
Abstract
Introduction
Minimal invasive surgical approach can achieve quick functional recovery. However, the oncologic outcome for cancer is still a concern. This study aims to compare the oncologic outcome between laparoscopic and open methods in the curative resection of Stage II or III left-sided colon cancers.
Methods
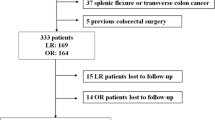
In consideration of statistical power up to 90%, 286 eligible patients with curable left-sided colon cancer (Tumor-Node-Metastasis Stage II and Stage III disease) requiring the takedown of colonic splenic flexure to facilitate a curative left hemicolectomy were recruited randomly and equally allocated to the laparoscopic and open group. The primary endpoint was time-to-recurrence of tumor. Data was analyzed according to intention-to-treat principle.
Results
Postrandomization exclusion occurred because of metastatic disease detected intraoperatively occurred in 13 patients and because of patient withdrawal from trial in 4. Therefore, 135 and 134 patients actually comprised the laparoscopic and open group, respectively. The median follow-up of patient was 40 months (range: 18–72 months). The oncologic results were similar (P = 0.362, one-sided log-rank test) in laparoscopic and open group of patients, with the estimated cumulative recurrence rate of 13.2% (9/68) versus 17.2% (11/64) in Stage II disease and 20.9% (14/67) versus 25.7% (18/70) in Stage III disease, respectively. The recurrence patterns were similar between the two groups. Both open and laparoscopic groups were comparable in the number of dissected lymph node (15.6 ± 3.0 vs. 16.0 ± 6.0, P = 0.489), various demographic and clinicopathologic parameters.
Conclusions
The estimated cumulative recurrence rate for the surgery of Stage II or III left-sided colon cancers was the same between laparoscopic and open methods.


Similar content being viewed by others


References
Nelson H, Sargent DJ, Wieand HS, et al. A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 2004; 350:2050–2059
Leung KL, Kwok SPY, Lam SCW, et al. Laparoscopic resection of rectosigmoid carcinoma: prospective randomized trial. Lancet 2004; 363:1187–1192
Guillou P, Quirke P, Thorpe H, et al. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomized controlled trial. Lancet 2005; 365:1718–1726 and 1666–1668
Lacy AM, Carcia-Valdecasas JC, Delgado S, et al. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomized trial. Lancet 2002; 359:2224–2229
Yamamoto S, Watanabe M, Hasegawa H, et al. Oncologic outcome of laparoscopic versus open surgery for advanced colorectal cancer. Hepatogastroenterology 2001; 48:1248–1251
Beart R, Kehlet H, Buechler M, et al. International trends in abdominal surgery: laparotomy compared with laparoscopy. Dis Colon Rectum 2004; 47:623
Delaney CP, Kiran RP, Senagore AJ, et al. Case-matched comparison of clinical and financial outcome after laparoscopic and open colorectal surgery. Ann Surg 2003; 238:67–72
Liang JT, Shieh MJ, Chen CN, et al. Prospective evaluation of laparoscopy-assisted colectomy versus laparotomy with resection in the management of complex polyps of the sigmoid colon. World J Surg 2002; 26:377–383
Liang JT, Lai HS, Huang KC, et al. Comparison of medial-to-lateral versus traditional lateral-to-medial dissection sequences for the resection of rectosigmoid cancers—a randomized controlled clinical trial. World J Surg 2003; 27:190–196
Liang JT. Comparison of medial-to-lateral versus traditional lateral-to-medial dissection sequences for the resection of rectosigmoid cancers (letter, comment). World J Surg 2003; 27:1337–1338
Milsom JW, Böhm B. Laparoscopic colorectal surgery. New York: Springer-Verlag; 1996
Milsom JW, Böhm B, Hammerhofer KA, et al. A prospective, randomized trial comparing laparoscopic versus conventional techniques in colorectal cancer surgery: a preliminary report. J Am Coll Surg 1998; 187:46–57
Liang JT, Lai HS, Lee PH. Laparoscopic medial-to-lateral approach for the curative left hemicolectomy. Dis Colon Rectum 2005; 48:2142–2143
Japanese Society for Cancer of the Colon and Rectum. General Rules for Clinical and Pathological Studies on Cancer of the Colon, Rectum, and Anus. Tokyo: Kanehara, 1994
Turnbull RB, Kyle K, Watson FR, et al. Cancer of the colon: the influence of the no-touch technique on survival rates. Ann Surg 1967; 166:420–427
McLeod RS. Issues in surgical randomized controlled trials. World J Surg 1999; 23:1210–1214
Holm T, Johansson H, Cedermark B, et al. Influence of hospital and surgeon related factors and outcome after treatment of rectal cancer with or without preoperative radiotherapy. Br J Surg 1997; 87:657–663
Parry JM, Collins S, Mathers J, et al. Influence of volume of work on the outcome of treatment for patients with colorectal cancer. Br J Surg 1998; 86:475–481
Kao LS, Aaron BC, Dellinger EP. Trials and tribulations: current challenges in conducting clinical trials. Arch Surg 2003; 138:59–62
Lilford R, Braunholtz D, Harris J, et al. Trials in surgery. Br J Surg 2004; 91:6–16
Weeks JC, Nelson H, Gelber S, Sargent D, Schroeder G. Clinical Outcomes of Surgical Therapy (COST) Study Group: Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: a randomized trial. JAMA 2002; 287:321–328
Iacopetta B. Are there two sides to colorectal cancer? Int J Cancer 2002; 101:403–408
Nishiguchi K, Okuda J, Toyoda M, et al. Comparative evaluation of surgical stress of laparoscopic and open surgeries for colorectal carcinoma. Dis Colon Rectum 2001; 44:223–230
Liang JT, Huang KC, Jeng YM, Lee PH, Lai HS, Hsu HC. Microvessel density, cyclo-oxygenase 2 expression, K-ras mutation and p53 overexpression in colonic cancer. Br J Surg 2004; 91:355–361
Sargent DJ, Wieand HS, Haller DG, et al. Disease-free survival versus overall survival as a primary end point for adjuvant colon cancer studies: individual patient data from 20,898 patients on 18 randomized trials. J Clin Oncol 2005; 23:8664–8670
Wexner SD, Cohen SM. Port site metastases after laparoscopic colorectal surgery for cure of malignancy. Br J Surg 1995; 82:295–298
Bouvy ND, Marquet RL, Jeekel J, Bonjer HJ. Laparoscopic surgery is associated with less tumour growth stimulation than conventional surgery: an experimental study. Br J Surg 1997; 84:358–361
Hubens G, Pauwels M, Hubens A, Vermeulen P, Van Marck E, Eyskens E. The influence of a pneumoperitoneum on the peritoneal implantation of free intraperitoneal colon cancer cells. Surg Endosc 1996; 10:809–812
Kim SH, Milsom JW, Gramlich TL, et al. Does laparoscopic vs. conventional surgery increase exfoliated cancer cells in the peritoneal cavity during resection of colorectal cancer? Dis Colon Rectum 1998; 41:971–978
Hsu TC. Feasibility of colectomy with mini-incision. Am J Surg 2005; 190:48–50
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Liang, JT., Huang, KC., Lai, HS. et al. Oncologic Results of Laparoscopic Versus Conventional Open Surgery for Stage II or III Left-Sided Colon Cancers: A Randomized Controlled Trial. Ann Surg Oncol 14, 109–117 (2007). https://doi.org/10.1245/s10434-006-9135-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-006-9135-4