
Abstract
Background
Anaplastic thyroid carcinoma (ATC) is a rare and lethal form of thyroid cancer. Overall prognosis is unclear when it arises focally in a background of papillary thyroid cancer (PTC). Clinicopathologic features and outcomes of tumors with coexisting PTC and ATC histologies (co-PTC/ATC) were categorized.
Methods
The National Cancer Database was queried for histologic codes denoting PTC, ATC, and co-PTC/ATC, defined as Grade 4 PTC, diagnosed from 2004 to 2017. Clinicopathologic features, OS, and treatment outcomes were analyzed by histologic type.
Results
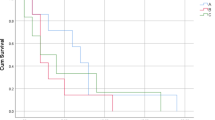
A total of 386,862 PTC, 763 co-PTC/ATC, and 3,880 ATC patients were identified. Patients with co-PTC/ATC had clinicopathologic features in-between those of PTC and ATC, including rates of tumor size >4 cm, extrathyroidal extension, and distant metastases. On multivariable Cox proportional hazards modeling, age >55 years, Charlson-Deyo score ≥2, positive lymph nodes, lymphovascular invasion, distant metastases, and positive surgical margins were associated with worse OS, whereas radioactive iodine (RAI) and external beam radiation therapy (EBRT) were associated with improved OS, irrespective of margin status. OS was worse for co-PTC/ATC than for PTC but better than for ATC and differed based on the presence or absence of “aggressive” tumor features, including lymph node positivity, lymphovascular invasion, distant metastases, and positive surgical margins.
Conclusions
Survival of patients with co-PTC/ATC is dependent on the presence of aggressive clinicopathologic features and lies within a spectrum between that of PTC and ATC. Adjuvant RAI and EBRT treatment may be beneficial, even after R0 resection.




Similar content being viewed by others

References
Pezzi TA, Mohamed AS, Fuller CD, et al. Radiation therapy is independently associated with worse survival after r0-resection for stage I-II non-small cell lung cancer: an analysis of the National Cancer Data Base. Ann Surg Oncol. 2017;24(5):1419–27.
Cramer JD, Fu P, Harth KC, Margevicius S, Wilhelm SM. Analysis of the rising incidence of thyroid cancer using the Surveillance Epidemiology and End Results National Cancer Data Registry. Surgery. 2010;148(6):1147–53.
Bible KC, Kebebew E, Brierley J, et al. 2021 American Thyroid Association Guidelines for management of patients with anaplastic thyroid cancer. Thyroid. 2021;31(3):337–86.
Molinaro E, Romei C, Biagini A, et al. Anaplastic thyroid carcinoma: from clinicopathology to genetics and advanced therapies. Nat Rev Endocrinol. 2017;13(11):644–60.
Haymart MR, Banerjee M, Yin H, Worden F, Griggs JJ. Marginal treatment benefit in anaplastic thyroid cancer. Cancer. 2013;119(17):3133–9.
Glaser SM, Mandish SF, Gill BS, Balasubramani GK, Clump DA, Beriwal S. Anaplastic thyroid cancer: prognostic factors, patterns of care, and overall survival. Head Neck. 2016;38(Suppl 1):E2083–90.
Oishi N, Kondo T, Ebina A, et al. Molecular alterations of coexisting thyroid papillary carcinoma and anaplastic carcinoma: identification of TERT mutation as an independent risk factor for transformation. Mod Pathol. 2017;30(11):1527–37.
Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133.
Choi JY, Hwang BH, Jung KC, et al. Clinical significance of microscopic anaplastic focus in papillary thyroid carcinoma. Surgery. 2013;154(1):106–10.
Ragazzi M, Torricelli F, Donati B, et al. Coexisting well-differentiated and anaplastic thyroid carcinoma in the same primary resection specimen: immunophenotypic and genetic comparison of the two components in a consecutive series of 13 cases and a review of the literature. Virchows Arch. 2021;478(2):265–81.
Wong KS, Lorch JH, Alexander EK, et al. Histopathologic features and clinical outcome of anaplastic thyroid carcinoma with a minor anaplastic component. Endocr Pathol. 2020;31(3):283–90.
Lerro CC, Robbins AS, Phillips JL, Stewart AK. Comparison of cases captured in the national cancer data base with those in population-based central cancer registries. Ann Surg Oncol. 2013;20(6):1759–65.
Limberg J, Stefanova D, Thiesmeyer JW, et al. Association of medicaid expansion of the Affordable Care Act with the stage at diagnosis and treatment of papillary thyroid cancer: a difference-in-differences analysis. Am J Surg. 2021;222(3):562–9.
Kwon J, Kim BH, Jung HW, Besic N, Sugitani I, Wu HG. The prognostic impacts of postoperative radiotherapy in the patients with resected anaplastic thyroid carcinoma: a systematic review and meta-analysis. Eur J Cancer. 2016;59:34–45.
Khan ZF, Kutlu O, Picado O, Lew JI. Margin positivity and survival outcomes: a review of 14,471 patients with 1-cm to 4-cm papillary thyroid carcinoma. J Am Coll Surg. 2021;232(4):545–50.
Mercado CE, Drew PA, Morris CG, Dziegielewski PT, Mendenhall WM, Amdur RJ. Positive surgical margins in favorable-stage differentiated thyroid cancer. Am J Clin Oncol. 2018;41(12):1168–71.
Adam MA, Thomas S, Youngwirth L, et al. Is there a minimum number of thyroidectomies a surgeon should perform to optimize patient outcomes? Ann Surg. 2017;265(2):402–7.
Acknowledgments
The authors thank Paul Christos, PhD, for his review of the statistical analyses herein.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
The authors report no relevant conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Greenberg, J.A., Moore, M.D., Thiesmeyer, J.W. et al. Coexisting Papillary and Anaplastic Thyroid Cancer: Elucidating the Spectrum of Aggressive Behavior. Ann Surg Oncol 30, 137–145 (2023). https://doi.org/10.1245/s10434-022-12553-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-022-12553-6