
Abstract
Background
Due to the significant contribution of anastomotic leak, with its disastrous consequences to patient morbidity and mortality, multiple parameters have been proposed and individually meta-analyzed for the formation of the ideal esophagogastric anastomosis following cancer resection. The purpose of this pooled analysis was to examine the main technical parameters that impact on anastomotic integrity.
Methods
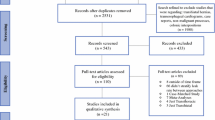
Medline, Embase, trial registries, and conference proceedings were searched. Technical factors evaluated included hand-sewn versus stapled esophagogastric anastomosis (EGA), cervical versus thoracic EGA, minimally invasive versus open esophagectomy, anterior versus posterior route of reconstruction and ischemic conditioning of the gastric conduit. The outcome of interest was the incidence of anastomotic leak, for which pooled odds ratios were calculated for each technical factor.
Results
No significant difference in the incidence of anastomotic leak was demonstrated for the following technical factors: hand-sewn versus stapled EGA, minimally invasive versus open esophagectomy, anterior versus posterior route of reconstruction and ischemic conditioning of the gastric conduit. Four randomized, controlled trials comprising 298 patients were included that compared cervical and thoracic EGA. Anastomotic leak was seen more commonly in the cervical group (13.64 %) than in the thoracic group (2.96 %). Pooled analysis demonstrated a significantly increased incidence of anastomotic leak in the cervical group (pooled odds ratio = 4.73; 95 % CI 1.61–13.9; P = 0.005).
Conclusions
A tailored surgical approach to the patient’s physiology and esophageal cancer stage is the most important factor that influences anastomotic integrity after esophagectomy.





Similar content being viewed by others


References
Biere SS, van Berge Henegouwen MI, Maas KW, et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet. 2012;379:1887–92.
Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90.
Siegel R, Naishadham D, Jemal A. Cancer statistics. CA Cancer J Clin. 2012;62(1):10–29.
Coupland VH, Lagergren J, Luchtenborg M, et al. Hospital volume, proportion resected and mortality from oesophageal and gastric cancer: a population-based study in England, 2004–2009. Gut. 2013;62(7):961–6.
Hanna GB, Boshier PR, Knaggs A, et al. Improving outcomes after gastroesophageal cancer resection: can Japanese results be reproduced in Western centers? Arch Surg. 2012;147(8):738–45.
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88.
Law S, Fok M, Chu KM, et al. Comparison of hand-sewn and stapled esophagogastric anastomosis after esophageal resection for cancer: a prospective randomized controlled trial. Ann Surg. 1997;226(2):169–73.
Hsu HH, Chen JS, Huang PM, et al. Comparison of manual and mechanical cervical esophagogastric anastomosis after esophageal resection for squamous cell carcinoma: a prospective randomized controlled trial. Eur J Cardiothorac Surg. 2004;25(6):1097–101.
Laterza E, de’Manzoni G, Veraldi GF, et al. Manual compared with mechanical cervical oesophagogastric anastomosis: a randomised trial. Eur J Surg. 1999;165(11):1051–4.
Valverde A, Hay JM, Fingerhut A, et al. Manual versus mechanical esophagogastric anastomosis after resection for carcinoma: a controlled trial. French Associations for Surgical Research. Surgery. 1996;120(3):476–83.
Luechakiettisak P, Kasetsunthom S. Comparison of hand-sewn and stapled in esophagogastric anastomosis after esophageal cancer resection: a prospective randomized study. J Med Assoc Thai. 2008;91(5):681–5.
Walther B, Johansson J, Johansson F, et al. Cervical or thoracic anastomosis after esophageal resection and gastric tube reconstruction: a prospective randomized trial comparing sutured neck anastomosis with stapled intrathoracic anastomosis. Ann Surg. 2003;238(6):803–12.
Okuyama M, Motoyama S, Suzuki H, et al. Hand-sewn cervical anastomosis versus stapled intra-thoracic anastomosis after esophagectomy for middle or lower thoracic esophageal cancer: a prospective randomized controlled study. Surg Today. 2007;37(11):947–52.
Craig SR, Walker WS, Cameron EW, et al. A prospective randomized study comparing stapled with handsewn oesophagogastric anastomoses. J R Coll Surg Edinb. 1996;41(1):17–9.
George WD, West of Scotland and Highland Anastomosis Study Group. Suturing or stapling in gastrointestinal surgery: a prospective randomized study. Br J Surg. 1991;78:337–41.
Saluja SS, Ray S, Pal S, et al. Randomized trial comparing side-to-side stapled and hand-sewn esophagogastric anastomosis in neck. J Gastrointest Surg. 2012;16(7):1287–95.
Chasseray VM, Kiroff GK, Buard JL, et al. Cervical or thoracic anastomosis for esophagectomy for carcinoma. Surg Gynecol Obstet. 1989;169(1):55–62.
Ribet M, Debrueres B, Lecomte-Houcke M. Resection for advanced cancer of the thoracic esophagus: cervical or thoracic anastomosis? Late results of a prospective randomized study. J Thorac Cardiovasc Surg. 1992;103(4):784–9.
Lam TC, Fok M, Cheng SW, et al. Anastomotic complications after esophagectomy for cancer. A comparison of neck and chest anastomoses. J Thorac Cardiovasc Surg. 1992;104:395–400.
Nurnberger HR, Lohlein D. Experiences with reliability and rate of complications in collar or thoracic anastomosis after subtotal esophagectomy. Zentralbl Chir. 1994;119:233–9.
Blewett CJ, Miller JD, Young JE, et al. Anastomotic leaks after esophagectomy for esophageal cancer: a comparison of thoracic and cervical anastomoses. Ann Thorac Cardiovasc Surg. 2001;7:75–8.
Egberts JH, Schniewind B, Bestmann B, et al. Impact of the site of anastomosis after oncologic esophagectomy on quality of life–a prospective, longitudinal outcome study. Ann Surg Oncol. 2008;15:566–75.
Klink CD, Binnebosel M, Otto J, et al. Intrathoracic versus cervical anastomosis after resection of esophageal cancer: a matched pair analysis of 72 patients in a single center study. World J Surg Oncol. 2012;10:1477–9.
Ben-David K, Sarosi GA, Cendan JC, et al. Decreasing morbidity and mortality in 100 consecutive minimally invasive esophagectomies. Surg Endosc. 2012;26:162–7.
Berger AC, Bloomenthal A, Weksler B, et al. Oncologic efficacy is not compromised, and may be improved with minimally invasive esophagectomy. J Am Coll Surg. 2011;212(4):560–6.
Gao Y, Wang Y, Chen L, et al. Comparison of open three-field and minimally invasive esophagectomy for esophageal cancer. Interact Cardiovasc Thorac Surg. 2011;12:366–9.
Hamouda AH, Forshaw MJ, Tsigritis K, et al. Perioperative outcomes after transition from conventional to minimally invasive Ivor-Lewis esophagectomy in a specialized center. Surg Endosc. 2010;24:865–9.
Lee JM, Cheng JW, Lin MT, et al. Is there any benefit to incorporating a laparoscopic procedure into minimally invasive esophagectomy? The impact on perioperative results in patients with esophageal cancer. World J Surg. 2011;35:790–7.
Nafteux P, Moons J, Coosemans W, et al. Minimally invasive oesophagectomy: a valuable alternative to open oesophagectomy for the treatment of early oesophageal and gastro-oesophageal junction carcinoma. Eur J Cardiothorac Surg. 2011;40:1455–63.
Safranek PM, Cubitt J, Booth MI, et al. Review of open and minimal access approaches to oesophagectomy for cancer. Br J Surg. 2010;97:1845–53.
Schroder W, Holscher AH, Bludau M, et al. Ivor-Lewis esophagectomy with and without laparoscopic conditioning of the gastric conduit. World J Surg. 2010;34:738–43.
Smithers BM, Gotley DC, Martin I, et al. Comparison of the outcomes between open and minimally invasive esophagectomy. Ann Surg. 2007;245:232–40.
Yamasaki M, Miyata H, Fujiwara Y, et al. Minimally invasive esophagectomy for esophageal cancer: comparative analysis of open and hand-assisted laparoscopic abdominal lymphadenectomy with gastric conduit reconstruction. J Surg Oncol. 2011;104:623–8.
Zingg U, McQuinn A, DiValentino D, et al. Minimally invasive versus open esophagectomy for patients with esophageal cancer. Ann Thorac Surg. 2009;87:911–9.
Biere SS, Maas KW, Cuesta MA, et al. Cervical or thoracic anastomosis after esophagectomy for cancer: a systematic review and meta-analysis. Dig Surg. 2011;28:29–35.
Bartels H, Thorban S, Siewert JR. Anterior versus posterior reconstruction after transhiatal oesophagectomy: a randomized controlled trial. Br J Surg 1993;80:1141–4.
Gawad KA, Hosch SB, Bumann D, et al. How important is the route of reconstruction after esophagectomy: a prospective randomized study. Am J Gastroenterol. 1999;94:1490–6.
van Lanschot JJ, van Blankenstein M, Oei HY, et al. Randomized comparison of prevertebral and retrosternal gastric tube reconstruction after resection of oesophageal carcinoma. Br J Surg. 1999;86:102–8.
Zieren HU, Muller JM, Pichlmaier H. Prospective randomized study of one- or two-layer anastomosis following oesophageal resection and cervical oesophagogastrostomy. Br J Surg. 1993;80:608–11.
Motoyama S, Kitamura M, Saito R, et al. Surgical outcome of colon interposition by the posterior mediastinal route for thoracic esophageal cancer. Ann Thorac Surg. 2007;83:1273–8.
Khiria LS, Pal S, Peush S, et al. Impact on outcome of the route of conduit transposition after transhiatal oesophagectomy: a randomized controlled trial. Dig Liver Dis. 2009;41:711–6.
Chan ML, Hsieh CC, Wang CW, et al. Reconstruction after esophagectomy for esophageal cancer: retrosternal or posterior mediastinal route? J Chin Med Assoc. 2011;74:505–10.
Akiyama S, Ito S, Sekiguchi H, et al. Preoperative embolization of gastric arteries for esophageal cancer. Surgery. 1996;120:542–6.
Akiyama S, Kodera Y, Sekiguchi H, et al. Preoperative embolization therapy for esophageal operation. J Surg Oncol. 1998;69:219–23.
Isomura T, Itoh S, Akiyama S, et al. Efficacy of gastric blood supply redistribution by transarterial embolization: preoperative procedure to prevent postoperative anastomotic leaks following esophagoplasty for esophageal carcinoma. Cardiovasc Intervent Radiol. 1999;22:119–23.
Diana M, Hubner M, Vuilleumier H, et al. Redistribution of gastric blood flow by embolization of gastric arteries before esophagectomy. Ann Thorac Surg. 2011;91:1546–51.
Farran L, Miro M, Alba E, et al. Preoperative gastric conditioning in cervical gastroplasty. Dis Esophagus. 2011;24:205–10.
Nguyen NT, Nguyen XT, Reavis KM, et al. Minimally invasive esophagectomy with and without gastric ischemic conditioning. Surg Endosc. 2012;26:1637–41.
Perry KA, Enestvedt CK, Pham TH, et al. Esophageal replacement following gastric devascularization is safe, feasible, and may decrease anastomotic complications. J Gastrointest Surg. 2010;14:1069–73.
Berrisford RG, Veeramootoo D, Parameswaran R, et al. Laparoscopic ischaemic conditioning of the stomach may reduce gastric-conduit morbidity following total minimally invasive oesophagectomy. Eur J Cardiothorac Surg. 2009;36:888–93.
Veeramootoo D, Shore AC, Shields B, et al. Ischemic conditioning shows a time-dependent influence on the fate of the gastric conduit after minimally invasive esophagectomy. Surg Endosc. 2010;24:1126–31.
Wajed SA, Veeramootoo D, Shore AC. Surgical optimisation of the gastric conduit for minimally invasive oesophagectomy. Surg Endosc. 2012;26:271–6.
Zahedi M, Ganai S, Yetasook AK, et al. Laparoscopic ischemic conditioning as a modality to reduce gastric conduit morbidity following esophagectomy. Digestive Disease Week 2012; Poster presentation.
Law S, Wong KH, Kwok KF, et al. Predictive factors for postoperative pulmonary complications and mortality after esophagectomy for cancer. Ann Surg. 2004;240:791–800.
Marietter C, Taillier G, Van Seuningen I, et al. Factors affecting postoperative course and survival after en bloc resection for esophageal carcinoma. Ann Thorac Surg. 2004;78:1177–83.
Noble F, Curtis N, Harris S, South Coast Cancer Collaboration-Oesophago-Gastric (SC-OG), et al. Risk assessment using a novel score to predict anastomotic leak and major complications after oesophageal resection. J Gastrointest Surg. 2012;16:1083–95.
Alanezi K, Urschel JD. Mortality secondary to esophageal anastomotic leak. Ann Thorac Cardiovasc Surg. 2004;10:71–5.
Hulscher JB, Tijssen JG, Obertop H, et al. Transthoracic versus transhiatal resection for carcinoma of the esophagus: a meta-analysis. Ann Thorac Surg. 2001;72:306–13.
Verhoef C, van der Weyer R, Schaapveld M, et al. Better survival in patients with esophageal cancer after surgical treatment in university hospitals: a plea for performance by surgical oncologists. Ann Surg Oncol. 2007;14:1678–87.
Markar SR, Karthikesalingam A, Vyas S, et al. Hand-sewn versus stapled oesophago-gastric anastomosis: systematic review and meta-analysis. J Gastrointest Surg. 2011;15(5):876–84.
Blencowe NS, Strong S, McNair AG, et al. Reporting of short-term clinical outcomes after esophagectomy: a systematic review. Ann Surg. 2012;255:658–66.
Carrott PW, Markar SR, Kuppusamy MK, et al. Accordian severity grading system: assessment of relationship between costs, length of hospital stay, and survival in patients with complications after esophagectomy for cancer. J Am Coll Surg. 2012;215(3):331–6.
Markar SR, Karthikesalingam A, Low DE. Outcomes assessment of the surgical management of esophageal cancer in younger and older patients. Ann Thorac Surg. 2012;94(5):1652–8.
Schroder W, Beckurts KT, Stahler D, et al. Microcirculatory changes associated with gastric tube formation in the pig. Eur Surg Res. 2002;34:411–7.
National Oesophago-Gastric Cancer Audit—The Royal College of Surgeons of England 2010.
Luketich JD, Pennathur A, Awais O, et al. Outcomes after minimally invasive esophagectomy: review of over 1000 patients. Ann Surg. 2012;256(1):95–103.
Reavis KM, Chang EY, Hunter JG, Jobe BA. Utilization of the delay phenomenon improves blood flow and reduces collage deposition in esophagogastric anastomoses. Ann Surg. 2005;241:736–47.
Urschel JD, Antkowiak JG, Delacure MD, Takita H. Ischemic conditioning (delay phenomenon) improves esophagogastric anastomotic wound healing in the rat. J Surg Oncol. 1997;66:254–6.
Stiles BM, Mirza F, Coppolino A, et al. Clinical T2-T3N0MO esophageal cancer: the risk of node positive disease. Ann Thorac Surg. 2011;92(2):491–6.
Hamai Y, Hihara J, Emi M, et al. Esophageal reconstruction using the terminal ileum and right colon in esophageal cancer surgery. Surg Today. 2012;42(4):342–50.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Markar, S.R., Arya, S., Karthikesalingam, A. et al. Technical Factors that Affect Anastomotic Integrity Following Esophagectomy: Systematic Review and Meta-analysis. Ann Surg Oncol 20, 4274–4281 (2013). https://doi.org/10.1245/s10434-013-3189-x
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-013-3189-x