
Abstract
Background
The Society of Surgical Oncology collaborates with the National Resident Matching Program (NRMP) to facilitate the Complex General Surgical Oncology (CGSO) Match.
Objective
The purpose of this study was to understand trends in CGSO Match outcomes. We hypothesized that (1) match rates would increase with time; (2) US allopathic graduates would have higher match rates than non-US allopathic graduates; and (3) most applicants would match at one of their top three ranked choices.
Methods
The NRMP provided applicant and program data from the CGSO Match (2014–2021). Chi-square tests elucidated temporal trends and match rates by applicant archetype.
Results
The annual number of applicants decreased from 103 to 90 (13% decrease), while the annual number of fellowship positions increased from 56 to 67 (20% increase) from 2014–2021. The annual percentage of applicants who did not match decreased from 46% to 26% (p < 0.05). Annual match rates increased from 54% to 74% (p < 0.05). US allopathic graduates had higher match rates than non-US allopathic graduates but this disparity narrowed over time (84% vs. 55% in 2021; p < 0.001). Approximately half of all applicants matched at one of their top three choices (first, 29%; second, 12%; third, 8%). Applicants matching at one of their top three choices increased from 36% to 50% (p < 0.05).
Conclusions
CGSO Match rates have increased over the past decade, thus primarily benefiting non-US allopathic graduates. Most applicants match at one of their top three choices. More research is needed to understand disparities in match rates by applicant and residency program characteristics.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The Society of Surgical Oncology (SSO) sponsors the Complex General Surgical Oncology (CGSO) Match, which helps coordinate the placement of general surgery residents into CGSO Fellowships. Fellowship programs in the US are accredited by the Accreditation Council for Graduate Medical Education (ACGME) and adhere to specific requirements as outlined in the ACGME Program Requirements for Graduate Medical Education in CGSO.1During the 2022 CGSO Match, there were also five Canadian programs that were accredited by the Royal College of Physicians and Surgeons of Canada. Programs participating in the CGSO Match must be approved by the SSO and adhere to the CGSO curriculum.2.
Fellowship applicants in general surgery residency training typically apply during their penultimate year of training. Interviews are conducted February through May of the CGSO Match year and results are announced in the middle of June.3 CGSO Fellowship training commences on 1 August of the subsequent year after general surgery residents complete their residency training.
Data on the relative performance of US versus non-US allopathic graduates can help prospective applicants anticipate outcomes from the CGSO Match. The CGSO Match is a competitive process with a 65% match rate from 2009 to 2018.4 Prior to the universal adoption of the virtual interview process after coronavirus disease 2019 (COVID-19), the fellowship application process was a costly endeavor that required significant financial and time investments. While no studies on the cost of fellowship application exist specifically for CGSO, the average general surgery fellowship applicant invests over $4000 to attend, on average, 8–12 interviews.5 The permanency of the virtual interview process for CGSO Fellowship interviews remains uncertain.
This study elucidates contemporary outcomes in the CGSO Match, including the number of applicants, programs, available positions, match rates, and number of unmatched positions. We further determine the number of applicants matching at their top-ranked fellowships. We hypothesized that match rates would increase over the study period, with the majority of applicants matching at their top-three ranked fellowships. We further hypothesized that US allopathic graduates would have higher match rates than non-US allopathic graduates. Ultimately, we provide objective data to help inform future applicants and faculty during the match process.
Methods
The National Resident Matching Program (NRMP) provided outcomes data from the CGSO Match. Given the public availability of all data, this study received review exemption from the Institutional Review Board. Eligible training programs were either accredited by the ACGME or the Royal College of Physicians and Surgeons of Canada. All training programs adhered to specific curriculum requirements to receive SSO recognition status.2 The NRMP provided data on the number of applicants, number of available positions, and unfilled positions by specialty.
This was a retrospective cohort study of all applicants from 2014 to 2021. Match rates for US and non-US allopathic graduates were calculated and trended over time. Percentages of applicants matching at their first, second, third, and fourth or higher ranked fellowship were calculated and trended over time. The annual percentage of unmatched positions was calculated and trended over time.
Temporal trends were analyzed using Chi-square goodness-of-fit tests. Differences in match rates by applicant archetype (US and non-US allopathic graduates) were calculated using Chi-square tests. All statistical tests were two-tailed and were calculated on GraphPad Prism (San Diego, CA, USA). P-values <0.05 were considered statistically significant.
Results
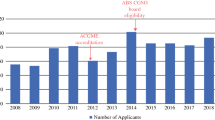
From 2014 to 2021, the number of fellowship programs increased from 23 to 34 (48% increase) and the number of available positions increased from 56 to 67 (20% increase). The annual number of applicants decreased from 103 in 2014 to 90 in 2021 (13% decrease). The increase in applicants was driven primarily by US allopathic graduates, which increased from 52 in 2014 to 61 in 2021 (17% increase). The annual number of non-US allopathic graduates decreased from 51 in 2014 to 29 in 2021 (43% decrease). The annual percentage of applicants that did not match decreased from 46% in 2014 to 26% in 2021 (p < 0.05) (Fig. 1).

Number of applicants and programs in the Complex General Surgical Oncology (CGSO) Match
From 2014 to 2021, the annual match rate increased from 54% to 74% (p < 0.05). The average match rate over the past three application cycles (2019–2021) was 75%. Both US and non-US allopathic graduates had significant increases in annual match rates over the study period (Fig. 2). The increase in overall match rates was driven primarily by the increase in match rates for non-US allopathic graduates. During each year, US allopathic graduates had higher match rates than non-US allopathic graduates (p < 0.05), but this disparity decreased over the study period. In 2014, there was a 1.9-fold difference in match rates between US and non-US allopathic graduates (71% vs. 37%, p < 0.001), which decreased to 1.5-fold in 2021 (84% vs. 54%; p < 0.001).

Match rates in the Complex General Surgical Oncology (CGSO) Match
Over the study period, about half of all applicants matched at one of their top three choices (Fig. 3): first choice, 29%; second choice, 12%; third choice, 8%. The percentage of applicants who matched at their fourth choice or lower was 19%, while the percentage of unmatched applicants was 32%. Applicants matching at one of their top three choices increased from 36% to 50% (p < 0.001) over the study period.

Proportion of applicants matching at their top choices in the Complex General Surgical Oncology (CGSO) Match
There were only two unmatched positions in the CGSO Match over the study period, with one occurring in 2015 and another in 2018 (Table 1).
Discussion
Contemporary trends in the CGSO Match highlight increasing match rates, especially benefitting non-US allopathic graduates. Similarly, the rate of unmatched applicants has decreased and the proportion of applicants matching at one of their top three choices has increased. The exact reasons for this are unclear and should be the focus of future research. Overall, the annual number of training positions has increased, while the annual number of applicants has decreased, especially among non-US allopathic graduates. Increasing match rates are fundamentally driven by an increasing number of available training positions and fewer applicants. Even so, the CGSO Match remains a competitive process, with a 74% overall match rate in 2021 and 55% among non-US allopathic graduates.
A previous study analyzing applications to a single CGSO fellowship program determined positive predictors for successful matriculation. These were achieving Alpha Omega Alpha status, obtaining a dual degree, and performing a clinical or research rotation at a desired program.6 Similarly, an analysis of all applicants to CGSO fellowship programs in 2015–2016 revealed additional factors associated with successful matriculation, which included medical school tier, residency reputation, and individual research accomplishments.7 However, additional factors such as interview performance, quality of letters of recommendation, and American Board of Surgery In-Training Examination (ABSITE) performance were not analyzed. Indeed, a survey of CGSO fellowship program directors revealed the importance of ABSITE scores, number of first author publications, interview performance, operative skills, and interpersonal skills (e.g., ability to work as part of a team and communication abilities) on ranking applicants in the CGSO Match.8
The first qualifying examination for CGSO as a board-certified specialty was administered on 15 September 2014,9 which coincided with the start of our study period. Overall, CGSO fellows believe completion of ACGME-accredited fellowship training is important to obtaining academic career goals in surgical oncology. Indeed, models in surgical oncology training are rapidly evolving, with these trends driving the competitiveness of CGSO fellowship training.10,11,12 In our study, the competitiveness of matching at CGSO fellowship training appeared to decrease over the study period, which was driven by the increasing number of available training positions and a decreasing number of applications. This is a potentially disturbing trend given the predicted future shortage of the oncology workforce.13,14 The etiology of the decreasing number of applicants is likely multifactorial and driven by financial and future job prospects. Most CGSO fellowship graduates are employed at major academic medical centers,15 which may present a barrier to the desired practice settings of many general surgery residents. Ultimately, more research is needed to improve the adequacy of the CGSO workforce, including the distribution of these providers in the US.
Prospective applicants can use these data to anticipate CGSO Match outcomes and plan accordingly. About half of all applicants over the study period matched at one of their top three ranked programs. Results from this study highlight that non-US allopathic graduates should apply to more programs than US allopathic graduates, given the lower match rates. COVID-19 has greatly impacted the CGSO Match, as all interviews have been conducted virtually for the 2021 and 2022 application cycles.16,17,18 Prior to the pandemic, in-person interviews required significant time and financial resources. Most applicants spent $4000 to attend between 8–12 interviews.5 While the present study was not designed to assess the impact of virtual interviews on CGSO Match rates, we believe this is an important area of future research. Virtual interviews and coordinated interviews at well-attended national meetings such as the SSO can help alleviate financial and logistical burdens of future application cycles.
Several limitations existed in this study. First, only 8 years of Match data were analyzed to provide a contemporary analysis. Second, given the limitations of NRMP data, the impact of additional applicant variables on match outcomes could not be assessed. Future studies should assess the role of race and sex on Match outcomes, given recent efforts to promote diversity and inclusion in surgical oncology.19,20 Surveys and focus group discussions can provide additional insights into how to improve the efficiency of the CGSO Match. Third, the impact of other training variables such as publication output, residency program reputation, and letters of recommendation on Match outcomes were not available and will be the focus of subsequent research.
Conclusion
In summary, match rates in the CGSO Match have increased over the past 8 years and about half of applicants match at one of their top three choices. This study provides a benchmark for future applicants and mentors to anticipate Match outcomes and ultimately improve the efficiency of the CGSO Match. More research is needed to understand disparities in match rates by additional applicant and training factors.
References
Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Graduate Medical Education in Complex General Surgical Oncology. Available at: https://www.acgme.org/globalassets/PFAssets/ProgramResources/446_ComplexGeneralSurgicalOncology_2020_TCC.pdf?ver=2020-02-17-090323-063&ver=2020-02-17-090323-063. Accessed 1 Mar 2022.
Society of Surgical Oncology. Surgical Oncology Fellowship Patient Care and Medical Knowledge Curriculum Outline. Available at: https://www.surgonc.org/wp-content/uploads/2019/03/surgical-oncology-curriculum-outline-extended-version.pdf. Accessed 1 Mar 2022.
Society of Surgical Oncology. Complex General Surgical Oncology (CGSO) Fellowships. Available at: https://www.surgonc.org/fellows/surgical-oncology-fellowships/. Accessed 1 Mar 2022.
Yheulon CG, Cole WC, Ernat JJ, Davis SS Jr. Normalized competitive index: analyzing trends in surgical fellowship training over the past decade (2009–2018). J Surg Educ. 2020;77(1):74–81.
Watson SL, Hollis RH, Oladeji L, Xu S, Porterfield JR, Ponce BA. The burden of the fellowship interview process on general surgery residents and programs. J Surg Educ. 2017;74(1):167–72.
Lillemoe HA, Scally CP, Adams CL, Bednarski BK, Balch CM, Aloia TA, et al. Complex general surgical oncology fellowship applicants: trends over time and the impact of board certification eligibility. Ann Surg Oncol. 2019;26(9):2667–74.
Wach MM, Ruff SM, Ayabe RI, Martin SP, Diggs LP, Alexander IA, et al. An examination of applicants and factors associated with matriculation to complex general surgical oncology fellowship training programs. Ann Surg Oncol. 2018;25(12):3436–42.
Wach MM, Ayabe RI, Ruff SM, D’Angelica M, Dineen SP, Grubbs EG, et al. A survey of the complex general surgical oncology fellowship programs regarding applicant selection and rank. Ann Surg Oncol. 2019;26(9):2675–81.
Lee DY, Flaherty DC, Lau BJ, Deutsch GB, Kirchoff DD, Huynh KT, et al. Attitudes and perceptions of surgical oncology fellows on ACGME accreditation and the complex general surgical oncology certification. Ann Surg Oncol. 2015;22(12):3776–84.
Jeyarajah DR, Abouljoud M, Alseidi A, Berman R, D’Angelica M, Hagopian E, et al. Training paradigms in hepato-pancreatico-biliary surgery: an overview of the different fellowship pathways. J Gastrointest Surg. 2021;25(8):2119–28.
Qadan M, Davies AR, Polk HC, Allum WH, Brennan MF. Cancer care in the developed world: a comparison of surgical oncology training programs. Am J Surg. 2018;215(1):1–7.
Kim MJ, Monson JR. The future of innovation and training in surgical oncology. Surg Oncol. 2011;20(3):219–22.
Erikson C, Salsberg E, Forte G, Bruinooge S, Goldstein M. Future supply and demand for oncologists: challenges to assuring access to oncology services. J Oncol Pract. 2007;3(2):79–86.
Yang W, Williams JH, Hogan PF, Bruinooge SS, Rodriguez GI, Kosty MP, et al. Projected supply of and demand for oncologists and radiation oncologists through 2025: an aging, better-insured population will result in shortage. J Oncol Pract. 2014;10(1):39–45.
Ruff S, Ilyas S, Steinberg SM, Tatalovich Z, McLaughlin SA, D’Angelica M, et al. Survey of surgical oncology fellowship graduates 2005–2016: insight into initial practice. Ann Surg Oncol. 2019;26(6):1622–8.
Vining CC, Eng OS, Hogg ME, Schuitevoerder D, Silverman RS, Yao KA, et al. Virtual surgical fellowship recruitment during COVID-19 and its implications for resident/fellow recruitment in the future. Ann Surg Oncol. 2020;27(3):911–5.
Molina G, Mehtsun WT, Qadan M, Hause KC, Raut CP, Fairweather M. Virtual interviews for the complex general surgical oncology fellowship: the dana-farber/partners experience. Ann Surg Oncol. 2020;27(9):3103–6.
Hill MV, Ross EA, Crawford D, Lai L, Turaga K, Grubbs EG, et al. Program and candidate experience with virtual interviews for the 2020 Complex General Surgical Oncology interview season during the COVID pandemic. Am J Surg. 2021;222(1):99–103.
Clarke CN. Disparities in creating a diverse surgical oncology physician workforce: Just a leaky pipeline? Surg Oncol Clin. 2022;31(1):21–7.
Chowdhary M, Chowdhary A, Royce TJ, Patel KR, Chhabra AM, Jain S, et al. Women’s representation in leadership positions in academic medical oncology, radiation oncology, and surgical oncology programs. JAMA Netw Open. 2020;3(3):e200708.
Acknowledgement
The authors would like to thank the Howard-Harvard Health Sciences Outcomes Research Center for their statistical support and expertise.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Silvestre, J., Smith, J.R., Nasef, K.E. et al. Application and Match Rates in the Complex General Surgical Oncology Match. Ann Surg Oncol 29, 8094–8098 (2022). https://doi.org/10.1245/s10434-022-12428-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-022-12428-w