
Abstract
Background
Esophageal carcinoma has poor prognosis. Surgery is still considered to be the mainstay of treatment. The mortality rate within the first year after surgery is unknown, but identifying risk factors for early mortality would increase our ability to predict the outcome of these patients and might improve patient selection.
Methods
All patients who had undergone subtotal esophagectomy for cancer between 2003 and 2008 were included in this retrospective series. Patients with less than 12 months follow-up, perioperative mortality, and death from unrelated causes were excluded. Patients were divided into two groups. Group A included all oncological mortality cases within 12 months of surgery. Group B included all patients who survived longer than 12 months following surgery.
Results
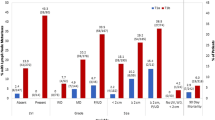
Of 81 patients who met the inclusion criteria, group A included 18 patients and group B included 63 (median survival 10 and 25 months, respectively). A higher proportion of patients were operated for pN1 disease in group A (72% versus 33%, p = 0.0004). R0 esophagectomy rate was lower in group A (39% versus 76%, p = 0.03). Metastatic lymph node ratio (LNR) was higher in group A (mean: 46% versus 10%, p = 0.0003). Multivariate analysis identified LNR as an independent risk factor for first-year oncological mortality [odds ratio (OR) = 1.04, p = 0.0001; 95% confidence interval (CI): 1.02–1.06]. No differences were found in preoperative variables including age, gender, tumor histology, type of operation, and administration of or response to neoadjuvant therapy. Response to neoadjuvant therapy was associated with R0 resection.
Conclusions
pN1 disease, resection margin involvement, and high LNR were found to be risk factors for first-year oncological mortality after esophagectomy for cancer.


Similar content being viewed by others


References
Muller JM et al. Surgical therapy of oesophageal carcinoma. Br J Surg. 1990;77(8):845–57.
Sabanathan S, et al. Results of surgical treatment of oesophageal cancer. J R Coll Surg Edinb. 1996;41(5):295–301.
Morstyn G, et al. Improved survival in esophageal cancer in the period 1978 to 1983. J Clin Oncol. 1986;4(7):1062–7.
Wu PC, Posner MC. The role of surgery in the management of oesophageal cancer. Lancet Oncol. 2003;4(8):481–8.
Pines G, et al. The use of circular stapler for cervical esophagogastric anastomosis after esophagectomy: surgical technique and early postoperative outcome. Dis Esophagus. 2009;22(3):274–8.
Bedenne L, et al. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J Clin Oncol. 2007;25(10):1160–8.
Coia LR, et al. Long-term results of infusional 5-FU, mitomycin-C and radiation as primary management of esophageal carcinoma. Int J Radiat Oncol Biol Phys. 1991;20(1):29–36.
Leichman L, et al. Nonoperative therapy for squamous-cell cancer of the esophagus. J Clin Oncol. 1987;5(3):365–70.
Seitz JF, et al. Inoperable nonmetastatic squamous cell carcinoma of the esophagus managed by concomitant chemotherapy (5-fluorouracil and cisplatin) and radiation therapy. Cancer. 1990;66(2):214–9.
Sobon LH, Wittekind, C, editors. UICC TNM classification of malignant tumors. 6th ed. New York: Wiley; 2002.
Eisenhauer EA, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47.
Idelevich E, et al. Overall survival with cisplatin and 5-fluorouracil neoadjuvant treatment in patients with esophageal cancer: single-center experience. Onkologie. 2008;31(12):673–7.
Allum WH, et al. Long-term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J Clin Oncol. 2009;27(30):5062–7.
Stahl M, et al. Chemoradiation with and without surgery in patients with locally advanced squamous cell carcinoma of the esophagus. J Clin Oncol. 2005;23(10):2310–7.
Wijnhoven BP, et al. An evaluation of prognostic factors and tumor staging of resected carcinoma of the esophagus. Ann Surg. 2007;245(5):717–25.
Thompson SK, et al. Improving the accuracy of TNM staging in esophageal cancer: a pathological review of resected specimens. Ann Surg Oncol. 2008;15(12):3447–58.
Rice TW, et al. Cancer of the esophagus and esophagogastric junction: data-driven staging for the seventh edition of the American Joint Committee on Cancer/International Union Against Cancer Cancer Staging Manuals. Cancer. 2010;116(16):3763–73.
Peyre CG, et al. Predicting systemic disease in patients with esophageal cancer after esophagectomy: a multinational study on the significance of the number of involved lymph nodes. Ann Surg. 2008;248(6):979–85.
Nitti D, et al. Ratio between metastatic and examined lymph nodes is an independent prognostic factor after D2 resection for gastric cancer: analysis of a large European monoinstitutional experience. Ann Surg Oncol. 2003;10(9):1077–85.
Peng J, et al. Prognostic significance of the metastatic lymph node ratio in node-positive rectal cancer. Ann Surg Oncol. 2008;15(11):3118–23.
Bando E, et al. Outcome of ratio of lymph node metastasis in gastric carcinoma. Ann Surg Oncol. 2002;9(8):775–84.
Nigro JJ, et al. Node status in transmural esophageal adenocarcinoma and outcome after en bloc esophagectomy. J Thorac Cardiovasc Surg. 1999;117(5):960–8.
Darling G. The role of lymphadenectomy in esophageal cancer. J Surg Oncol. 2009;99(4):189–93.
Mariette C, et al. The number of metastatic lymph nodes and the ratio between metastatic and examined lymph nodes are independent prognostic factors in esophageal cancer regardless of neoadjuvant chemoradiation or lymphadenectomy extent. Ann Surg. 2008;247(2):365–71.
Dexter SP, et al. Circumferential resection margin involvement: an independent predictor of survival following surgery for oesophageal cancer. Gut. 2001;48(5):667–70.
Scheepers JJ, et al. Influence of circumferential resection margin on prognosis in distal esophageal and gastroesophageal cancer approached through the transhiatal route. Dis Esophagus. 2009;22(1):42–8.
Barbour AP, et al. Adenocarcinoma of the gastroesophageal junction: influence of esophageal resection margin and operative approach on outcome. Ann Surg. 2007;246(1):1–8.
Griffiths EA, et al. The prognostic value of circumferential resection margin involvement in oesophageal malignancy. Eur J Surg Oncol. 2006;32(4):413–9.
Machlenkin S, Melzer E, Idelevich E, Ziv-Sokolovsky N, Klein Y, Kashtan H. Endoscopic ultrasound: doubtful accuracy for restaging of esophageal cancer after preoperative chemotherapy. Isr Med Assoc J. 2009;11(3):166–9.
Krasna MJ, et al. Combined thoracoscopic/laparoscopic staging of esophageal cancer. J Thorac Cardiovasc Surg. 1996;111(4):800–6; discussion 806–7.
Krasna MJ, et al. CALGB 9380: a prospective trial of the feasibility of thoracoscopy/laparoscopy in staging esophageal cancer. Ann Thorac Surg. 2001;71(4):1073–9.
Krasna MJ, et al. Thoracoscopy/laparoscopy in the staging of esophageal cancer: Maryland experience. Surg Laparosc Endosc Percutan Tech. 2002;12(4):213–8.
Acknowledgment
The authors wish to thank Mario Baras, Ph.D. for his assistance in the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pines, G., Klein, Y., Buyeviz, V. et al. Disease-Related Mortality within the First Year after Subtotal Esophagectomy for Cancer. Ann Surg Oncol 18, 1139–1144 (2011). https://doi.org/10.1245/s10434-010-1386-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-010-1386-4