
Abstract
Background
In 2002, breast cancer patients with supraclavicular nodal metastases (cN3c) were downstaged from AJCC stage IV to IIIc, prompting management with locoregional treatment. We sought to estimate the impact of multimodal therapy on overall survival (OS) in a contemporary cohort of cN3c patients.
Methods
Women ≥ 18 years with cT1-T4c/cN3c invasive breast cancer who underwent systemic therapy were identified from the 2004–2016 National Cancer Database. We compared three patient cohorts: (a) cN3c + multimodal therapy (systemic therapy, surgery, and radiation); (b) cN3c + non-standard therapy; and, (c) cM1. Logistic regression identified factors associated with receipt of multimodal therapy and Kaplan–Meier was used to estimate unadjusted OS. The Cox proportional hazards model estimated effects of diagnosis and treatment on OS after adjustment.
Results
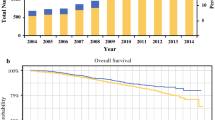
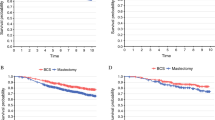
Overall, 1827 (3.7%) patients with cN3c disease and 46,919 (96.3%) cM1 patients were identified. Of cN3c patients, 74.5% (n = 1362) received multimodal therapy and 25.5% (n = 465) received non-standard therapy; receipt of multimodal therapy was associated with improved 5-year OS (multimodal: 59% vs. M1: 28% vs. non-standard: 28%, log-rank p < 0.001). Adjusting for covariates, non-standard therapy was associated with an increased risk of death compared with receipt of multimodal therapy (HR 2.20, 95% CI 1.71–2.83, p < 0.001). Private insurance was the only patient characteristic associated with a greater likelihood of receiving multimodal therapy (OR 2.81; 95% CI, 1.64–4.82; p < 0.001).
Conclusion
Women with cN3c breast cancer who received multimodal therapy demonstrated improved overall survival when compared with patients undergoing non-standard therapy and those with metastatic (M1) disease. Although selection bias may contribute to worse overall survival among cN3c patients undergoing non-standard therapy, national guidelines should encourage locoregional treatment in carefully selected patients.


Similar content being viewed by others
References
Owusu C, Lash TL, Silliman RA. Effect of undertreatment on the disparity in age-related breast cancer-specific survival among older women. Breast Cancer Res Treat. 2007;102(2):227–36.
Poorvu PD et al. Variation in guideline-concordant care for elderly patients with metastatic breast cancer in the United States. Breast Cancer Res Treat. 2018.
Mann JM et al. The State of Surgical Axillary Management and Adjuvant Radiotherapy for Early-stage Invasive Breast Cancer in the Modern Era. Clin Breast Cancer. 2017.
Singletary SE et al. Revision of the American Joint Committee on Cancer staging system for breast cancer. J Clin Oncol. 2002;20(17):3628–36.
Brito RA et al. Long-term results of combined-modality therapy for locally advanced breast cancer with ipsilateral supraclavicular metastases: the University of Texas M.D. Anderson Cancer Center experience. J Clin Oncol. 200119(3):628–33.
Olivotto IA et al. Long-term survival of patients with supraclavicular metastases at diagnosis of breast cancer. J Clin Oncol. 2003;21(5):851–4.
https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf. Accessed 15 Mar 2020.
Fan Y et al. A retrospective study of metachronous and synchronous ipsilateral supraclavicular lymph node metastases in breast cancer patients. Breast. 2010;19(5):365–9.
Shenkier T et al. Clinical practice guidelines for the care and treatment of breast cancer: 15. Treatment for women with stage III or locally advanced breast cancer. CMAJ. 2004;170(6):983–94.
Huang EH et al. Locoregional treatment outcomes for breast cancer patients with ipsilateral supraclavicular metastases at diagnosis. Int J Radiat Oncol Biol Phys. 2007;67(2):490–6.
Chen SC et al. Prognosis of breast cancer after supraclavicular lymph node metastasis: not a distant metastasis. Ann Surg Oncol. 2006;13(11):1457–65.
Surgeons ACO. American College of Surgeons: National Cancer Data Base [cited 2015 June 19th]; Available from: https://www.facs.org/quality-programs/cancer/ncdb. Accessed 1 Aug 2016.
Neter J, Kutner M, Wasserman W, Nachtsheim C. Applied linear statistical models. Vol 4. Chicago: Irwin; 1996.
Greenup RA et al. The effect of hospital volume on breast cancer mortality. Ann Surg. 2018;267(2):375–381.
Caudle AS et al. Predictors of tumor progression during neoadjuvant chemotherapy in breast cancer. J Clin Oncol. 2010;28(11):1821–8.
Plichta J et al. Implications for Breast Cancer Restaging Based on the 8th Edition AJCC Staging Manual. Ann Surg. 2020;271(1):169–76.
Jagsi R et al. Adoption of hypofractionated radiation therapy for breast cancer after publication of randomized trials. Int J Radiat Oncol Biol Phys. 2014;90(5):1001–9.
Ong CT et al. Patient age and tumor subtype predict the extent of axillary surgery among breast cancer patients eligible for the american college of surgeons oncology group trial Z0011. Ann Surg Oncol. 2017;24(12):3559–66.
Freedman RA et al. The association of race/ethnicity, insurance status, and socioeconomic factors with breast cancer care. Cancer. 2011;117(1):180–9.
Chen F et al. Improving breast cancer quality of care with the use of patient navigators. Am Surg. 2010;76(10):1043–6.
Jung J et al. Treatment outcome of breast cancer with pathologically proven synchronous ipsilateral supraclavicular lymph node metastases. J Breast Cancer. 2015;18(2):167–72.
Park HJ et al. Outcomes of positron emission tomography-staged clinical N3 breast cancer treated with neoadjuvant chemotherapy, surgery, and radiotherapy. Int J Radiat Oncol Biol Phys. 2011;81(5):e689–95.
Acknowledgement
Portions of this manuscript were presented at the Society of Surgical Oncology Annual Meeting on March 23, 2018. The National Cancer Data Base (NCDB) is a joint project of the Commission on Cancer (CoC) of the American College of Surgeons and the American Cancer Society. The CoC’s NCDB and the hospitals participating in the CoC NCDB are the source of the de-identified data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Funding
Dr. O. Fayanju was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health (NIH) under Award Number 5KL2TR001115 (PI: Boulware). Dr. R. Greenup was supported by the NIH BIRCWH K12HD043446 (PI: Andrews). This work was also supported by the Duke Cancer Institute through NIH grant P30CA014236 (PI: Kastan). The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Samantha Thomas - Abbvie, Inc: consulting on biosimilar and bioequivalence work unrelated to this work. Jeremy Force - Consulting: Genomic Health.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tamirisa, N.P., Ren, Y., Campbell, B.M. et al. Treatment Patterns and Outcomes of Women with Breast Cancer and Supraclavicular Nodal Metastases. Ann Surg Oncol 28, 2146–2154 (2021). https://doi.org/10.1245/s10434-020-09024-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-020-09024-1