
Abstract
Background
The aim of this study was to asses quality of life (QoL) after axillary or inguinal sentinel lymph node biopsy (SLNB) with or without completion lymph node dissection (CLND) in patients with cutaneous melanoma by comparing patients to a norm group of the general population and by comparing QoL between four patient groups depending on surgical procedure and location, i.e., patients receiving an axillary or groin SLNB, or an axillary or groin CLND.
Methods
Between 1995 and 2003, a total of 242 axillary and inguinal SLNBs were performed. Of the 127 patients eligible for the study, 116 patients participated (91%). QoL was measured by the 30-item European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30), the McGill Pain Questionnaire and the Groningen Activity Restriction Scale.
Results
Median age at diagnosis was 50 (range, 18–77) years; median Breslow thickness 2.0 (range, 1–13) mm; median follow-up 56 (range, 4–94) months. SLNB only was performed in 89 patients (77%): 48 in the groin and 41 in the axilla. CLND was performed in 27 patients (23%): 13 in the axilla and 14 in the groin. More postoperative complications (13 vs. 5; P < 0.001) and lymphedema (10 vs. 8; P < 0.001) occurred in the CLND group than in the SLNB group. The total group of patients reported better physical (P < 0.001), role (P < 0.001), emotional (P < 0.001), and social functioning (P = 0.049), global QoL (P < 0.001), and less fatigue (P < 0.001) and pain (P < 0.001) than a German norm group. Analysis of variance revealed significant differences in role functioning (P = 0.02) and tendencies toward physical problems (P = 0.051) and fatigue (P = 0.051) between the four groups. Post hoc Bonferroni tests showed that the axillary CLND group had more problems than the axillary and inguinal SLNB groups. Kruskal-Wallis tests showed that the axillary CLND group reported most pain.
Conclusions
QoL in melanoma survivors after axillary or inguinal SLNB with or without CLND was better than that in a norm group. Patients who underwent CLND in the axilla after SLNB reported most problems.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Cancer patients experience numerous problems in physical, emotional, social, practical, and spiritual functioning. Those who survive their disease reportedly continue to experience physical and psychosocial problems, such as functional impairment; worries about recurrence, second malignancies, or late effects of treatment; and employment, financial, or insurance problems.1,2 However, comparable or even better quality of life (QoL) has been found in cancer survivors, as well as in long-term melanoma survivors treated with isolated limb perfusion.3–6
Sentinel lymph node biopsy (SLNB) was developed by Morton et al. in the 1990s to stage patients with clinical stage I or II cutaneous melanoma.7 Over the years, it has proved to be a reliable staging method.8 Recently, the results of the first multicenter selective lymphadenectomy trial (MSLT I) have been published. The third interim analysis showed that SLNB led to improved disease-free survival, but not to improved survival.9 If SLNB is tumor positive, completion lymph node dissection (CLND) is recommended. At present, the MSLT II is investigating whether CLND may be omitted in some patients with a tumor-positive SLNB.10
Various studies on breast cancer patients showed that axillary SLNB led to less short-term and long-term morbidity than completion axillary lymph node dissection (ALND).11–14 Studies on QoL in breast cancer patients did not detect any difference between patients who underwent SLNB alone and patients who underwent SLNB and ALND, whereas other studies showed that ALND was associated with impaired QoL.15–19
In melanoma patients, complication rates after SLNB (such as postoperative bleeding, infection, and lymphedema) varied between 4.6 and 10.1%.8,20,21 Recent studies have reported that morbidity after SLNB alone in melanoma patients was lower than that after SLNB followed by CLND.20,22,23 In particular, the groin dissections after SLNB were associated with more complications than SLNB alone.23 A recent study found a negative correlation between complications and QoL in breast cancer patients.16
To our knowledge, QoL studies in melanoma patients after SLNB in the axilla or the groin, whether in combination with CLND or not, have not been carried out. In the absence of data from the literature, we first hypothesized that QoL in stage I–II melanoma patients after SLNB would be the same as that in the normal population. These patients have a relatively favorable prognosis. However, melanoma patients who underwent a lymph node dissection, in particular in the groin, experience increased morbidity. Therefore, we also hypothesized that patients with inguinal CLND would have more QoL-related problems than patients with SLNB alone and patients with an axillary CLND.
Patients and Methods
Patient Population
In the period 1995–2003, a total of 242 patients underwent inguinal and/or axillary SLNB at the University Medical Center Groningen as a staging procedure for stage I/II cutaneous melanoma (>1.0 mm). We excluded 46 patients who had died and 69 patients for one of the following reasons: bilateral axillary or inguinal SLNBs, follow-up in a different area as a result of moving house, preexisting functional limitations and/or previous surgery to the relevant extremities, preexisting volume discrepancies in the relevant extremities (e.g., status after stroke), severe comorbidity such as dementia or disseminated disease, patients undergoing palliative therapy, and patients who were receiving treatment for local or locoregional recurrence at the time of the study.
Therefore, 127 patients were suitable candidates to take part in this study. They were approached by telephone by the research physician. Information about the study was given verbally and they were invited to participate. At their next outpatient follow-up visit, 116 patients (response rate 91%) provided written informed consent. These patients underwent physical examination and were asked to fill in the questionnaire at home and return it to us in the self-addressed, stamped envelope provided. All the patients returned the questionnaire. The internal review board of the hospital approved the study.
SLNB Technique
Patients were admitted to the hospital to undergo the SLNB, reexcision of scar tissue, and possible CLND. The SLNB procedure has been described in detail previously.24 Excision specimens were sent for routine histopathological analysis with hematoxylin-eosin (HE) staining. Specific immunohistochemical staining was performed on HE-negative specimens for the protein S100 and the melanoma-related antigen HMB45. If histopathological examination of the sentinel lymph node revealed metastatic melanoma tissue, then all those patients received CLND. ALND comprised level I–III axillary dissection with preservation of the pectoralis minor muscle. In the case of a tumor-positive SLNB in the groin, superficial and deep groin lymph node dissections were performed, in which the femoroinguinal lymph nodes and the lymph nodes along the iliac artery and vein were excised, together with the obturator lymph nodes. After superficial lymphadenectomy, the sartorius muscle was freed from its attachment to the anterior superior iliac spine, moved in a medial direction, and fixed to the ligament of Poupart. This technique has been described extensively in the past.25 Since 2002, patients with HE-negative and immunohistochemistry-positive sentinel lymph nodes underwent superficial lymphadenectomy alone. If additional positive lymph nodes were found in the resection specimen, deep groin dissection (iliac and obturator nodal dissection) was performed.
Instruments
Demographic data (sex, age) and clinical data were extracted from the medical files. Complications in the first 30 days postoperatively comprised wound infection, bleeding, seroma, and wound necrosis.
To determine the degree of lymphedema, the volumes of the arms and/or legs were measured by an adapted version of the water displacement technique as described by Kissin et al.26 Each arm or leg was submerged slowly in a large, transparent water-filled cylinder until the level of the axillary fold or inguinal fold was reached. The extremity was then withdrawn from the cylinder and the displaced water refilled in precise quantities and recorded as the volume of the relevant arm or leg. Both healthy and affected extremities were measured. Lymphedema in the groin was classified according to the criteria formulated by Baas (normal 0–6.5%, slight 6.5–20%, moderate 20–40%, severe >40%). Lymphedema in the axilla was classified according to the criteria formulated by Stillwell (normal 0–10%, slight 10–20%, moderate 20–40%, marked 40–80%, severe >80%).25,27
Quality of Life
The 30-item European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) version 3.0 (Dutch version) consists of five multi-item functional scales, three symptom scales, a global health status/QoL scale, and six single items.28 Transformation of the scores was performed according to the instructions in the manual. Scores on all the scales and single items could range from 0 to 100. Higher scores on the functional and global health status QoL scales reflect better functioning. On the symptom scales, higher scores mean more symptoms or problems. A difference of 5–10 points on an EORTC QoL functional subscale is considered to be a small clinically meaningful difference, a difference of 10–20 points is considered to be a moderate clinically meaningful difference, and a difference of >20 points is considered to be a large clinically meaningful difference.29 In this study, the functional scales and the symptom scales “fatigue” and “pain” were included in the analyses.
To make comparisons with a normal population, use was made of the reference data from the EORTC QLQ-C30 (n = 2,028).30 The only general population data available is that of a German reference group. This norm population was selected at random. Mean age of the population was 49.4 (standard deviation [SD] 17.2) years, and 56% were women.
Pain
Pain was measured with the Dutch version of the McGill Pain Questionnaire.31 This questionnaire comprises a number of groups of pain adjectives that within each group reflect an ascending order of pain intensity. The patient is asked to choose one word from each group that best describes the pain. The adjectives are grouped onto three categories that describe separate dimensions of pain: sensory adjectives that describe how the pain feels, affective adjectives that reflect emotions such as anxiety and tension, and evaluative adjectives that express the subjective intensity of the pain. Two scores are calculated from the adjective list: the number of adjectives chosen (McGill Pain Questionnaire, Number of Words Chosen (MPQ-NWC)), and the intensity of these adjectives (sum of the order of the words chosen; MPQ Pain Rating Index (MPQ-PRI)). The higher the score, the more severe the pain. In addition, a visual analog scale was used to measure pain intensity (0 = no pain; 100 = unbearable pain).
Activities of Daily Living
The Groningen Activity Restriction Scale (GARS) measures restrictions in the execution of 18 general activities of daily living.32,33 For each of these items, the patient is asked whether he or she can perform the activity independently and without difficulty (score 1), independently but with some difficulty (score 2), independently but with great difficulty (score 3), or cannot perform the activity independently (only with the help of others; score 4). Scores can therefore vary between 18 and 72 points. A higher score reflects more functional restrictions.
Statistical Analysis
Descriptive statistics were used to analyze the patients. The χ2 and t-tests were used to compare the demographic data and disease-related characteristics between the SLNB tumor-negative group and the tumor-positive group. Unpaired t-tests were computed to compare the patients to the norm group. An analysis of variance (ANOVA) was performed, followed by post hoc Bonferroni tests when the ANOVA was statistically significant, to detect differences between the following four groups: patients with tumor-negative axillary SLNB (axillary SLNB), patients with tumor-positive axillary SLNB followed by ALND (axillary CLND), patients with tumor-negative inguinal SLNB (groin SLNB), and patients with tumor-positive inguinal SLNB followed by inguinal lymph node dissection (groin CLND). In addition, the Kruskal-Wallis test was used to deal with the small numbers. Differences with a P value of <0.05 were considered to be statistically significant. SPSS version 14.0 (SPSS, Chicago, IL) was used to perform all the analyses.
Results
Patients
The clinical and pathological data on the melanoma patients are summarized in Table 1. Approximately one-third of the respondents were men, median age in the total group at the time of diagnosis was 50 (range, 18–77) years, median Breslow thickness was 2.0 (range, 1–13) mm, and median follow-up was 56.8 (range, 4–94) months. In the total group, 62 patients underwent inguinal SLNB (53%) and 54 axillary SLNB (47%). The mean number of sentinel lymph nodes excised was 2 (SD = 0.8).
Histopathological examination showed that 27 patients (23%) had metastases from the melanoma in the SLNB: 14 in the groin (of whom 3 had a superficial groin dissection only after the change in surgical decision making in 2002) and 13 in the axilla. These tumor-positive patients underwent CLND. The percentages of men and women were the same in the SLNB tumor-positive and tumor-negative groups. However, there were more women (50 of 62, 81%) than men (12 of 62, 19%, P < 0.001) in the inguinal SLNB group, whereas the percentages of men (30 of 54, 56%) and women (24 of 54, 44%) in the axillary SLNB group were similar (P = 0.414). Patients in the tumor-positive group were significantly older than those in the tumor-negative group. ANOVA showed a significant effect of group on age (F = 2.70, P = 0.049). Subsequent Bonferroni testing showed that the patients in the inguinal tumor-positive group were significantly older (mean = 57.5 years, SD = 11.3) than the patients in the inguinal tumor-negative group (mean = 46.3, SD = 13.9, Bonferroni P = 0.036). No significant difference in age was found between the axillary tumor-positive (mean = 49.1 years, SD = 7.9) and axillary tumor-negative groups (mean = 50.2 years, SD = 14.2).
As far as disease characteristics were concerned, no differences were found between the tumor-positive and tumor-negative groups, except for complications and incidence of lymphedema. Postoperative complications, such as wound infection, seroma, wound necrosis, or bleeding, occurred in 18 patients (16%): 9 (17%) of 54 in the axillary group and 9 (15%) of 62 in the inguinal group. Complications were statistically significantly more common in the tumor-positive group than in the tumor-negative group.
A total of 18 (16%) of the 116 patients had lymphedema: 12 (19%) of 62 in the inguinal group and 6 (11%) of 54 in the axillary group (NS). In all the cases, the lymphedema was classified as slight. In the inguinal group, lymphedema was statistically significantly more often prevalent in the tumor-positive group than in the tumor-negative group. This did not apply to the axillary group. An independent t-test showed no statistically significant difference in follow-up time between patients with or without lymphedema.
QoL, Pain, and Activities of Daily Living
Mean scores of the 116 melanoma patients on the EORTC QLQ-C30 subscales were statistically significantly higher than those in a healthy norm population from Germany. The only exception was cognitive functioning, for which the scores were similar (Table 2). Differences between the study group and the norm group in global QoL and emotional functioning were moderately clinically meaningful; in role functioning, they were small but clinically meaningful. However, in physical, cognitive, and social functioning, they were small and negligible. The QoL scores of the three patients who received a superficial groin dissection due to a change in surgical decision making in 2002 fell within the range of the total group.
ANOVA showed a significant effect of group on role functioning (P = 0.021) and tendencies toward physical functioning problems (P = 0.051) and fatigue (P = 0.051, Table 3). The post hoc Bonferroni test showed that the axillary SLNB tumor-positive group had statistically significantly poorer scores on role functioning than the two tumor-negative groups (Table 3). With regard to the clinical relevance of the differences found between groups, it seemed that in the patients who underwent ALND after SLNB, the scores on global QoL, physical functioning, and social functioning were 5–10 points lower than those in the two tumor-negative groups. In addition, the difference in social functioning compared with the inguinal tumor-positive group was between 5 and 10 points. The difference in role functioning between the axillary tumor-positive group and the three other groups was between 10 and 20 points.
The nonparametric Kruskal-Wallis test confirmed the significant differences in physical functioning (P = 0.01) and in role functioning (P = 0.01), but not the difference in fatigue. In addition, the Kruskal-Wallis test showed significant differences in MPQ Pain Rating Index (P = 0.019) and MPQ Number of Words Chosen (P = 0.019) between the groups. The axillary tumor-positive group seemed to have more functioning problems and symptoms than the other groups.
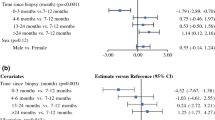
The relationship between the time elapsed since diagnosis and QoL were not statistically significant (r varied between 0.01 and 0.14).
In view of our findings that the tumor-positive and tumor-negative groups differed in age, complications, and lymphedema, combined with the fact that there were more women than men in the inguinal group than in the axillary group, we performed additional analyses to evaluate how these variables affected the outcome measures. Men had significantly higher mean scores on physical functioning (t = 3.1, P = 0.003) and the GARS (t = −3.1, P = 0.003) and a significantly lower score on fatigue (t = −2.6, P = 0.011) than the women. Age seemed to be negatively but weakly correlated with physical functioning (r = −0.29, P = 0.002) and was positively and moderately correlated with the GARS (r = 0.32, P = 0.001). The older the patient, the poorer the level of physical functioning and execution of daily activities.
Unpaired t-tests did not show any statistically significant difference in QoL, pain, and activities of daily living between patients with and without postoperative complications and the patients with and without lymphedema.
Discussion
In this study, QoL in patients with melanoma who underwent SLNB as a staging procedure, with or without CLND, was better than that in a German norm population. A possible explanation is that we investigated an exclusive group of melanoma patients with a relatively favorable prognosis who had (so far) survived their disease. In addition, the absence of important relationships between time and QoL indicates that patients, on the whole, function equally well, whether the diagnosis was relatively recent or years earlier. Other studies have also shown that QoL in cancer survivors was better than that in people who had never had cancer.3–5 Another explanation for the high QoL reported in this study might be a shift in how the patients appreciated and estimated their health status, the so-called response shift.34,35 Despite possible persistent treatment-related symptoms, patients judged their QoL relative to their own QoL while they were still undergoing treatment, resulting in even higher scores than that of people who had never been confronted with a life-threatening illness.36
Even though the differences between the melanoma patients and the norm group were statistically significant, with the exception of cognitive functioning, if we look at the clinical relevance of those differences, then only the differences in global QoL and emotional functioning were clinically meaningful.
It was striking that these melanoma patients reported less fatigue than the norm group because fatigue is a common and long-term complaint in cancer patients. An explanation might be that most of this group of melanoma patients had undergone a relatively small surgical intervention, without adjuvant chemotherapy or radiotherapy. It seemed that fatigue was highest in the group of patients after SLNB followed by completion ALND.
Our results did not confirm the hypothesis that patients in the CLND group, particularly those who had undergone groin dissection, would have more problems with QoL than those in the group with SLNB alone. Statistically significant differences or tendencies toward more problems were found in physical functioning, role functioning, fatigue, and pain. In clinical terms, meaningful differences were also present in global QoL and social functioning. However, it was not the patients with groin dissections (an intervention that is known to be associated with complications) who reported the most problems, but the patients who underwent ALND.25,37–41
Postoperative complications could not explain the higher prevalence of problems in the axillary tumor-positive group. Complications did not occur more frequently in the patients who underwent ALND than in the patients with inguinal lymph node dissection, even though complications were more common in the patients whose SLNB had been followed by dissection.
An explanation for this result might lie in the demographic or disease-related variables analyzed in this study. Sex could not explain the finding of more problems in the axillary tumor-positive group. In agreement with the literature, women with a melanoma reported more problems than men.30 However, the percentage of female patients in the axillary tumor-positive and tumor-negative groups was the same. In relation to age, we found that older patients reported more problems with physical functioning and daily activities. It should be borne in mind that the inguinal tumor-positive group, and not the axillary tumor-positive group, contained a higher proportion of older patients.
To our knowledge, this is the first study that compared QoL between melanoma patients and a group of people from the normal population and that mapped differences between patients with and without axillary or inguinal lymph node dissection after SLNB. It is important to note that our group of melanoma patients did not have any evidence of disease at the time of this study. Several of the groups had small numbers, particularly the tumor-positive SLNB groups. If the groups had been larger, the study would have had more power, and more of the differences may have been statistically significant. Furthermore, this was a cross-sectional study with wide variation in follow-up duration. However, the duration of follow-up did not seem to be correlated with QoL.
It can be concluded that the procedure of SLNB in the axilla or groin in patients with a melanoma did not have any negative effects on QoL. Our patients even reported better QoL than the norm population. Patients with CLND in the axilla after axillary SLNB had more problems than those who underwent SLNB alone in the axilla or groin. The clinical relevance of the differences found in this study varied from moderate to small. On the basis of the insights gained from this study, physicians and nurses provide better information to melanoma patients, in particular to patients who will receive an ALND after tumor-positive SLNB, on QoL consequences of staging and treatment, thus allowing better informed decision making.
References
Ganz PA. Monitoring the physical health of cancer survivors: a survivorship-focused medical history. J Clin Oncol. 2006;24:5105–11.
Stanton AL. Psychosocial concerns and interventions for cancer survivors. J Clin Oncol. 2006;24:5132–7.
Joly F, Heron JF, Kalusinski L, et al. Quality of life in long-term survivors of testicular cancer: a population-based case-control study. J Clin Oncol. 2002;20:73–80.
Ganz PA, Desmond KA, Leedham B, et al. Quality of life in long-term, disease-free survivors of breast cancer: a follow-up study. J Natl Cancer Inst. 2002;94:39–49.
Fredette SL. Breast cancer survivors: concerns and coping. Cancer Nurs. 1995;18:35–46.
Noorda EM, van Kreij RH, Vrouenraets BC, et al. The health-related quality of life of long-term survivors of melanoma treated with isolated limb perfusion. Eur J Surg Oncol. 2007;33:776–82.
Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg. 1992;127:392–9.
Morton DL, Cochran AJ, Thompson JF, et al. Sentinel node biopsy for early-stage melanoma: accuracy and morbidity in MSLT-I, an international multicenter trial. Ann Surg. 2005;242:302–11.
Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N Engl J Med. 2006;355:1307–17.
National Cancer Institute. MSLT-II protocol. 2007. Available at: http://clinicaltrials.gov/ct/show/NCT00297895. Accessed 21 July 2009.
Schijven MP, Vingerhoets AJ, Rutten HJ, et al. Comparison of morbidity between axillary lymph node dissection and sentinel node biopsy. Eur J Surg Oncol. 2003;29:341–50.
Schrenk P, Rieger R, Shamiyeh A, Wayand W. Morbidity following sentinel lymph node biopsy versus axillary lymph node dissection for patients with breast carcinoma. Cancer. 2000;88:608–14.
Purushotham AD, Upponi S, Klevesath MB, et al. Morbidity after sentinel lymph node biopsy in primary breast cancer: results from a randomized controlled trial. J Clin Oncol. 2005;23:4312–21.
Olson JA Jr, McCall LM, Beitsch P, et al. Impact of immediate versus delayed axillary node dissection on surgical outcomes in breast cancer patients with positive sentinel nodes: results from American College of Surgeons Oncology Group Trials Z0010 and Z0011. J Clin Oncol. 2008;26:3530–5.
Peintinger F, Reitsamer R, Stranzl H, Ralph G. Comparison of quality of life and arm complaints after axillary lymph node dissection vs sentinel lymph node biopsy in breast cancer patients. Br J Cancer. 2003;89:648–52.
Kootstra J, Hoekstra-Weebers JE, Rietman H, et al. Quality of life after sentinel lymph node biopsy or axillary lymph node dissection in stage I/II breast cancer patients: a prospective longitudinal study. Ann Surg Oncol. 2008;15:2533–41.
Del Bianco P, Zavagno G, Burelli P, et al. Morbidity comparison of sentinel lymph node biopsy versus conventional axillary lymph node dissection for breast cancer patients: results of the Sentinella-GIVOM Italian randomised clinical trial. Eur J Surg Oncol. 2008;34:508–13.
Rietman JS, Geertzen JH, Hoekstra HJ, et al. Long term treatment related upper limb morbidity and quality of life after sentinel lymph node biopsy for stage I or II breast cancer. Eur J Surg Oncol. 2006;32:148–52.
Dabakuyo TS, Fraisse J, Causeret S, et al. A multicenter cohort study to compare quality of life in breast cancer patients according to sentinel lymph node biopsy or axillary lymph node dissection. Ann Oncol. May 25, 2009 [Epub ahead of print].
Wrightson WR, Wong SL, Edwards MJ, et al. Complications associated with sentinel lymph node biopsy for melanoma. Ann Surg Oncol. 2003;10:676–80.
Wasserberg N, Tulchinsky H, Schachter J, Feinmesser M, Gutman H. Sentinel-lymph-node biopsy (SLNB) for melanoma is not complication-free. Eur J Surg Oncol. 2004;30:851–6.
de Vries M, Vonkeman WG, van Ginkel RJ, Hoekstra HJ. Morbidity after axillary sentinel lymph node biopsy in patients with cutaneous melanoma. Eur J Surg Oncol. 2005;31:778–83.
de Vries M, Vonkeman WG, van Ginkel RJ, Hoekstra HJ. Morbidity after inguinal sentinel lymph node biopsy and completion lymph node dissection in patients with cutaneous melanoma. Eur J Surg Oncol. 2006;32:785–9.
Doting MH, Hoekstra HJ, Plukker JT, et al. Is sentinel node biopsy beneficial in melanoma patients? A report on 200 patients with cutaneous melanoma. Eur J Surg Oncol. 2002;28:673–8.
Baas PC, Schraffordt KH, Hoekstra HJ, et al. Groin dissection in the treatment of lower-extremity melanoma. Short-term and long-term morbidity. Arch Surg. 1992;127:281–6.
Kissin MW, Querci della RG, Easton D, Westbury G. Risk of lymphoedema following the treatment of breast cancer. Br J Surg. 1986;73:580–4.
Stillwell GK. Treatment of postmastectomy lymphedema. Mod Treat. 1969;6:396–412.
Aaronson NK, Ahmedzai S, Bergman B, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85:365–76.
Osoba D, Rodrigues G, Myles J, Zee B, Pater J. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol. 1998;16:139–44.
Schwarz R, Hinz A. Reference data for the quality of life questionnaire EORTC QLQ-C30 in the general German population. Eur J Cancer. 2001;37:1345–51.
van der Kloot WA, Oostendorp RA, van der MJ, van den HJ. [The Dutch version of the McGill Pain Questionnaire: a reliable pain questionnaire]. Ned Tijdschr Geneeskd. 1995;139:669–73.
Kempen GI, Miedema I, Ormel J, Molenaar W. The assessment of disability with the Groningen Activity Restriction Scale. Conceptual framework and psychometric properties. Soc Sci Med. 1996;43:1601–10.
Suurmeijer TP, Doeglas DM, Moum T, et al. The Groningen Activity Restriction Scale for measuring disability: its utility in international comparisons. Am J Public Health. 1994;84:1270–3.
Sprangers MA. Quality-of-life assessment in oncology. Achievements and challenges. Acta Oncol. 2002;41:229–37.
Schwartz CE, Sprangers MA. An introduction to quality of life assessment in oncology: the value of measuring patient-reported outcomes. Am J Manag Care. 2002;8:S550–9.
Schwartz CE, Sprangers MA. Methodological approaches for assessing response shift in longitudinal health-related quality-of-life research. Soc Sci Med. 1999;48:1531–48.
Karakousis CP, Driscoll DL. Groin dissection in malignant melanoma. Br J Surg. 1994;81:1771–4.
Karakousis CP. Surgical procedures and lymphedema of the upper and lower extremity. J Surg Oncol. 2006;93:87–91.
Beitsch P, Balch C. Operative morbidity and risk factor assessment in melanoma patients undergoing inguinal lymph node dissection. Am J Surg. 1992;164:462–5.
Tonouchi H, Ohmori Y, Kobayashi M, et al. Operative morbidity associated with groin dissections. Surg Today. 2004;34:413–8.
Sabel MS, Griffith KA, Arora A, et al. Inguinal node dissection for melanoma in the era of sentinel lymph node biopsy. Surgery. 2007;141:728–35.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
de Vries, M., Hoekstra, H.J. & Hoekstra-Weebers, J.E.H.M. Quality of Life After Axillary or Groin Sentinel Lymph Node Biopsy, With or Without Completion Lymph Node Dissection, in Patients With Cutaneous Melanoma. Ann Surg Oncol 16, 2840–2847 (2009). https://doi.org/10.1245/s10434-009-0602-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-009-0602-6