
Abstract
Background
Hepatocellular carcinoma (HCC) is a highly aggressive malignant disease with a high rate of vascular invasion. (Bruix et al. in Gastroenterology 150:835–853, 2016; Xia et al. in Oncol Lett 20:101, 2020) The conventional surgical strategy for HCC with inferior vena cava (IVC) tumor thrombus is open major surgery with cardiopulmonary bypass, combined with large trauma. (Liu et al. in Eur J Gastroenterol Hepatol 24:186–194, 2012; Bai et al. in J Oncol 2020:3264079, 2020) We report a video of laparoscopic hemihepatectomy and thrombectomy without bypass. As far as we are aware, this is the first report on IVC thrombectomy using a minimally invasive surgical technique.
Patient
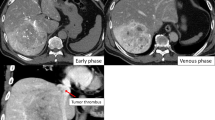
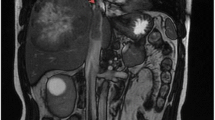
A 52-year-old male was admitted to our institution for a giant hepatic mass in the right liver combined with IVC tumor thrombosis. After 2 months of preoperative systemic treatment, the tumor had reduced to 8 cm and the enhancement of tumor thrombosis in the magnetic resonance imaging (MRI) scan was significantly reduced.
Methods
We used laparoscopy combined with thoracoscopy to perform the surgery, with the patient placed in the supine position. The abdominal trocar position is shown in Fig. 1b. First, we set the blocking band of the suprahepatic IVC in the thoracoscopy. Infrahepatic IVC occlusion and the Pringle maneuver device were prepared for laparoscopy. After fully exposing the retrohepatic IVC, we performed a thrombectomy and IVC suture completely in laparoscopy. Finally, the patient was transferred to the intensive care unit (ICU) for observation.

a Three-dimensional reconstruction model of the patient (a giant hepatic mass and tumor thrombosis extending to the suprahepatic IVC). b Trocar position for the laparoscopic surgery. The patient was placed in the supine position, and the 5, 6, and 7 intercostal axillary fronts were set for the thoracoscopic trocar, while the remaining five abdominal trocars were set for laparoscopic operation. c Retrohepatic IVC before being cut open. The fullness indicates the position of the tumor thrombosis. d Thrombectomy and suture of the IVC. IVC inferior vena cava, TT tumor thrombus
Results
Operation time was 495 mins and estimated blood loss was 1000 mL. The patient was discharged on the thirteenth day after the surgery. HCC was confirmed in histopathology.
Conclusion
Laparoscopic hepatectomy with IVC thrombectomy is a possible operation for HCC combined with IVC tumor thrombus, offering hope for minimally invasive treatment of such cases; however, it is still a highly challenging procedure.
Similar content being viewed by others

References
Bruix J, Reig M, Sherman M. Evidence-based diagnosis, staging, and treatment of patients with hepatocellular carcinoma. Gastroenterology. 2016;150:835–53.
Xia Y, Zhang J, Ni X. Diagnosis, treatment and prognosis of hepatocellular carcinoma with inferior vena cava/right atrium tumor thrombus. Oncol Lett. 2020;20:101.
Liu J, Wang Y, Zhang D, et al. Comparison of survival and quality of life of hepatectomy and thrombectomy using total hepatic vascular exclusion and chemotherapy alone in patients with hepatocellular carcinoma and tumor thrombi in the inferior vena cava and hepatic vein. Eur J Gastroenterol Hepatol. 2012;24:186–94.
Bai Y, Wu J, Zeng Y, et al. Nomogram for predicting long-term survival after synchronous resection for hepatocellular carcinoma and inferior vena cava tumor thrombosis: a multicenter retrospective study. J Oncol. 2020;2020:3264079.
Funding
This study was supported by the Zhejiang Major Medical Science and Technology Plan supported by the National Health Commission of China under Grant No. WKJ-ZJ-2030 (to XL), the National Natural Science Foundation of China under Grant No. 82072625 (to XL), the National Natural Science Foundation of China under Grant No. 81827804 (to XL), Key Research and Development Project of Zhejiang Province under Grant No. 2021C03127 (to XL), and the Medical Health Science and Technology Project of Zhejiang Province under Grant No. 2018PY029 (to JC).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
Jiaqi Gao, Junhao Zheng, Ziyi Zhu, Junjie Xu, Weilin Qi, Jun Chen, and Xiao Liang have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (M4V 92711 kb)
Rights and permissions
About this article

Cite this article
Gao, J., Zheng, J., Zhu, Z. et al. Laparoscopic Orthotopic Right Hemihepatectomy by Anterior Approach Combined with Inferior Vena Cava Thrombectomy. Ann Surg Oncol 29, 5548–5549 (2022). https://doi.org/10.1245/s10434-022-11710-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-022-11710-1