
Abstract
Background
We evaluated the necessity of a tumor bed boost after whole-breast radiotherapy for early-stage breast cancer after breast-conserving surgery and negative re-excision.
Methods
Of patients treated at the Virginia Commonwealth and Tufts Universities with breast-conservation therapy for early-stage breast cancer between 1983 and 1999, 205 required re-excision of the tumor cavity to obtain clear margins and were found to be without residual disease. Adjuvant conventionally fractionated whole-breast radiotherapy was given to a total dose of 50 Gy in 25 fractions. The tumor bed boost was omitted.
Results
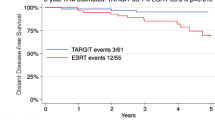
The median follow-up was 98 months (range, 6–229 months). The tumor histological diagnosis was primarily infiltrating ductal carcinoma (183 cases; 89%). Nodal involvement was documented in 49 cases (24%). There were four documented recurrences at the tumor bed site. Five in-breast recurrences were documented to be in a location removed from the tumor bed. The overall Kaplan-Meier 15-year in-breast control rate was 92.4%, and the freedom from true recurrence rate was 97.6%.
Conclusions
The findings support the concept that postlumpectomy radiotherapy can be tailored according to the degree of surgical resection. There is an easily identifiable subgroup of patients who can avoid a tumor bed boost, thus resulting in a reduced treatment time and improved cosmesis, while maintaining local control rates that approach 100%. The data suggest that in patients who undergo a negative re-excision, treatment with whole-breast radiotherapy to 50 Gy is a sufficient dose to maximally reduce the risk of local recurrence.
Similar content being viewed by others


References
Veronesi U, Marubini E, Mariani L, et al. Radiotherapy after breast-conserving surgery in small breast carcinoma: long-term results of a randomized trial. Ann Oncol 2001; 12:997–1003
Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of randomized study comparing breast-conserving surgery with radical (Halstead) mastectomy for early breast cancer. N Engl J Med 2002; 347:1227–32
Clark RM, McCulloch PB, Levine MN, et al. Randomized clinical trial to assess the effectiveness of breast irradiation following lumpectomy and axillary dissection for node-negative breast cancer. J Natl Cancer Inst 1992; 84:683–9
Uppsala-Oreboro Breast Cancer Study Group. Sector resection with or without postoperative radiotherapy for stage I breast cancer: a randomized trial. J Natl Cancer Inst 1990; 82:277–82
Recht A, Silver B, Schnitt S, et al. Breast relapse following primary radiation therapy for early breast cancer. I. Classification, frequency and salvage. Int J Radiat Oncol Biol Phys 1985; 11:1271–6
Smith TE, Daesung L, Turner BC, et al. True recurrence vs. new primary ipsilateral breast tumor relapse: an analysis of clinical and pathologic differences and their implications in natural history, prognoses, and therapeutic management. Int J Radiat Oncol Biol Phys 2000; 48:1281–9
Obedian E, Fischer DB, Haffty BG. Second malignancies after treatment of early-stage breast cancer: lumpectomy and radiation therapy versus mastectomy. J Clin Oncol 2000; 18:2406–12
Fisher B, Anderson S. Conservative surgery for the management of invasive and noninvasive carcinoma of the breast: NSABP trials. World J Surg 1994; 18:63–9
Fisher ER, Dignam J, Tan-Chiu E, et al. Pathologic findings from the National Surgical Adjuvant Breast Project (NSABP) eight-year update of protocol B-17. Cancer 1999; 86:429–38
Holli K, Saaristo R, Isola J, et al. Lumpectomy with or without postoperative radiotherapy for breast cancer with favourable prognostic features: results of a randomized study. Br J Cancer 2001; 84:164–9
Morrow M. Rational local therapy for breast cancer. N Engl J Med 2002; 347:1270–1
Hayman JA, Hillner BE, Harris JR, et al. Cost-effectiveness of adding an electron-beam boost to tangential radiation therapy in patients with negative margins after conservative surgery for early-stage breast cancer. J Clin Oncol 2000; 18:287–95
Romestaing P, Lehinge Y, Carrie C, et al. Role of a 10-Gy boost in the conservative treatment of early breast cancer: results of a randomized clinical trial in Lyon, France. J Clin Oncol 1997; 15:963–8
Polgar C, Fodor J, Orosz Z, et al. Electron and high-dose-rate brachytherapy boost in the conservative treatment of stage I-II breast cancer: first results of the randomized Budapest boost trial. Strahlenther Onkol 2002; 178:615–23
Bartelink H, Horiot JC, Poortmans P, et al. Recurrence rates after treatment of breast cancer with standard radiotherapy with or without additional radiation. N Engl J Med 2001; 345:1378–87
Schmidt-Ullrich RK, Wazer DE, Tercilla O, et al. Tumor margin assessment as a guide to optimal conservation surgery and irradiation in early stage breast carcinoma. Int J Radiat Oncol Biol Phys 1989; 17:733–8
Wazer DE, Sinesi M, Schmidt-Ullrich RK, et al. Importance of surgical and pathologic determinants of tumor margin status for breast conservation therapy. Breast Dis 1991; 4:285–92
Schmidt-Ullrich RK, Wazer DE, DiPetrillo T, et al. Breast conservation therapy for early stage breast carcinoma with outstanding 10-year locoregional control rates: a case for aggressive therapy to the tumor bearing quadrant. Int J Radiat Oncol Biol Phys 1993; 27:545–52
Wazer DE, Schmidt-Ullrich RK, Schmid CH, et al. The value of breast lumpectomy margin assessment as a predictor of residual tumor burden. Int J Radiat Oncol Biol Phys 1997; 38:291–9
Wazer DE, Schmidt-Ullrich RK, Ruthazer R, et al. Factors determining outcome for breast-conserving irradiation with margin-directed dose escalation to the tumor bed. Int J Radiat Oncol Biol Phys 1998; 40:851–8
Neuschatz AC, DiPetrillo T, Safaii H, et al. Long-term follow-up of a prospective policy of margin-directed radiation dose escalation in breast-conserving therapy. Cancer 2003; 97:30–9
Marubini E, Valsecchi M. Analysing Survival Data From Clinical Trials and Observational Studies. Chichester: Wiley, 1995
Recht A, Harris JR. To boost or not to boost, and how to do it. Int J Radiat Oncol Biol Phys 1991; 20:177–8
Pezner RD. Cosmetic breast fibrosis: it’s the local boost! Int J Radiat Oncol Biol Phys 1994; 30:1251–2
Regine WF, Kramer CA. To boost or not to boost?...it’s not the only question! In response to Pezner, Int J Radiat Oncol Biol Phys 30:1251–2; 1994. Int J Radiat Oncol Biol Phys 1995; 32:273–7
Fischer B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 2002; 347:1233–41
Fischer B, Bower M, Margolese R, et al. Five year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med 1985; 312:665–73
Vrieling C, Collette L, Fourquet A, et al. The influence of the boost in breast-conserving therapy on cosmetic outcome in the EORTC “boost versus no boost” trial. Int J Radiat Oncol Biol Phys 1999; 45:677–85
Vrieling C, Collette L, Fourquet A, et al. The influence of patient, tumor and treatment factors on the cosmetic results after breast-conserving therapy in the EORTC “boost vs no boost” trial. Radiother Oncol 2000; 55:219–32
Pezner RD, Wagman LD, Ben-Ezra J, et al. Breast conservation therapy: local tumor control in patients with pathologically clear margins who receive 5000cGy breast irradiation without local boost. Breast Cancer Res Treat 1994; 32:261–7
Gelman R, Gelber R, Henderson IC, et al. Improving methodology for analyzing local and distant recurrence. J Clin Oncol 1990; 8:548–55
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arthur, D.W., Cuttino, L.W., Neuschatz, A.C. et al. Tumor Bed Boost Omission After Negative Re-Excision in Breast-Conservation Treatment. Ann Surg Oncol 13, 794–801 (2006). https://doi.org/10.1245/ASO.2006.04.002
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/ASO.2006.04.002