curative resection and adequately counsel patients. The aim of this multicenter, nationwide audit-based study was to determine the postoperative morbidity and mortality after pancreatoduodenectomy for duodenal adenocarcinoma compared with other periampullary cancers.
Methods
After pancreatoduodenectomy for duodenal adenocarcinoma and other periampullary cancers (pancreatic ductal adenocarcinoma, distal cholangiocarcinoma, and ampullary cancer) between 2014 and 2019, consecutive patients were included from the nationwide mandatory Dutch Pancreatic Cancer Audit (DPCA). This audit covers all pancreatic resections and demonstrates high accuracy and case ascertainment.17 In this study, only patients with adenocarcinoma were included based on final postoperative histopathology. The duodenal adenocarcinoma group included patients with a final diagnosis of duodenal adenocarcinoma, which did not include (intestinal type) ampullary carcinoma. Neither informed consent nor ethical approval for this study were required since the data are anonymously registered. Complication rates, hospital stay, and mortality after pancreatoduodenectomy were compared for duodenal adenocarcinoma and other periampullary cancers.
Definitions
Postoperative complications were classified according to the Clavien–Dindo classification, of which only complications with at least grade IIIa were included (i.e., major complications). Pancreatic surgery-specific complications were scored according to the International Study Group of Pancreatic Surgery (ISGPS) definitions for POPF, post-pancreatectomy hemorrhage, delayed gastric emptying (DGE), and bile leakage.18,19,20,21 Only clinically relevant complications, defined as grade B/C, were included.
Endpoints
The primary endpoint was the rate of major complications (Clavien–Dindo grade III or higher), while secondary endpoints included length of stay, in-hospital mortality rates, and pancreatic-specific complications.
Statistical Analysis
Normally distributed continuous data were presented as means with standard deviations (SDs) and were compared using Student’s t-test. Non-normally distributed continuous data were expressed as medians with interquartile ranges (IQR) and assessed using the Mann–Whitney U test. Categorical data were presented in frequencies with percentages and analyzed using the Chi-square test. Multivariable complete-case logistic regression analyses, adjusted for all relevant confounders based on literature and expert opinion, was performed to assess the association between diagnosis and major complications (Clavien–Dindo grade III or higher). Confounders were patient characteristics (sex, age, body mass index [BMI], preoperative weight loss, and American Society of Anesthesiologists [ASA] score), perioperative care (neoadjuvant treatment, preoperative biliary drainage, perioperative use of octreotide), and intraoperative findings (pancreatic texture and diameter of the pancreatic duct).
Results
Baseline Characteristics
Overall, 3113 consecutive patients, after pancreatoduodenectomy for cancer, were included: 264 (9%) patients with duodenal adenocarcinomas and 2849 (91%) patients with other periampullary cancers, including 1753 (56%) patients with pancreas ductal adenocarcinomas, 546 (17%) patients with distal cholangiocarcinomas, and 550 (18%) patients with ampullary cancers. Baseline characteristics are summarized in Table 1. Patient characteristics (e.g., sex and age) did not differ between duodenal adenocarcinomas and other periampullary cancers. After pancreatoduodenectomy for duodenal adenocarcinoma, patients had less preoperative weight loss (4 vs. 5 kg; p = 0.018) and less often underwent preoperative biliary drainage (14% vs. 64%; p < 0.001).
Surgical Outcome
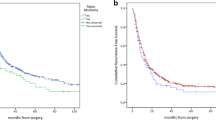
Postoperative complications and mortality are shown in Table 2. In total, 929 (29.8%) patients experienced major complications, which were more often seen after pancreatoduodenectomy for duodenal adenocarcinoma (42.8% vs. 28.6%; p < 0.001), compared with other periampullary cancers.
In-hospital mortality was higher in patients with duodenal adenocarcinoma (5.7% vs. 3.1%; p = 0.025). Re-intervention was more common in patients with duodenal adenocarcinoma (39.8% vs. 26.6%; p < 0.001), especially regarding radiologic drainage (28.3% vs. 17.6%; p < 0.001), and complications leading to intensive care admission occurred more often in patients with duodenal adenocarcinoma (14.3% vs. 10.3%; p = 0.046). Median length of hospital stay was longer for patients with duodenal adenocarcinoma in comparison with other periampullary cancers (15 days [IQR 9–24] vs. 11 days [IQR 8–17]; p < 0.001). Subgroup analysis of postoperative outcome stratified by diagnosis is shown in electronic supplementary Table 1.
Multivariable Analysis for Major Complications
Overall, 1881 patients were included in the multivariable logistic regression analysis for the development of major complications (Table 3). Multivariable analysis identified male sex (odds ratio [OR] 1.31, 95% confidence interval [CI] 1.04–1.64; p = 0.022), ASA score of III or higher (OR 1.64, 95% CI 1.05–2.56; p = 0.031), pancreatic texture (OR 0.65, 95% CI 0.51–0.83; p = 0.001), pancreatic duct diameter (OR 0.93, 95% CI 0.89–0.97; p < 0.001), and duodenal adenocarcinoma (OR 1.14, 95% CI 1.03–1.27; p = 0.011) as independent factors influencing the development of major complications.
Discussion
This first multicenter nationwide study on surgical outcome after pancreatoduodenectomy for duodenal adenocarcinoma found more major complications, more re-interventions, longer postoperative stay, and higher mortality compared with pancreatoduodenectomy for other periampullary cancers.
Only a few, mostly small, monocenter studies reported on surgical outcome after pancreatoduodenectomy for duodenal adenocarcinoma and compared these with outcomes for other periampullary tumors.14,15,22,23,24,25,26,27 An overview of these studies, based on a systematic search, is shown in Table 4. The reported rates of major complications after PD for duodenal adenocarcinoma varied between 18 and 24%.14,15,27 Some of these studies included only patients with duodenal adenocarcinoma, whereas others performed a subgroup analysis within a larger cohort. None of these studies included all endpoints reported in the current study. The higher rate of major complications found in the present study may be related to the prospective nature of the DPCA. Moreover, the current study may better reflect more daily clinical practice than monocenter studies.
Multivariable analysis confirmed the positive correlation between high ASA score, soft pancreatic texture, small pancreatic duct diameter, and the occurrence of major complications.28,29 It is widely recognized that soft pancreatic texture and small diameter of the pancreatic duct are associated with POPF; however, this study confirms that both are also associated with major complications. Patients with duodenal adenocarcinoma usually have both these risk factors, which poses them at greater risk for complications.15,26 However, in the present analysis, even after adjustment for pancreatic texture and duct diameter, duodenal adenocarcinoma as an indication for pancreatoduodenectomy remained an independent risk factor for postoperative complications.
In the current study, somatostatin analogs (octreotide or pasireotide) were used more often in patients with duodenal adenocarcinoma (67% vs. 60%; p = 0.03); however, the value of these agents in preventing POPF in all patients undergoing a pancreatoduodenectomy remains debated.30,31 Based on our results, no benefit of somatostatin use was observed in patients after pancreatoduodenectomy for duodenal adenocarcinoma.
Neoadjuvant or induction chemotherapy, radiotherapy, or a combination has been more frequently provided for patients with pancreatic cancer over the last decade, which also affects patients included in the current analysis. Neoadjuvant therapy could impact the texture of pancreatic tissue, which has been associated with reduced rates of POPF.32
The results of the present study should be interpreted considering several limitations. First, there was potential information bias regarding the lack of information on patient’s preoperative nutritional status as no data on nutritional status are available in the nationwide, prospectively recorded DPCA. Preoperative nutrition status in pancreatic surgery has been recognized as a significant variable in postoperative mortality and morbidity.33 Malignancies such as PDAC are widely recognized to be associated with cachexia and malnutrition.34 Jaundice, exocrine insufficiency, and weight loss are the most common preoperative findings noted in patients with PDAC.35,36 A gastric outlet obstruction caused by duodenal adenocarcinoma can lead to cachexia and malnutrition, which further impairs nutrition status. Second, although all complications are registered during hospital admission or within 30 days postoperatively, no information was available on the exact timing in which complications in the present study population were diagnosed and/or treated. Third, data on bile duct diameter were not available; however, it seems likely that the higher rate of bile leak is related to less-dilated bile ducts in patients with duodenal adenocarcinoma compared with other patients undergoing pancreatoduodenectomy. Fourth, during the majority of the study period, the Dutch hospitals had no uniform postoperative algorithm for detecting and treating complications. Such a protocol has recently been implemented during the nationwide PORSCH trial, which included patients with duodenal adenocarcinoma and reduced mortality after pancreatic surgery.37 Fifth, no data on adjuvant chemotherapy were available. Major morbidity could influence the rate of adjuvant chemotherapy, for instance, in patients with positive nodal status. Efforts are underway to couple the DPCA to the Dutch cancer registry, allowing for such analyses.
Ways to reduce the relatively high rates of major complications after pancreatoduodenectomy for duodenal adenocarcinoma should be the subject of further investigation. Preventive measurements such as preoperative prehabilitation could potentially contribute in this manner.38 The role of somatostatin analogs in the prevention of POPF remains unclear.30,39 An intervention to alter the pancreatic texture using stereotactic radiotherapy is currently being investigated in the multicenter phase II FIBROPANC trial (NL9299).
Conclusion
Pancreatoduodenectomy for duodenal adenocarcinoma is associated with higher rates of major complications and in-hospital mortality compared with patients undergoing pancreatoduodenectomy for other periampullary cancers. This finding is relevant when counseling patients with duodenal adenocarcinoma undergoing pancreatoduodenectomy and optimizing postoperative treatment strategies.
Data Availability
The authors had complete access to the study data that support this publication. All relevant data are within the paper and its electronic supplementary files. Data, analytic methods, and study materials can be made available to other researchers on reasonable request.
References
Bilimoria KY, Bentrem DJ, Wayne JD, Ko CY, Bennett CL, Talamonti MS. Small bowel cancer in the United States: changes in epidemiology, treatment, and survival over the last 20 years. Ann Surg. 2009;249(1):63–71.
Meijer LL, Alberga AJ, de Bakker JK, van der Vliet HJ, Le Large TYS, van Grieken NCT, de Vries R, Daams F, Zonderhuis BM, Kazemier G. Outcomes and treatment options for duodenal adenocarcinoma: a systematic review and meta-analysis. Ann Surg Oncol. 2018;25(9):2681–92.
Ahn DH, Bekaii-Saab T. Ampullary cancer: an overview. Am Soc Clin Oncol Educ Book 2014: 112-115.
Delaunoit T, Neczyporenko F, Limburg PJ, Erlichman C. Pathogenesis and risk factors of small bowel adenocarcinoma: a colorectal cancer sibling? Am J Gastroenterol. 2005;100(3):703–10.
Hester CA, Dogeas E, Augustine MM, Mansour JC, Polanco PM, Porembka MR, Wang SC, Zeh HJ, Yopp AC. Incidence and comparative outcomes of periampullary cancer: a population-based analysis demonstrating improved outcomes and increased use of adjuvant therapy from 2004 to 2012. J Surg Oncol. 2019;119(3):303–17.
Sánchez-Velázquez P, Muller X, Malleo G, Park JS, Hwang HK, Napoli N, et al. Benchmarks in pancreatic surgery: a novel tool for unbiased outcome comparisons. Ann Surg. 2019;270(2):211–8.
Mackay TM, Gleeson EM, Wellner UF, Williamsson C, Busch OR, Groot Koerkamp B, et al. Transatlantic registries of pancreatic surgery in the United States of America, Germany, the Netherlands, and Sweden: comparing design, variables, patients, treatment strategies, and outcomes. Surgery. 2021;169(2):396–402.
de Wilde RF, Besselink MG, van der Tweel I, de Hingh IH, van Eijck CH, Dejong CH, et al. Impact of nationwide centralization of pancreaticoduodenectomy on hospital mortality. Br J Surg. 2012;99(3):404–10.
Pedrazzoli S. Pancreatoduodenectomy (PD) and postoperative pancreatic fistula (POPF) A systematic review and analysis of the POPF-related mortality rate in 60,739 patients retrieved from the English literature published between 1990 and 2015. Medicine. 2017;96(19):66.
Pessaux P, Sauvanet A, Mariette C, Paye F, Muscari F, Cunha AS, Sastre B, Arnaud JP, Federation de Recherche en C. External pancreatic duct stent decreases pancreatic fistula rate after pancreaticoduodenectomy: prospective multicenter randomized trial. Ann Surg. 2011;253(5):879–85.
House MG, Fong Y, Arnaoutakis DJ, Sharma R, Winston CB, Protic M, et al. Preoperative predictors for complications after pancreaticoduodenectomy: impact of BMI and body fat distribution. J Gastrointest Surg. 2008;12(2):270–8.
Lermite E, Wu T, Sauvanet A, Mariette C, Paye F, Muscari F, et al. Postoperative biological and clinical outcomes following uncomplicated pancreaticoduodenectomy. Korean J Hepatobiliary Pancreat Surg. 2016;20(1):23–31.
van Rijssen LB, Zwart MJ, van Dieren S, de Rooij T, Bonsing BA, Bosscha K, et al. Variation in hospital mortality after pancreatoduodenectomy is related to failure to rescue rather than major complications: a nationwide audit. HPB. 2018;20(8):759–67.
Bourgouin S, Ewald J, Mancini J, Moutardier V, Delpero JR, Le Treut YP. Predictive factors of severe complications for ampullary, bile duct and duodenal cancers following pancreaticoduodenectomy: Multivariate analysis of a 10-year multicentre retrospective series. Surgeon. 2017;15(5):251–8.
Jung JH, Choi DW, Yoon S, Yoon SJ, Han IW, Heo JS, Shin SH. Three thousand consecutive pancreaticoduodenectomies in a tertiary cancer center: a retrospective observational study. J Clin Med. 2020;9(8):66.
Wang W, Liu Q, Zhao ZM, Tan XL, Wang ZZ, Zhang KD, Liu R. Comparison of robotic and open pancreaticoduodenectomy for primary nonampullary duodenal adenocarcinoma: a retrospective cohort study. Langenbecks Arch Surg. 2022;407(1):167–73.
van Rijssen LB, Koerkamp BG, Zwart MJ, Bonsing BA, Bosscha K, van Dam RM, et al. Nationwide prospective audit of pancreatic surgery: design, accuracy, and outcomes of the Dutch Pancreatic Cancer Audit. HPB. 2017;19(10):919–26.
Koch M, Garden OJ, Padbury R, Rahbari NN, Adam R, Capussotti L, et al. Bile leakage after hepatobiliary and pancreatic surgery: a definition and grading of severity by the International Study Group of Liver Surgery. Surgery. 2011;149(5):680–8.
Bassi C, Marchegiani G, Dervenis C, Sarr M, Abu Hilal M, Adham M, et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery. 2017;161(3):584–91.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13.
Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, et al. Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery. 2007;142(1):20–5.
Bakaeen FG, Murr MM, Sarr MG, Thompson GB, Farnell MB, Nagorney DM, et al. What prognostic factors are important in duodenal adenocarcinoma? Arch Surg. 2000;135(6):635–41; discussion 641-632.
He J, Ahuja N, Makary MA, Cameron JL, Eckhauser FE, Choti MA, et al. 2564 resected periampullary adenocarcinomas at a single institution: trends over three decades. HPB. 2014;16(1):83–90.
Lee CHA, Shingler G, Mowbray NG, Al-Sarireh B, Evans P, Smith M, et al. Surgical outcomes for duodenal adenoma and adenocarcinoma: a multicentre study in Australia and the United Kingdom. ANZ J Surg. 2018;88(3):E157-e161.
Lee SY, Lee JH, Hwang DW, Kim SC, Park KM, Lee YJ. Long-term outcomes in patients with duodenal adenocarcinoma. ANZ J Surg. 2014;84(12):970–5.
Shamali A, McCrudden R, Bhandari P, Shek F, Barnett E, Bateman A, Abu Hilal M. Pancreaticoduodenectomy for nonampullary duodenal lesions: indications and results. Eur J Gastroenterol Hepatol. 2016;28(12):1388–93.
Wiltberger G, Krenzien F, Atanasov G, Hau HM, Schmelzle M, Bartels M, Benzing C. Pancreaticoduodenectomy for periampullary cancer: does the tumour entity influence perioperative morbidity and long-term outcome? Acta Chir Belg. 2018;118(6):341–7.
Mungroop TH, Klompmaker S, Wellner UF, Steyerberg EW, Coratti A, D’Hondt M, et al. Updated Alternative Fistula Risk Score (ua-FRS) to include minimally invasive pancreatoduodenectomy: Pan-European validation. Ann Surg. 2021;273(2):334–40.
Mungroop TH, van Rijssen LB, van Klaveren D, Smits FJ, van Woerden V, Linnemann RJ, et al. Alternative Fistula Risk Score for Pancreatoduodenectomy (a-FRS): design and international external validation. Ann Surg. 2019;269(5):937–43.
Chen JS, Liu G, Li TR, Chen JY, Xu QM, Guo YZ, Li M, Yang L. Pancreatic fistula after pancreaticoduodenectomy: risk factors and preventive strategies. J Cancer Res Ther. 2019;15(4):857–63.
Sarr MG. The potent somatostatin analogue vapreotide does not decrease pancreas-specific complications after elective pancreatectomy: a prospective, multicenter, double-blinded, randomized, placebo-controlled trial. J Am Coll Surg. 2003;196(4): 556–64; discussion 564-555; author reply 565.
van Dongen JC, Wismans LV, Suurmeijer JA, Besselink MG, de Wilde RF, Groot Koerkamp B, van Eijck CHJ. The effect of preoperative chemotherapy and chemoradiotherapy on pancreatic fistula and other surgical complications after pancreatic resection: a systematic review and meta-analysis of comparative studies. HPB. 2021;23(9):1321–31.
Hamza N, Darwish A, O’Reilly DA, Denton J, Sheen AJ, Chang D, et al. Perioperative enteral immunonutrition modulates systemic and mucosal immunity and the inflammatory response in patients with periampullary cancer scheduled for pancreaticoduodenectomy: a randomized clinical trial. Pancreas. 2015;44(1):41–52.
van Dijk DPJ, van Woerden V, Cakir H, den Dulk M, Olde Damink SWM, Dejong CHC. ERAS: improving outcome in the cachectic HPB patient. J Surg Oncol. 2017;116(5):617–22.
Fearon KC, Barber MD, Falconer JS, McMillan DC, Ross JA, Preston T. Pancreatic cancer as a model: inflammatory mediators, acute-phase response, and cancer cachexia. World J Surg. 1999;23(6):584–8.
Gupta R, Ihmaidat H. Nutritional effects of oesophageal, gastric and pancreatic carcinoma. Eur J Surg Oncol. 2003;29(8):634–43.
Smits FJ, Henry AC, van Eijck CH, Besselink MG, Busch OR, Arntz M, et al. Care after pancreatic resection according to an algorithm for early detection and minimally invasive management of pancreatic fistula versus current practice (PORSCH-trial): design and rationale of a nationwide stepped-wedge cluster-randomized trial. Trials. 2020;21(1):389.
van Wijk L, van der Snee L, Buis CI, Hentzen J, Haveman ME, Klaase JM. A prospective cohort study evaluating screening and assessment of six modifiable risk factors in HPB cancer patients and compliance to recommended prehabilitation interventions. Perioper Med. 2021;10(1):5.
Li T, D’Cruz RT, Lim SY, Shelat VG. Somatostatin analogues and the risk of post-operative pancreatic fistulas after pancreatic resection: asystematic review & meta-analysis. Pancreatology. 2020;20(2):158–68.
Acknowledgement
This study was not preregistered. Deltaplan Alvleesklierkanker supports the DPCG.
Funding
This work was funded by Deltaplan Alvleesklierkanker, Dutch Institute for Clinical Auditing, who were not involved in the study design or drafting of the manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
JdB, JAS, JT, MB, and GK were involved in the conception and design of the study, acquisition of data, analysis and interpretation of the data, drafting and revising critically all versions of the article for important intellectual content, and gave final approval of this current version to be published. BB, OB, CvE, IdH, VdM, IQM, HvS, MS, SF, EvdH, GP, DL, MD and KB were involved in the conception and design of the study, interpretation of the data, revising critically all versions of the article for important intellectual content, and gave final approval of this current version to be published.
Corresponding authors
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Jacob K. de Bakker and J. Annelie Suurmeijer shared first authorship on this work.
Marc G. Besselink and Geert Kazemier shared senior authorship on this work.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
de Bakker, J.K., Suurmeijer, J.A., Toennaer, J.G.J. et al. Surgical Outcome After Pancreatoduodenectomy for Duodenal Adenocarcinoma Compared with Other Periampullary Cancers: A Nationwide Audit Study. Ann Surg Oncol 30, 2448–2455 (2023). https://doi.org/10.1245/s10434-022-12701-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-022-12701-y