
Abstract
Background
Although neoadjuvant chemotherapy (NCT) is standard therapy for locally advanced breast cancer, it remains controversial for early-stage disease due to concerns that disease progression may make breast-conservation therapy (BCT), or even operability, impossible. The goal of this study was to determine the impact of disease progression during NCT on surgical management.
Methods
We reviewed clinicopathological data on patients who received NCT for stage I-III breast cancer from 1994 to 2007. Chemotherapy regimens were anthracycline- and/or taxane-based as determined by the treating medical oncologist.
Results
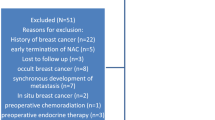
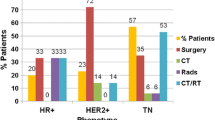
Of 1,928 patients who received NCT, 1,762 (91%) had a partial or complete response, 107 (6%) had stable disease (SD), and 59 (3%) progressed (PD) while receiving at least one regimen. Of the patients with progressive disease, 40 (68%) patients underwent mastectomy, 12 (20%) underwent BCT, and 7 (12%) did not undergo surgery. In patients who underwent mastectomy, only three (8%) were BCT candidates before progression. Overall, disease progression changed the operative plan in 11 (0.5%) patients: 3 developed distant metastasis, 2 developed clinical lymphadenopathy, 3 required mastectomy instead of BCT, 2 became inoperable, and 1 required flap closure.
Conclusions
Disease progression while receiving NCT is infrequent (3%), but early identification may allow for change to other, potentially beneficial, therapeutic interventions. Patients with breast cancer who receive NCT should be evaluated frequently for response to therapy. Overall, progression during NCT changes the surgical management in a small proportion of patients.


Similar content being viewed by others

References
Hunt K, Yi M, Mittendorf E, et al. Sentinel lymph node surgery after neoadjuvant chemotherapy is accurate and reduces the need for axillary dissection in breast cancer patients. Ann Surg. 2009.
Eisenhauer E, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–47.
Caudle A, Gonzalez-Angulo A, Hunt K, et al. Predictors of tumor progression during neoadjuvant chemotherapy in breast cancer. J Clin Oncol. 2010;28:1821–28.
Fisher B, Bryant J, Wolmark N, et al. Effect of pre-operative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol. 1998;16:2672–85.
van Nes J, Putter H, Julien J, et al. Preoperative chemotherapy is safe in early breast cancer, even after 10 years of follow-up; clinical and translational results from the EORTC trial 10902. Breast Cancer Res Treat. 2009;115:101–13.
Bear H, Anderson S, Smith R, et al. Sequential preoperative or postoperative docetaxel added to preoperative doxorubicin plus cyclophosphamide for operable breast cancer: National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol. 2006;24:2019–27.
van der Hage J, van de Velde C, Julien J, et al. Preoperative chemotherapy in primary operable breast cancer: results from the European Organization for Research and Treatment of Cancer trial 10902. J Clin Oncol. 2002;20:2905–6.
Boughey J, Peintinger F, Meric-Bernstam F, et al. Impact of preoperative versus postoperative chemotherapy on the extent and number of surgical procedures in patients treated in randomized clinical trials for breast cancer. Ann Surg. 2006;244:464–70.
Taylor M, Perez C, Halverson K, et al. Factors influencing cosmetic results after conservation therapy for breast cancer. Int J Radiat Oncol Biol Phys. 1995;31:753–64.
Christy C, Thorsteinsson D, Grube B, et al. Preoperative chemotherapy decreases the need for re-excision of breast cancers between 2 and 4 cm diameter. Ann Surg Oncol. 2009;16:697–702.
Shen J, Valero V, Buchholz T, et al. Effective local control and long-term survival in patients with T4 locally advanced breast cancer treated with breast conservation therapy. Ann Surg Oncol. 2004;11:854–60.
Chagpar A, Middleton L, Sahin A, et al. Accuracy of physical examination, ultrasonography, and mammography in predicting residual pathologic tumor size in patients treated with neoadjuvant chemotherapy. Ann Surg. 2006;243:257–64.
Boughey J, Wagner J, Garrett B, et al. Neoadjuvant chemotherapy in invasive lobular carcinoma may not improve rates of breast conservation. Ann Surg Oncol. 2009;16:1606–11.
Faneyte I, Schrama J, Peterse J, et al. Breast cancer response to neoadjuvant chemotherapy: predictive markers and relation with outcome. Br J Cancer. 2003;88:406–12.
Dowsett M, Dunbier A. Emerging biomarkers and new understanding of traditional markers in personalized therapy for breast canc. Clin Cancer Res. 2008;14:8019–26.
Acknowledgment
Supported by National Institutes of Health T32 Institutional Research Training Grant (CA09599; F.M.-B. and A.S.C.), Susan G. Komen for the Cure grant (KG090341; A.M.G.-A.) and by the National Institutes of Health through M.D. Anderson’s Cancer Center Support Grant CA016672.
Conflict of Interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Caudle, A.S., Gonzalez-Angulo, A.M., Hunt, K.K. et al. Impact of Progression During Neoadjuvant Chemotherapy on Surgical Management of Breast Cancer. Ann Surg Oncol 18, 932–938 (2011). https://doi.org/10.1245/s10434-010-1390-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-010-1390-8