
Abstract
It is unknown whether the survival of patients cured of esophageal cancer differs from that of the corresponding background population. This nationwide and population-based cohort study included all patients who survived for at least 5 years after surgery for esophageal cancer in Sweden between 1987 and 2015, with follow-up throughout 2020. Relative survival rates with 95% confidence intervals (95% CI) were calculated by dividing the observed with the expected survival. The expected survival was assessed from the entire Swedish population of the corresponding age, sex, and calendar year. Yearly relative survival rates were calculated between 6 and 10 years postoperatively. Among all 762 participants, the relative survival was initially similar to the background population (96.1%, 95% CI 94.3–97.9%), but decreased each following postoperative year to 83.5% (95% CI 79.5–87.6%) by year 10. The drop in relative survival between 6 and 10 years was more pronounced in participants with a history of squamous cell carcinoma [from 94.5% (95% CI 91.2–97.8%) to 70.8% (95% CI 64.0–77.6%)] than in those with adenocarcinoma [from 96.9% (95% CI 94.8–99.0%) to 91.5% (95% CI 86.6–96.3%)], and in men [from 96.0% (95% CI 93.8–98.1%) to 81.8% (95% CI 76.8–86.8%)] than in women [from 96.4% (95% CI 93.4–99.5%) to 88.1% (95% CI 81.5–94.8%)]. No major differences were found between age groups. In conclusion, esophageal cancer survivors had a decline in survival between 6 and 10 years after surgery compared with the corresponding general population, particularly those with a history of squamous cell carcinoma of the esophagus and male sex.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Esophageal cancer is the eighth most common cancer worldwide, with approximately 600,000 new cases every year,1,2 and has a poor prognosis with overall 5-year survival below 20%.2 The dominating histological types are adenocarcinoma, which is mainly associated with gastroesophageal reflux disease and obesity, and squamous cell carcinoma, with heavy alcohol consumption and tobacco smoking as the main risk factors.2,3,4 Curatively intended treatment usually includes surgical resection (esophagectomy) with or without pre- or perioperative chemo(radio)therapy and is followed by a 5-year survival of 30–45%, with tumor stage as the strongest prognostic factor.2,6,7 Esophagectomy is one of the most extensive standard surgical procedures, and comorbidity and fitness are carefully assessed preoperatively. Tumor recurrences and deaths in esophageal cancer typically occur shortly after treatment (within 1–3 years), and 5-year survivors can be considered cured.1 Whether life expectancy among esophageal cancer survivors differs from the corresponding background population is unknown. Yet this knowledge is of great relevance to individuals and families, and also to healthcare and society. Esophageal cancer survivors might have a worse survival; the risk factors for the tumor could increase the risk of other lethal diseases or conditions, the treatment itself can cause serious sequelae,7,8 and the prevalence of severe comorbidities could be increased.7,9,10 The survival may also be better, e.g., due to selection of the fittest patients for curative treatment, healthy lifestyle changes, and increased awareness of symptoms of serious illnesses that may alert individuals to seek medical attention in time. This study aimed to clarify whether and how the survival of patients cured of esophageal cancer differs from that of the corresponding general population.
Patients and Methods
Design
This was a population-based cohort study that included all individuals in Sweden who survived for at least 5 years after surgery for esophageal cancer within the study period from 1 January 1987 to 31 December 2020. The observed survival from 6 to 10 years after esophagectomy in this cohort was compared with the expected survival, which was estimated from the survival in the entire Swedish population of the corresponding age, sex, and calendar year. We did not assess longer follow-up after considering the statistical power. The dominating surgical procedure was open thoracoabdominal surgery according to Ivor Lewis. A patient research partnership group consisting of former esophageal cancer patients was involved in formulating the research question and in the planning of the study. The study was approved by the Regional Ethical Review Board in Stockholm, Sweden.
Data Sources
Study Cohort
The cohort of esophageal cancer survivors was retrieved from the Swedish Esophageal Cancer Surgery Study (SESS). Earlier versions of this cohort have been used for studies examining factors influencing the survival after esophageal cancer surgery.11,12,13 Data came from medical records and national Swedish health data registries, including the Cancer Registry, Patient Registry, and Cause of Death Registry. The Cancer Registry is 98% complete for esophageal cancer;14 the Patient Registry has a positive predictive value of 99.6% for esophageal cancer surgery;15 the recording of death dates is 100% in the Cause of Death Registry.16
Background Population
Statistics Sweden provided survival data of the entire Swedish population by age, sex, and calendar year. Statistics Sweden also records the death dates of all Swedish residents, and this information is automatically issued to the Cause of Death Registry.17 The completeness of the recording of residents and deaths (including deaths abroad) is 100%.16 Ethnicity data was not available for the cohort nor the background population.
Statistical Analysis
The follow-up of the esophageal cancer survivors started in year 6 after esophagectomy and ended after year 10. Relative survival rates with 95% confidence intervals (CI) were calculated for each of the five follow-up years by dividing the observed survival with the expected survival using the life table method.18 The expected survival was derived from the entire Swedish population of the same age, sex, and calendar year. Stratified analyses were performed by sex (male and female), age (in quartiles, i.e., four approximately equal-sized groups), calendar period (quartiles), tumor histology (adenocarcinoma and squamous cell carcinoma), and comorbidity (Charlson comorbidity index 0, 1, and ≥ 2). Calendar year and age groups were divided into quartiles to avoid arbitrary cut-offs as decided before initiating the analyses. A sub-analysis was performed in which we excluded patients with diagnoses related to heavy smoking tobacco and alcohol abuse, in both patients with a history of adenocarcinoma and those with squamous cell carcinoma. The analyses followed a predefined study protocol and were conducted by an experienced biostatistician (F.M.) who used the statistical software SAS, Version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Participants
The study included 762 individuals who survived for at least 5 years after surgery for esophageal cancer. The majority of the participants were men, aged above 70 years, who underwent their surgery after the year 2007, and had tumor histology of adenocarcinoma. The vast majority of the patients had early pathological tumor stage (Table 1).
Survival
Total Cohort
The survival of the total cohort was marginally lower than the background population 6 years after surgery (96.1%, 95% CI 94.3–97.9), but decreased almost linearly each year to 83.5% (95% CI 79.5–87.6) in year 10 (Table 2).
Sexes
The reduction in relative survival during the follow-up decreased more in men [from 96.0% (95% CI 93.8–98.1%) in year 6 to 81.8% (95% CI 76.8-86.8%) in year 10] than in women [from 96.4% (95% CI 93.4–99.5%) in year 6 to 88.1% (95% CI 81.5–94.8%) in year 10] (Table 3).
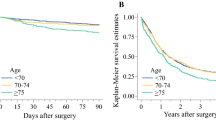
Age Groups
There were no major differences in the decline in relative survival when comparing the different age groups (Table 4).
Calendar Periods
The relative survival showed similar trends, with a reduction between 6 and 10 years after esophagectomy in all calendar periods, but the survival was worse during earlier calendar periods than in more recent periods (Table 5).
Tumor Histology
There was a pronounced drop in relative survival in participants with a history of squamous cell carcinoma, i.e., from 94.5% (95% CI 91.2–97.8%) in year 6 to 70.8% (95% CI 64.0–77.6%) in year 10. Participants with a history of adenocarcinoma indicated only a slightly decreased relative survival during follow-up, with a reduction from 96.9% (95% CI 94.8–99.0%) in year 6 to 91.5% (95% CI 86.6–96.3%) in year 10 (Table 6).
Comorbidity
The relative survival of esophageal cancer survivors was worse in patients with higher Charlson comorbidity scores (Table 7).
Exclusion of Patients with Smoking- and Alcohol-Related Diagnoses
The relative survival remained inferior to the corresponding background population after exclusion of patients with smoking- and alcohol-related diagnoses. There were minor improvements in relative survival in patients with a history of adenocarcinoma and a moderate improvement in those with a history of squamous cell carcinoma (Table 8).
Discussion
This study found that esophageal cancer survivors have poorer survival than the corresponding background population, and the difference increased between 6 and 10 years after surgery. The reduction in relative survival seemed more pronounced in men than in women and in those with comorbidity than without, but was particularly marked among participants with a history of squamous cell carcinoma compared with adenocarcinoma of the esophagus.
This study benefits from a population-based design with the inclusion of all patients treated for esophageal cancer in Sweden who had survived for 5 years. This counteracts selection bias and facilitates generalizability. Another strength was the complete follow-up for survival, which rules out losses to follow-up. The well-maintained population registries in Sweden made it possible to compare the observed survival in the study cohort with that of the entire Swedish population of the corresponding age, sex, and calendar year. Among the limitations is the limited data available in the background population, which made it impossible to perform more targeted analyses and assess diseases that might contribute to the differences in survival. However, this was not the aim of the study. Although patients who have undergone surgery for esophageal cancer and survived for 5 years are considered cured of cancer, some late deaths due to tumor recurrences cannot be ruled out. However, any such deaths would occur earlier rather than later during the follow-up, and do not explain the main finding of a reduction in survival from 6 to 10 years after surgery. Finally, the statistical power did not allow robust analyses of survival more than 10 years after treatment.
This study yielded novel information to an area with gaps in knowledge. Previous studies investigating long-term survival in patients with esophageal cancer have examined survival up to 5 years after treatment, but to our knowledge, no study has compared the survival after 5 years with that of a corresponding general population.19
The results of the stratified analyses provide some clues that may help explain the findings. The most striking result was the substantial decline in relative survival in patients with a history of squamous cell carcinoma compared with those with adenocarcinoma. Heavy alcohol consumption and tobacco smoking, particularly in combination, are strong risk factors for squamous cell carcinoma, and these exposures are associated with several other diseases and generally poorer survival.3,4 This was supported by the finding of better survival in squamous cell carcinoma after exclusion of patients with patients with smoking and- alcohol-related diagnoses. Another factor that may contribute is the generally lower socioeconomic status of this patient category. Regarding adenocarcinoma, the main risk factor of gastro-esophageal reflux disease is not associated with decreased survival,20,21 while the risk factor of obesity reduces the overall survival to a limited degree, which could explain the slightly lower survival than the background population in this category.22 The relatively better survival in women compared with men may be at least partly explained by the knowledge that female patients with esophageal squamous cell carcinoma may be less likely to be heavy alcohol users than male patients.23 The lower decline in relative survival in recent calendar periods compared with earlier periods may be explained by a stricter selection of patients for surgery over time, who may be more fit and have fewer comorbidities compared with earlier years.24,25 These results indicate that survivors of esophageal cancer may benefit from recommendations of a healthier lifestyle, e.g., regarding tobacco smoking and alcohol consumption, and check-ups for potentially serious comorbidities. These recommendations may be especially relevant for men with a history of squamous cell carcinoma of the esophagus.
In conclusion, this Swedish nationwide and population-based cohort study shows that the life expectancy of esophageal cancer survivors is distinctly poorer than that of the corresponding general population, particularly in those with a history of squamous cell carcinoma of the esophagus and in men.
Human and animal rights
This study is based on original data from medical records and health data registries. No previous study has compared the survival of esophageal cancer patients with that of a corresponding general population. The results indicate that survivors of esophageal cancer, especially men and those with a history of squamous cell carcinoma of the esophagus, benefit from recommendations of a healthier lifestyle, e.g., regarding tobacco smoking and alcohol consumption, and check-ups for potentially serious comorbidities.
Data availability statement
Data are available upon request after approval from the relevant authorities.
References
Sung H, Ferlay J, Siegel RL, Torre LA, Ahmedin J. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. https://doi.org/10.3322/caac.21660.
Lagergren J, Smyth E, Cunningham D, Lagergren P. Oesophageal cancer. Lancet. 2017;390(10110):2383–96.
Montgomery, EA; et al. "Oesophageal Cancer". In Stewart, BW; Wild, CP (eds.). World Cancer Report 2014. World Health Organization.2014. pp. 528–543.
Fitzmaurice C, Akinyemiju TF, Al Lami FH, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: a systematic analysis for the global burden of disease study. JAMA Oncol. 2018
Nationell kvalitetsregisterrapport matstrups- och magsäckscancer. : RCC i Samverkan. Available from: http://www.cancercentrum.se/samverkan/cancerdiagnoser/matstrupeoch-magsack/kvalitetsregister/
Delpisheh A, Veisani Y, Sayehmiri K, Rahimi E. Esophageal carcinoma: long-term survival in consecutive series of patients through a retrospective cohort study. Gastroenterol Hepatol Bed Bench. 2014;7(2):101–7.
Ghaly G, Kamel M, Nasar A, et al. Locally advanced esophageal cancer: what becomes of 5-year survivors? J Thorac Cardiovasc Surg. 2016;151(3):726–32. https://doi.org/10.1016/j.jtcvs.2015.10.096.
Chuang SC, Hashibe M, Scelo G, et al. Risk of second primary cancer among esophageal cancer patients: a pooled analysis of 13 cancer registries. Cancer Epidemiol Biomarkers Prev. 2008;17(6):1543–9.
Martin L, Lagergren J, Lindblad M, Rouvelas I, Lagergren P. Malnutrition after oesophageal cancer surgery in Sweden. Br J Surg. 2007;94(12):1496–500.
Evidence based practice guidelines for the nutritional management of malnutrition in adult patients across the continuum of care. 2009;66(s3):S1-S34
Markar SR, Mackenzie H, Lagergren P, Hanna GB, Lagergren J. Surgical proficiency gain and survival after esophagectomy for cancer. J Clin Oncol. 2016;34(13):1528–36. https://doi.org/10.1200/JCO.2015.65.2875.
Derogar M, Sadr-Azodi O, Johar A, Lagergren P, Lagergren J. Hospital and surgeon volume in relation to survival after esophageal cancer surgery in a population-based study. J Clin Oncol. 2013;31(5):551–7. https://doi.org/10.1200/JCO.2012.46.1517.
Rouvelas I, Zeng W, Lindblad M, Viklund P, Ye W, Lagergren J. Survival after surgery for oesophageal cancer: a population-based study. Lancet Oncol. 2005;6(11):864–70. https://doi.org/10.1016/S1470-2045(05)70347-8.
Lindblad M, Ye W, Lindgren A, Lagergren J. Disparities in the classification of esophageal and cardia adenocarcinomas and their influence on reported incidence rates. Ann Surg. 2006;243(4):479–85. https://doi.org/10.1097/01.sla.0000205825.34452.43.
Lagergren K, Derogar M. Validation of oesophageal cancer surgery data in the Swedish patient registry. Acta Oncol. 2012;51(1):65–8. https://doi.org/10.3109/0284186X.2011.633932.
Brooke HL, Talbäck M, Hörnblad J, et al. The Swedish cause of death register. Eur J Epidemiol. 2017;32(9):765–73. https://doi.org/10.1007/s10654-017-0316-1.
Statistics Sweden/Statistiska Centralbyrån. Om SCB [Internet] Stockholm: Finansdepartementet; 2020 [cited 2020-12-14]. Available from: https://www.scb.se/om-scb/
Cutler SJ, Ederer F. Maximum utilization of the life table method in analyzing survival. J Chronic Dis. 1958;8:699–712.
Darling GE. A dream come true: Long-term survivors of esophageal cancer. J Thorac Cardiovasc Surg. 2016;151(3):733–4. https://doi.org/10.1016/j.jtcvs.2015.11.015.
Ness-Jensen E, Santoni G, Gottlieb-Vedi E, Lindam A, Pedersen N, Lagergren J. Mortality in gastro-oesophageal reflux disease in a population-based nationwide cohort study of Swedish twins. BMJ Open. 2020;10(8):e037456. https://doi.org/10.1136/bmjopen-2020-037456.
Ness-Jensen E, Gottlieb-Vedi E, Wahlin K, Lagergren J. All-cause and cancer-specific mortality in GORD in a population-based cohort study (the HUNT study). Gut. 2018;67(2):209–15. https://doi.org/10.1136/gutjnl-2016-312514.
Duan XF, Tang P, Shang XB, Jiang HJ, Zhao Q, Yu ZT. High body mass index worsens survival in patients with esophageal squamous cell carcinoma after esophagectomy. Dig Surg. 2017;34(4):319–27. https://doi.org/10.1159/000453044.
Morita M, Otsu H, Kawano H, et al. Gender differences in prognosis after esophagectomy for esophageal cancer. Surg Today. 2014;44(3):505–12. https://doi.org/10.1007/s00595-013-0573-x.
Boshier PR, Anderson O, Hanna GB. Transthoracic versus transhiatal esophagectomy for the treatment of esophagogastric cancer: a meta-analysis. Ann Surg. 2011;254(6):894–906. https://doi.org/10.1097/SLA.0b013e3182263781.
Talsma AK, Damhuis RA, Steyerberg EW, Rosman C, van Lanschot JJ, Wijnhoven BP. Determinants of improved survival after oesophagectomy for cancer. Br J Surg. 2015;102(6):668–75. https://doi.org/10.1002/bjs.9792.
Acknowledgments
We would like to thank the members of the Surgical Care Science patient research partnership group for their ideas and comments throughout the development of the study.
Funding
Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
The first author was Ellinor Lundberg who drafted the manuscript. Pernilla Lagergren suggested the research question, Fredrik Mattsson performed the data management and statistical analyses, and Jesper Lagergren was the principal investigator and supervisor. All authors provided critical input on the study protocol, manuscript, and approved the manuscript before submission.
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lundberg, E., Lagergren, P., Mattsson, F. et al. Life Expectancy in Survivors of Esophageal Cancer Compared with the Background Population. Ann Surg Oncol 29, 2805–2811 (2022). https://doi.org/10.1245/s10434-022-11416-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-022-11416-4