
Abstract
Background
Perioperative hypotension during esophagectomy results from hypovolemia caused by a shift of extracellular fluid from the intravascular to the extravascular compartment. Fluid management is often difficult to gauge during major surgery because there are no reliable indicators of fluid status, and some patients still experience cardiorespiratory instability. In this retrospective study, we evaluated stroke volume variation (SVV), calculated by using a new arterial pressure-based cardiac output measurement device, as a predictor for fluid responsiveness after esophageal surgery.
Methods
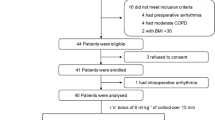
Eighteen patients undergoing esophagectomy with extended radical lymphadenectomy were monitored by the FloTrac sensor/Vigileo monitor system during the perioperative and immediate postoperative period. Fluid responsiveness was assessed and compared with concurrent SVV and central venous pressure (CVP) values, and routine hemodynamic variables.
Results
Eleven of 18 patients needed additional volume loading within the first 10 postoperative hours as a result of hypotension. The maximum SVV value of fluid resuscitated patients was >15% in all cases, whereas six of seven patients without postoperative hypotension had maximum SVV values of <15%. The correlation between SVV and the development of hypotension was statistically significant (P = 0.0012). From the linear correlation analysis of hemodynamic variables influenced by additional fluid loading, SVV was significantly correlated to cardiac output (r = 0.638; P = 0.049), whereas CVP was not (P > 0.05).
Conclusion
We conclude that SVV, as displayed on the Vigileo monitor, is an accurate predictor of intravascular hypovolemia and is a useful indicator for assessing the appropriateness and timing of applying fluid for improving circulatory stability during the perioperative period after esophagectomy.




Similar content being viewed by others


References
Ando N, Ozawa S, Kitagawa Y, et al. Improvement in the results of surgical treatment of advanced squamous esophageal carcinoma during 15 consecutive years. Ann Surg 2000;232:225–32
Fujita H, Kakegawa T, Yamana H, et al. Mortality and morbidity rates, postoperative course, quality of life, and prognosis after extended radical lymphadenectomy for esophageal cancer. Comparison of three-field lymphadenectomy with two-field lymphadenectomy. Ann Surg 1995;222:654–62
Ishihara H, Nakamura H, Okawa H, et al. Comparison of initial distribution volume of glucose and intrathoracic blood volume during hemodynamically unstable states early after esophagectomy. Chest 2005;128:1713–9
Imamura M, Shimada Y, Kanda T, et al. Hemodynamic changes after resection of thoracic duct for en-bloc resection of esophageal cancer. Surg Today 1992;22:226–32
Luketich JD, Alvelo-Rivera M, Buenaventura PO, et al. Minimally invasive esophagectomy: outcomes in 222 patients. Ann Surg 2003;238:486–94
Sayama J, Shineha R, Yokota K, et al. [Control of the excessive reaction after surgery for esophageal carcinoma with preoperative administration of the cortico-steriods]. Jpn J Gasroenterol Surg 1994;81:49–51
Shimada H, Ochiai T, Okazumi S, et al. Clinical benefits of steroid therapy on surgical stress in patients with esophageal cancer. Surgery 2000;128:791–8
Kobayashi M, Harada O, Shimaya S, et al. [Experiences using neutrophil elastase inhibitors perioperatively after radical esophagectomy]. Shinyaku Rinsho 2004;53:762–5
Bartels H, Stein HJ, Siewert JR. Preoperative risk analysis and postoperative mortality of oesophagectomy for resectable oesophageal cancer. Br J Surg 1998;85:840–4
Reynolds JV, Ravi N, Hollywood D, et al. Neoadjuvant chemoradiation may increase the risk of respiratory complications and sepsis after transthoracic esophagectomy. J Thorac Cardiovasc Surg 2006;132:549–55
Michard F, Teeboul JL. Predicting fluid responsiveness in ICU patients: a critical analysis of the evidence. Chest 2002;121:2000–8
Manecke GR Jr, Auger WR. Cardiac output determination from the arterial pressure wave: clinical testing of a novel algorithm that does not require calibration. J Cardiothorac Vasc Anesth 2007;21:3–7
Reuter DA, Felbinger TW, Schmidt C, et al. Stroke volume variations for assessment of cardiac responsiveness to volume loading in mechanically ventilated patients after cardiac surgery. Intensive Care Med 2002;28:392–8
Suzuki A, Ishihara H, Okawa H, et al. Can initial distribution volume of glucose predict hypovolemic hypotension after radical surgery for esophageal cancer? Anesth Analg 2001;92:1146–51
Shippy CR, Appel PL, Shoemaker WL. Reliability of clinical monitoring to assess blood volume in critically ill patients. Crit Care Med 1984;12:107–12
Michard F. Changes in arterial pressure during mechanical ventilation. Anesthesiology 2005;103:419–28
Hofer CK, Muller SM, Furrer L, et al. Stroke volume and pulse pressure variation for prediction of fluid responsiveness in patients undergoing off-pump coronary artery bypass grafting. Chest 2005;128:848–54
Rex S, Brose S, Metzelder S, et al. Prediction of fluid responsiveness in patients during cardiac surgery. Br J Anaesth 2004;93:782–8
Tandon S, Batchelor A, Bullock R, et al. Peri-operative risk factors for acute lung injury after elective oesophagectomy. Br J Anaesth 2001;86:633–8
Acknowledgment
We thank Steve Clissold, PhD (Content Ed Net), who provided assistance with English language and whose work was funded by Edwards Lifesciences, Japan.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kobayashi, M., Koh, M., Irinoda, T. et al. Stroke Volume Variation as a Predictor of Intravascular Volume Depression and Possible Hypotension During the Early Postoperative Period After Esophagectomy. Ann Surg Oncol 16, 1371–1377 (2009). https://doi.org/10.1245/s10434-008-0139-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-008-0139-0