
Abstract
Purpose
To test whether the rates of in-hospital mortality, complications, and transfusions are higher in patients treated with cytoreductive nephrectomy (CNT) for metastatic renal cell carcinoma (mRCC) relative to patients treated with nephrectomy (NT) for non-mRCC.
Methods
We assessed 17,688 patients treated with a NT between years 1999 and 2008, within the Florida Inpatient Database. Chi-square and Student t-tests were used to compare the statistical significance of differences in proportions and means, respectively. Univariable and multivariable logistic regression analyses tested the relationship between surgery type (CNT vs. NT) and three end points: in-hospital mortality, complications, and transfusions.
Results
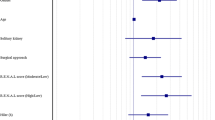
Overall, 6.0% of patients underwent CNT. The rates of in-hospital mortality, complications, and transfusions were 2.4, 26.5, and 24.3% in CNT patients versus 0.9, 18.9, and 11.1% in NT patients. At multivariable analyses, CNT patients demonstrated a 2.0-, 1.3-, and 2.4-fold higher risk of in-hospital mortality, complications, and transfusions (all P < 0.001). Similarly, more advanced age, comorbidity, and the cumulative number of secondary surgical procedures were independent predictors of a higher risk of in-hospital mortality, complications, and transfusions (all P < 0.001).
Conclusions
The rate of in-hospital mortality, complications, and transfusions is higher in patients treated with CNT relative to NT. Older age, higher comorbidity, and the necessity of secondary surgical procedures further increases the risk of all aforementioned end points. Physicians should consider these observations during the planning of a CNT, and patients should be informed accordingly.
Similar content being viewed by others

References
NCCN (2010) NCCN clinical practice guidelines in oncology. Kidney cancer. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp.
Flanigan RC, Salmon SE, Blumenstein BA, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer. N Engl J Med. 2001;345:1655–9.
Mickisch GH, Garin A, van Poppel H, et al. Radical nephrectomy plus interferon-alfa-based immunotherapy compared with interferon alfa alone in metastatic renal-cell carcinoma: a randomised trial. Lancet. 2001;358:966–70.
Flanigan RC, Mickisch G, Sylvester R, et al. Cytoreductive nephrectomy in patients with metastatic renal cancer: a combined analysis. J Urol. 2004;171:1071–6.
Bennett RT, Lerner SE, Taub HC, et al. Cytoreductive surgery for stage IV renal cell carcinoma. J Urol. 1995;154:32–4.
Fallick ML, McDermott DF, LaRock D, et al. Nephrectomy before interleukin-2 therapy for patients with metastatic renal cell carcinoma. J Urol. 1997;158:1691–5.
Levy DA, Swanson DA, Slaton JW, et al. Timely delivery of biological therapy after cytoreductive nephrectomy in carefully selected patients with metastatic renal cell carcinoma. J Urol. 1998;159:1168–73.
Walther MM, Alexander RB, Weiss GH, et al. Cytoreductive surgery prior to interleukin-2-based therapy in patients with metastatic renal cell carcinoma. Urology. 1993;42:250–7.
Walther MM, Yang JC, Pass HI, et al. Cytoreductive surgery before high dose interleukin-2 based therapy in patients with metastatic renal cell carcinoma. J Urol. 1997;158:1675–8.
Matin SF, Madsen LT, Wood CG. Laparoscopic cytoreductive nephrectomy: the M. D. Anderson Cancer Center experience. Urology. 2006;68:528–32.
Goetzl MA, Goluboff ET, Murphy AM, et al. A contemporary evaluation of cytoreductive nephrectomy with tumor thrombus: morbidity and long-term survival. Urol Oncol. 2004;22:182–7.
Margulis V, Matin SF, Tannir N, et al. Surgical morbidity associated with administration of targeted molecular therapies before cytoreductive nephrectomy or resection of locally recurrent renal cell carcinoma. J Urol. 2008;180:94–8.
Florida Health Finder. http://www.floridahealthfinder.gov/researchers/researchers.aspx. Accessed 14 June 2010.
Statistics. Hysterectomy hospitalizations, 1993–2002. Health outcome series. 2004, p 5. http://edocs.dlis.state.fl.us/fldocs/ahca/Hoseries/hysterectomy_hospitalizations2004.pdf.
Romano PS, Roos LL, Jollis JG. Adapting a clinical comorbidity index for use with ICD-9-CM administrative data: differing perspectives. J Clin Epidemiol. 1993;46:1075–9.
Joudi FN, Allareddy V, Kane CJ, et al. Analysis of complications following partial and total nephrectomy for renal cancer in a population based sample. J Urol. 2007;177:1709–14.
Jeldres C, Baillargeon-Gagne S, Liberman D, et al. A population-based analysis of the rate of cytoreductive nephrectomy for metastatic renal cell carcinoma in the United States. Urology. 2009;74:837–41.
Budaus L, Sun M, Abdollah F, et al. Impact of surgical experience on in-hospital complication rates in patients undergoing minimally invasive prostatectomy: a population-based study. Ann Surg Oncol. 2011;18:839–47.
Konety BR, Allareddy V, Herr H. Complications after radical cystectomy: analysis of population-based data. Urology. 2006;68:58–64.
Alibhai SM, Leach M, Tomlinson G. Impact of hospital and surgeon volume on mortality and complications after prostatectomy. J Urol. 2008;180:155–62.
Begg CB, Riedel ER, Bach PB, et al. Variations in morbidity after radical prostatectomy. N Engl J Med. 2002;346:1138–44.
Hu JC, Wang Q, Pashos CL, et al. Utilization and outcomes of minimally invasive radical prostatectomy. J Clin Oncol. 2008;26:2278–84.
Clavien PA, Sanabria JR, Strasberg SM. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery. 1992;111:518–26.
Lawthers AG, McCarthy EP, Davis RB, et al. Identification of in-hospital complications from claims data. Is it valid? Med Care. 2000;38:785–95.
CARMENA. Randomized phase III trial evaluating the importance of nephrectomy in patients presenting with metastatic renal cell carcinoma treated with sunitinib. http://clinicaltrials.gov/ct2/show/NCT00930033?term=renal+cancer&recr=Open&intr=nephrectomy&rank=2 (2009).
EORTC. Randomized Phase III trial comparing presurgical sunitinib followed by nephrectomy and sunitinib versus nephrectomy followed by sunitinib in patients with synchronous metastatic renal cell carcinoma. http://www.eortc.be/protoc/Details.asp?Protocol=30073&T= (2008, updated February 2010).
Halbert R, Figlin R, Atkins M, et al. Treatment of patients with metastatic renal cell cancer. Cancer. 2006;107:2375–83.
Mitchell RE, Lee BT, Cookson MS, et al. Immediate surgical outcomes for radical prostatectomy in the University HealthSystem Consortium Clinical Data Base: the impact of hospital case volume, hospital size and geographical region on 48,000 patients. BJU Int. 2009;104:1442–5.
Acknowledgment
Pierre I. Karakiewicz is partially supported by the University of Montreal Health Centre Urology Specialists, Fonds de la Recherche en Sante du Quebec, the University of Montreal Department of Surgery and the University of Montreal Health Centre (CHUM) Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Firas Abdollah and Maxine Sun contributed equally to this work.
Appendix
Appendix
Rights and permissions
About this article
Cite this article
Abdollah, F., Sun, M., Thuret, R. et al. Mortality and Morbidity After Cytoreductive Nephrectomy for Metastatic Renal Cell Carcinoma: A Population-Based Study. Ann Surg Oncol 18, 2988–2996 (2011). https://doi.org/10.1245/s10434-011-1715-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-011-1715-2