
Abstract
The consumption of non-steroidal anti-inflammatory drugs (NSAIDs) have increased lately around the world, as they are considered essential and popular drugs for effective reduction of pain and inflammation. They have analgesic, antipyretic, and anti-inflammatory activities; also, it was reported recently that they protect against various critical disorders like heart attacks and cancer. However, oral use of NSAIDs may cause several pulmonary, gastrointestinal, hepatic, cardiovascular, cerebral, and renal complications. Therefore, topical NSAIDs were recommended as a substitute to oral NSAIDs for the treatment of inflammation and pain. Still, the skin permeation of NSAIDs is considered a challenge, as the skin have an effective barrier function. Therefore, this review investigates various advanced vesicular nanocarriers and their applications through the skin, to augment the topical delivery of NSAIDs through stratum corneum over the conventional systems, enhance their effectiveness, and reduce the unwanted side effects. These innovative systems can manage bioavailability, solubility, stability, safety, and efficacy issues present in conventional systems.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Inflammation is a vascular reaction done by the immune systems during tissue injury and infection which may be caused by physical or chemical agents, immunological reactions, or infection by pathogenic organisms [1]. Inflammation results in the release of fluid, dissolved substances, and cells from the circulating blood into the injured or necrotic tissue [2]. It is crucial for the maintenance of normal tissue homeostasis. As a response to injury, prostaglandins are produced causing pain, swelling, and inflammation [3]. The skin’s major prostaglandin is PGE-2 which is a possible mediator of induced COX-2 [4]. COX-2 is an induced enzyme in case of pathophysiological conditions such as inflammation [5].
Non-steroidal anti-inflammatory drugs (NSAIDs) are among the most widespread over-the-counter drugs around the world [6]. The first NSAID isolated in 1829 was salicylate, followed by indomethacin which was developed in the 1960s. Then, more than 30 compounds have been developed and brought to market [7]. Various types of NSAIDs are listed by chemical class in Fig. 1. The beneficial activities of NSAIDs are produced through COX enzymes’ inhibition. Their anti-inflammatory effect is caused by the inhibition of COX-2, while the inhibition effect of COX-1 causes undesirable side effects. NSAIDs are widely favored because of their strong efficacy, extended history of clinical use, and low abuse potential [8]. They have anti-inflammatory, analgesic, and antipyretic activities [9]. NSAIDs treat mild to moderate pain accompanied by different acute and chronic inflammations, for example, osteoarthritis, neck pain, low back pain, headache, rheumatoid arthritis, gout, and dysmenorrhea. Generally, they are favored over opioids because of their established effectiveness and limited possibility for abuse [10].

Classification of NSAIDs. NSAIDs, non-steroidal anti-inflammatory drugs
The utilization of topical NSAIDs provides improved local delivery of the drug to injured tissues with a low occurrence of undesirable side effects associated with oral therapy [11], such as gastrointestinal irritation, effects on water and electrolyte balance, cardiovascular side effects [12], hepatotoxicity [13], nephrotoxicity, and eventually renal failure [14]. Therefore, topical NSAIDs were recommended as an alternative to oral NSAIDs for the management of pain and inflammation [15]. Direct skin application of medications is either intended for local or systemic effects and is usually formulated as topical patches, ointments, gels, creams, solutions, etc. [16]. However, despite the advantages of topical drug delivery, drugs must have certain characteristics to be effectively delivered in topical form. Firstly, drugs must have lipophilic nature to be released slowly through the stratum corneum reaching deep skin layers. This helps achieving high therapeutic concentration in the site of action and providing extended pharmacological effect [17]. Also, molecular weight is an important consideration for efficient topical drug delivery, as a molecular weight of < 500 daltons are considered perfect for passing through the skin barrier [18]. Improving topical drug delivery can be done by accumulating between corneocytes, passing into a shunt such as a hair follicle, merging with skin lipids, or discomposing and integrating with lipidic layers [19].
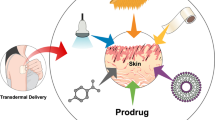
Studies showed that the penetration of NSAIDs through the skin into the blood occurs in small amounts and slowly, as topical NSAIDs’ bioavailability and maximal plasma concentration are mostly < 5 and 15%, respectively, in comparison with equivalent oral dose [11]. This provoked the necessity to develop vesicular systems for augmenting the delivery of NSAIDs through the skin to decrease the drawbacks associated with oral therapy and improve their efficacy (Fig. 2) [20].

Graphical illustration of permeation mechanism of nanovesicles across the skin
Vesicular Drug Delivery Systems
Vesicles are particles prepared using amphoteric molecules such as surfactants or phospholipids surrounding an aqueous phase creating colloids of one or more concentric lipid bilayers [21]. Vesicles can encapsulate both lipophilic or hydrophilic drugs in the lipid bilayer or the aqueous core, respectively [22]. They have the ability to deliver drugs to the targeted action site, thus decreasing the risk of drug toxicity [23]. Furthermore, vesicular delivery systems have confirmed superiority over conventional systems [24]. It was confirmed that vesicles can enhance the skin penetration of anti-inflammatory drugs as their lipidic components are able to permeate and modify the stratum corneum lipid matrix [19]. Also, vesicular systems improve the characteristics of topical formulas in the micro- or nanometer size range.
Liposomes and niosomes are considered the oldest discovered vesicles [25]; however, they have some limitations due to their low physical stability which may lead to aggregation, leakage, and drugs’ fusion, which limit their practicality and efficiency [26]. To overcome these limitations, several advanced vesicular systems have been used recently [27]. Yet these systems have some challenges, as some of them may sometimes cause skin irritation such as proniosomes, ethosomes, and transethosomes. Long term stability is also a challenge that may occur with emulsomes [21], pharmacosomes [23], and cubosomes. Also, natural phospholipids have low purity which is considered a challenge in preparing phospholipids containing vesicles such as transferosomes and cerosomes [23]. Table I presents the advantages and limitations of different vesicular systems. In our review, facts and several applications of innovative vesicular carriers for the delivery of NSAIDs through the skin will be discussed, as demonstrated in Table II.
Proniosomes
Proniosomes are dry surfactant-based vesicular carriers [28]. When compared with conventional niosomes, proniosomes are more identical in size, more stable, more economical, and easier to store and handle [55]. They overcome physical problems, for example, sedimentation, aggregation, entrapped drugs’ dripping, and fusion upon storage [29]. Furthermore, proniosomes can integrate drug molecules with different solubilities [56]. Also, they enhance the permeation of drugs through the skin due to the presence of surfactants, as they act as penetration enhancers that interact with the stratum corneum lipophilic barrier [57]. However, proniosomes have some limitations as the large particle-size drugs are not easily absorbed through the skin. Also, proniosomes may sometimes cause skin irritation. Proniosomes structure is presented in Fig. 3.

Schematic diagram represents the structure of proniosomes, emulsomes, pharmacosomes, transferosomes, ethosomes, and transethosomes
Shah et al. formulated naproxen-loaded proniosomes to compare the delivery of naproxen proniosomes through the transdermal route with oral therapy [20]. Proniosomes were prepared using a coacervation-phase separation process. The drug content, type, and amount of surfactant, lecithin, and cholesterol quantities were investigated to select the optimum formula. Different types of Span and Tween were used as penetration enhancers. The optimum proniosomal formula showed the highest entrapment efficiency and stability, with superior transdermal flux than other formulas. Also, the in vivo results confirmed that the anti-inflammatory efficacy of naproxen transdermal proniosomes was equal to the oral naproxen tablets present in the market. Generally, the results suggested that transdermal delivery of naproxen-loaded proniosomes is a reasonable alternative for oral naproxen delivery for avoiding gastric side effects such as ulceration, bleeding, and perforation.
Ammar et al.’s objective was the formulation of tenoxicam-loaded proniosomes for the management of rheumatic diseases, transdermally [39]. The coacervation phase separation technique was employed to prepare proniosomes using cholesterol, different types of surfactants, and phospholipids. Different types of Span and Tween were used as penetration enhancers. The prepared proniosomal formulas showed spherical vesicular structure under light microscopy, high entrapment efficiency, good stability profile, and in vitro release efficiency. The ex vivo skin permeability study was done for the optimum formula and revealed high permeation of tenoxicam across the skin. Moreover, the in vivo behavior of the optimum formula was evaluated on rats versus the oral product present in the market. The inspected proniosomes’ formula had significantly higher analgesic and anti-inflammatory effects than the oral commercial tenoxicam tablets. Thus, proniosomes’ vesicles offer a useful system for transdermal drug delivery.
Also, a study by Wen et al. aimed to improve mefenamic acid transdermal delivery through the preparation of proniosomes [40]. Several factors were investigated to optimize the proniosomes’ formulas. The preparation method used was coacervation phase separation using lecithin with cholesterol and different types of non-ionic surfactants. Span 60, Span 80, and Brij®52 were used as penetration enhancers. The formulas were prepared and then converted to gel. The optimum proniosomal gel had the highest entrapment efficiency, in vitro release profile, and superior skin permeation. The in vivo anti-inflammatory effect of the optimum formula was assessed using a formalin-induced rat paw edema model and resulted in a significantly higher inhibition of edema in comparison with the control. The study confirmed that proniosomes are safe vesicular carriers to improve mefenamic acid transdermal delivery.
Emulsomes
Emulsomes are a unique vesicular system with a fatty solid inner core formed of fats and triglycerides enclosed by a phospholipid bilayer, as shown in Fig. 3. They become stable by adding high concentrations of cholesterol and lecithin [58]. Emulsomes are biocompatible vesicles, with the features of both liposomes and emulsions [59]. They provide a better chance to load high concentrations of lipophilic drugs with a controlled release profile, and also, they can entrap water-soluble drugs in the aqueous parts surrounding the phospholipids layers [60]. Moreover, emulsomes’ composition plays a significant role in vesicle-skin interactions giving them a permeation-enhancing effect caused by the phospholipid bilayer adsorption at the stratum corneum-suspension interface. Emulsomes limitations include limited drug loading capacity and low stability due to high oil concentration.
Kommana and Babu formulated soya lecithin-based emulsomes for the evaluation of these vesicles for topical administration of lornoxicam [41]. Lornoxicam-loaded emulsomes were prepared by applying two methods: thin film hydration then high-speed homogenization. Emulsomes were formulated using cholesterol, butylated hydroxytoluene, oleic acid, and sodium deoxycholate, with different concentrations of glyceryl behenate and soya lecithin. Different concentrations of soya lecithin and glyceryl behenate were used to enhance the permeation of the drug through the skin by forming the phospholipid bilayer. The optimum emulsomes formula had a small particle size, high stability, and high entrapment efficiency. Also, it had a sustained release profile of 88.81% ± 0.46 at 72 h. Based on the study, emulsomes are considered a promising system for the effective management of pain related to joint inflammation.
Pharmacosomes
Pharmacosomes are lipidic amphiphilic vesicles composed of phospholipid complexes, which increase the bioavailability of drugs with poor water-solubility characteristics (Fig. 3) [61]. They are highly stable and suitable for incorporating high concentrations of lipophilic and hydrophilic drugs. Pharmacosomes can directly deliver the drug to the site of infection. Also, they enhance drug penetration across the skin because of their capacity to interact with the skin membrane, due to their transitions from vesicle to micelle by altering the transition temperature [62]. They were prepared for various proteins, antineoplastics, cardiovascular drugs, and NSAIDs [63]. There are some limitations of the pharmacosomes, such as drug leakage which requires a covalent bond to be avoided, low long-term stability, and amphiphilic nature is essential for the synthesis of the compound.
Kaur et al.’s aim was to prepare mefenamic acid-loaded pharmacosomes for the topical treatment of menstrual pain [42]. The hand shaking method was applied to formulate mefenamic acid-loaded pharmacosomes using different concentrations of cholesterol and soya lecithin. The prepared mefenamic acid pharmacosomes penetrated the lipoidal structure easily and produced a prolonged action. The drug was used in the topical treatment of menorrhagia and other gynecological disorders to avoid complications associated with oral administration.
Transferosomes
Transferosomes were presented in the 1990s by Cevc et al.; they are biocompatible and biodegradable vesicular carriers [64]. Transferosomes structure consists of an edge activator and phospholipids [65], as shown in Fig. 3. The edge activator provides ultra-deformable characteristics to the vesicles called self-optimizing deformability, which gives the transferosomes the ability to alter their flexibility and permit through the pores of the skin [66]. Moreover, the improved drug delivery of transferosomes is caused by the force offered by the osmotic gradient that exists between the stratum corneum’s outer and inner layers, which allows them to cross the intact skin by the effect of the natural transcutaneous hydration gradient. Transferosomes are accumulated easily inside the leaky synovial tissue causing peripheral targeting. Also, they act as depots which results in forming a controlled drug delivery system [67]. However, transferosomes have a high production cost and low chemical stability. Also, natural phospholipids may have low purity. Diractin® is a market application of transferosomes containing ketoprofen indicated for pain management in knee osteoarthritis. Despite the good clinical efficacy and high outcome of the market formula, it was removed from the market for its high cost [68].
A study done by Tawfeek et al. involved the formulation of a transferosomal gel using lornoxicam for the effective treatment of different skin inflammatory conditions [43]. Lornoxicam transferosomes were formulated by a thin film hydration technique using phosphatidylcholine with two different edge activators (sodium deoxycholate and Tween 80) which were used as penetration enhancers. They had high entrapment efficiency and drug loading, low vesicle size, high stability, and uniform spherical morphology. The selected lornoxicam-loaded transferosomal hydrogel showed high drug permeation through rat skin. Also, it showed higher anti-inflammatory activity than lornoxicam hydrogel and indomethacin gel as a standard NSAID. Results proved that lornoxicam transfersomal hydrogel is an effective preparation for the topical management of local inflammatory conditions.
Another study done by Shaji and Lal involved the encapsulation of piroxicam into transferosomes aimed to improve the drug’s permeation through the skin [44]. The thin film hydration method and Design-Expert® software were used to prepare and optimize piroxicam-loaded transferosomes, respectively. A full 32 factorial design was used by varying amounts of the drug and edge activator. Tween 80, Span 80, Span 65, and sodium deoxycholate were used as edge activators to enhance drug penetration through the skin. The selected formula was put into transferosomal gel and revealed a significantly higher collective drug permeation and flux when compared with the drug solution and conventional gel. Also, the pharmacodynamics study indicated that the transfersomal gel had better anti-inflammatory activity than the conventional gel. In brief, piroxicam transfersomal gel is a reasonable promising system for transdermal application.
Ethosomes
Ethosomes are hydroalcoholic phospholipids containing vesicular carriers [69]. They may be prepared using different phospholipids like hydrogenated phosphatidylcholine, phosphatidylethanolamine, phosphatidylserine, phosphatidylglycerol, phosphatidic acid, phosphatidylinositol, phosphatidylcholine, alcohol, water, and propylene glycol [30]. Ethosomes can penetrate human skin, which is caused by the presence of ethanol in their structure. Ethanol can increase the solubility of poorly soluble drugs and alter the barrier properties of the stratum corneum increasing thermodynamic activity due to ethanol evaporation [46], which increases their ability to carry different types of drugs across the skin barrier efficiently [31]. However, ethanol present in ethosomes may cause skin irritation or dermatitis. Also, there is a risk of aggregation and precipitation of the formulated vesicles. Ethosomes’ structure is presented in Fig. 3.
Chourasia et al. studied ethosomes for the delivery of ketoprofen via skin [45].
Ethosomes were prepared using different soya phosphatidylcholine and ethanol concentrations to enhance the penetration of the drug through the skin. The prepared ethosomes formulas had unilamellar spherical shapes with high entrapment efficiency and acceptable low particle sizes. They had a sustained release profile of the drug compared to the hydroethanolic drug solution. Also, in vitro ketoprofen permeability through human skin exhibited an improved permeation of the drug and transdermal flux with ethosomes over hydroalcoholic drug solution. The results of the study revealed that ethosomes vesicles are a possibly valuable transdermal system for the delivery of ketoprofen.
Also, indomethacin-loaded ethosomes were formulated by Sakdiset et al. applying a thin film hydration method using various concentrations of soybean phosphatidylcholine and ethanol (as a penetration enhancer) [46]. The formulated ethosomes had good colloidal appearance, entrapment efficiency, and size. The optimum ethosomal formula had significantly higher drug permeation across pig skin than the market solution and the alcoholic indomethacin solution over 24 h. The formula showed high stability regarding drug content, physical appearance, and encapsulation efficiency after storage at room temperature for 90 days. These outcomes recommended ethosomes as a good drug carrier for effective transdermal delivery of indomethacin.
Transethosomes
Transethosomes are ethosomes with an additional penetration enhancer or edge activator (Fig. 3) [70]. Transethosomes have high flexibility, high skin permeability, and a high flux rate compared to other vesicles caused by the presence of ethanol and edge activators in their structure. They are biocompatible, stable, and bio-degradable with high patient compliance [32]. However, drug molecular size must be reasonable to encapsulate efficiently inside transethosomes. They also may cause skin irritation or dermatitis.
Boosting transdermal delivery for the treatment of musculoskeletal pain was the objective of a study done by Kaul et al. through the preparation of naproxen-loaded transethosomes [47]. An ethanol injection technique was performed to prepare transethosomes applying 32 factorial design varying the amounts of phosphatidylcholine and sodium deoxycholate, using Tween 80 as an edge activator which increased skin penetration of the drug along with ethanol. The outcomes showed that transethosomes had a spherical morphology, high entrapment efficiency, and small particle size. The in vitro skin permeability profile across rat skin displayed high skin deposition with reduced systemic absorption which is important in musculoskeletal pain relief. The in vivo studies indicated the dominance of naproxen transethosomal gel in decreasing the edema rate in experimental rats. Overall, the study revealed that transethosomes are perfect carriers for the management of musculoskeletal pain.
Garg et al. prepared piroxicam-loaded transethosomal gel for treating rheumatoid arthritis, osteoarthritis, and other inflammatory diseases [48]. Piroxicam-loaded transethosomes were formulated utilizing the thin film hydration method using soya phosphatidylcholine, Span 80, and ethanol, as Span 80 and ethanol acted as penetration enhancers. The optimum formula was selected applying Design-Expert® software, and then it was converted into a gel. The developed piroxicam transethosomal gel had superior entrapment efficiency, drug skin retention, deformability, and drug permeability over the drug-loaded liposomes, ethosomes, and transfersomes’ gels. Consequently, transethosomes can be applied successfully as a topical carrier of piroxicam.
Bilosomes
Bilosomes are lipid-based vesicles composed of bile salts and non-ionic amphiphiles, as presented in Fig. 4 [71]. Bilosomes’ structure offers high flexibility to the vesicles permitting them to squeeze and transport the drug to the action site [49]. Bilosomes are stable, scalable, and easy to prepare, with high patient compliance [33]. They also enhance skin penetration properties [34], due to the bile salt’s integral ability to form chemical compounds with the keratocytes which increase the permeation of drugs through the skin [72]. Vaccines are among the most vital applications of bilosomes [73]. However, bilosomes efficiently entrap cationic drugs more than anionic drugs due to bile salt’s negative charge.

Schematic diagram represents the structure of bilosomes, cubosomes, spanlastics, and cerosomes
Al-mahallawi et al. prepared tenoxicam-loaded bilosomes using a thin film hydration process, applying the 3122 full factorial design [49]. Bilosomes were formulated using different types of Span, different cholesterol ratios, and different concentrations of bile salt, then optimized using Design-Expert® software. The bile salt used was sodium deoxycholate which acted as a penetration enhancer that helped enhancing the permeation of the drug through the skin. The optimum formula had high drug encapsulation efficiency with spherical morphology. Confocal laser scanning microscopy proved the ability of the fluoro-labeled bilosomes to enter deeply into the skin. Studies of ex vivo permeability and in vivo skin deposition were much better in bilosomes compared to the drug solution. Also, histopathological examination verified the topical safety of bilosomes. Overall, the outcomes proved that bilosomes can be implemented for the transdermal delivery of drugs.
Lornoxicam-loaded bilosomes were formulated and assessed by Salama et al. for effective treatment of osteoarthritis [50]. A thin film hydration procedure was applied to formulate the bilosomes applying 23 full factorial design. Design-Expert® software was applied to study the effect of changing the type of bile salt, the amount of drug, and the ratio of phosphatidylcholine to bile salt. Sodium deoxycholate and sodium taurocholate were used as bile salts acting as permeability enhancers giving bilosomes the ability to permeate through skin. The optimum bilosomes formula had a spherical morphology and biphasic in vitro release profile of the drug following Higuchi’s model. Also, in vivo results proved the efficacy of lornoxicam-loaded bilosomes for treating osteoarthritis by boosting locomotor activity and coordination, suppressing pro-inflammatory cytokines, NF-κβ and IL-6, and blocking the pathway of mitogen-activated protein kinases/extracellular signal-regulated kinase. Furthermore, histopathological examination of knee joint tissues displayed a decrease in inflammatory cell infiltration with average articular cartilage and average synovial lining. The outcomes showed that bilosomes can be used in the management of osteoarthritis as a promising system.
Cubosomes
Cubosomes were discovered in the 1980s [74]. They are cubic crystalline, distinct nanovesicles formed by the liquid–crystalline dispersion of cubic masses in aqueous media (Fig. 4) [75]. They can be prepared using biodegradable lipid ingredients, such as monoglycerides, for example, monoolein [52]. Cubosomes are described by the identical microstructure of their parent cubic aggregates and their high surface area [76]. They are safe, non-immunogenic, bioadhesive, and biocompatible vesicles [77]. Also, cubosomes are simply prepared and provide a great approach for improving the bioavailability of drugs with poor water solubility [78]. Cubosomes unique ordered structure gives them the capability to include high amounts and large varieties of drugs because of their high inner surface area [35]. Furthermore, cubosomes increase the skin permeation of drugs; this might be explained by the penetration action of the monoglycerides which can agitate the skin’s ordered structure by developing hydrophobic interaction with the skin lipid [52]. Cubosomes limitations include low stability and difficulty in large-scale production.
Hundekar et al. developed cubosomes of diclofenac sodium for the management of muscle pain and inflammation through percutaneous administration for avoiding the major side effects caused by systemic drug administration [51]. The top-down method with homogenization was used to prepare cubosomes using changed ratios of glyceryl monooleate and polymer 407. Glyceryl monooleate enhances the drug’s penetration through the skin. The formulated cubosomes displayed good compatibility and stability, with a spherical and smooth morphology. Moreover, the optimum cubosomal formula showed a good in vitro release profile. Also, in vivo evaluation studies of the optimum formula ensured more effective sustained release than drug-marketed gel. In brief, cubosomes are a great-controlled release system for the efficient delivery of diclofenac sodium.
Salah et al. prepared etodolac-loaded cubosomes for transdermal management of rheumatoid arthritis by providing a stable etodolac concentration at particular sites through controlled drug delivery [52]. Cubosomes were formulated using different ratios of poloxamer 407 and monoolein via emulsification and homogenization processes. The formulated cubosomes offered high encapsulation efficiency and high drug loading capacity, with cubic and hexagonal shapes. They also had a controlled drug release profile. The differential scanning calorimetric and X-ray analyses showed that etodolac was entrapped in the bicontinuous cubosomes’ structures. Also, cubosomes displayed quick drug permeation across mice skin at first, then a slow drug permeation took place up to 24 h. Furthermore, the pharmacokinetic study in human volunteers presented that the optimum cubosomes’ formula had an extensive half-life and improved etodolac bioavailability (266.11%) than the oral capsules. Therefore, cubosomes offer a good system for the topical management of arthritis.
Spanlastics
Spanlastics are flexible nanovesicles that contain a non-ionic surfactant and an edge activator (Fig. 4) [36]. They have good patient compliance, high target specificity, high convenience, and great chemical stability [37]. Spanlastics are promising vesicles as the existence of an edge activator provides the spanlastics with high flexibility [79, 80], which increases their ability to permeate drugs through the skin. One of spanlastics’ limitations is the low release profile caused by long-chain surfactant.
Celecoxib-loaded spanlastics were prepared by Alaaeldin et al. for the topical delivery of the drug for the management of the inflamed joints associated with rheumatoid arthritis [53]. Spanlastics were formulated applying a modified injection procedure using Span 60 and different types of edge activators (Tween 80 and Brij®35) to enhance the penetration of celecoxib through the skin. The formulated spanlastics had high entrapment efficiency with a small vesicle size. The optimum spanlastics’ formula had a higher permeability coefficient and transdermal flux in relation to other formulas. Celecoxib-loaded spanlastics gel decreased edema and suppressed NF-кB, TNF-α, and COX-2 levels significantly in relation to the conventional niosomal gel, the commercial diclofenac sodium gel, and the drug gel. The study showed that spanlastics are a more effective site-specific topical treatment of chronic inflammation, such as rheumatoid arthritis, than the market and other conventional substitutes.
Farghaly et al. formulated fenoprofen calcium-loaded spanlastics intended for topical delivery to avoid gastrointestinal effects of the drug such as ulceration, irritation, and gastric bleeding and for efficient treatment of inflammation, pain, and stiffness concomitant with rheumatoid arthritis and osteoarthritis [54]. A thin film hydration technique was employed to prepare the spanlastics based on 23 full factorial design to inspect the effect of different levels of Span 60, different types of edge activators, and different types of cosolvent. Edge activators used were Cremophor EL and Tween 60 as penetration enhancers of the formulated spanlastics. The optimum formula had a spherical shape. Also, the optimum fenoprofen calcium-loaded spanlastic gel had a sustained slow in vitro release profile compared to the conventional fenoprofen calcium gel. The permeability study through the skin exposed that spanlastics’ gel displayed steady and extended action. Also, the spanlastics’ gel inhibition percentage of carrageenan-induced rat paw edema was 3 times more than the conventional gel after 24 h. Overall, spanlastics gel is a great system for the topical treatment of arthritis using fenoprofen calcium.
Cerosomes
Cerosomes are vesicles with ceramide in their structure. They are prepared using different surfactants and phospholipids. Cerosomes have great stability and permeability, with high topical drug bioavailability [38, 81]. They are prepared using a mixture of lipidic phosphatidylcholine-ceramide with a surfactant to enhance the stability of the vesicles [82, 83]. Cerosomes high skin permeation can be explained by their adsorption to the stratum corneum surface and fusion with its lipid matrix. This causes transitions of stratum corneum lipids and keratin, thus increasing their fluidity and reducing the diffusional resistance of stratum corneum towards the drug, leading to enhanced permeation of the drug through the skin [82]. Moreover, studies showed that ceramide has an anti-inflammatory activity on its own, making cerosomes an excellent promising carrier for the delivery of NSAIDs [84]. Cerosomes structure is shown in Fig. 4.
An application of NSAID-loaded cerosomes is the study of Fathi-Azarbayjani et al. which included the formulation of cerosomes for the delivery of diclofenac through the skin [38]. Diclofenac-loaded cerosomes were obtained and assessed compared with conventional liposomes, ethosomes, transferosomes, proniosomes, and niosomes. The observations of Fourier transform infrared indicated that the vesicles increased stratum corneum lipid fluidization and altered protein conformation. Skin permeability profile revealed that the cerosomal formula caused a significant increase in diclofenac permeation across the skin compared with other vesicles. Overall, cerosomes are great promising vesicles for topical and transdermal delivery of diclofenac.
Conclusion
Since inflammatory conditions are common and require rapid management, the need to create advanced systems rises to enhance drug efficacy and avoid the limitations of conventional systems. Advanced vesicular carriers are innovative drug delivery systems that augment the delivery of NSAIDs through the skin. They can target NSAIDs to the desired action site and diminish their side effects, thus improving their therapeutic efficacy in the management of inflammatory diseases. Each vesicular system has a special ingredient that improves drug penetration through the skin and enhances its bioavailability. Overall, advanced vesicular carriers will likely replace conventional systems as more formulas become available commercially.
References
Vane JR, Botting RM. Mechanism of action of anti-inflammatory drugs. Scand J Rheumatol. 1996;25:9–21.
Ahmed AU. An overview of inflammation: mechanism and consequences. Front Biol. 2011;6:274–81.
Hyrich KL, Silman AJ, Watson KD, Symmons DPM. Anti-tumour necrosis factor therapy in rheumatoid arthritis: an update on safety. Ann Rheum Dis. 2004;63:1538–43.
Lee JL, Mukhtar H, Bickers DR, Kopelovich L, Athar M. Cyclooxygenases in the skin: pharmacological and toxicological implications. Toxicol Appl Pharmacol. 2003;192:294–306.
Dudhgaonkar SP, Tandan SK, Bhat AS, Jadhav SH, Kumar D. Synergistic anti-inflammatory interaction between meloxicam and aminoguanidine hydrochloride in carrageenan-induced acute inflammation in rats. Life Sci. 2006;78:1044–8.
Bindu S, Mazumder S, Bandyopadhyay U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: a current perspective. Biochem Pharmacol. 2020;180:1–21.
Green GA. Understanding NSAIDs: from aspirin to COX-2. Clin Cornerstone. 2001;3:50–9.
García-Rayado G, Navarro M, Lanas A. NSAID induced gastrointestinal damage and designing GI-sparing NSAIDs. Expert Rev Clin Pharmacol. 2018;11:1031–43.
Ammar H, Makram TS, Mosallam S. Effect of polymers on the physicochemical properties and biological performance of fenoprofen calcium dihydrate-triacetyl-β-cyclodextrin complex. Pharmaceutics. 2017;9:1–19.
Atchison JW, Herndon CM, Rusie E. NSAIDs for musculoskeletal pain management: current perspectives and novel strategies to improve safety. J Manag Care Pharm. 2013;19:1–19.
Heyneman CA, Lawless-Liday C, Wall GC. Oral versus topical NSAIDs in rheumatic diseases: a comparison. Drugs. 2000;60:555–74.
Vane JR, Botting RM. Mechanism of action of nonsteroidal anti-inflammatory drugs. Am J Med. 1998;104:2–8s.
Boelsterli U. Diclofenac-induced liver injury: a paradigm of idiosyncratic drug toxicity. Toxicol Appl Pharmacol. 2003;192:307–22.
Weir MR. Renal effects of nonselective NSAIDs and coxibs. Clevel Clin J Med. 2002;69:si53–8.
Stanos. Osteoarthritis guidelines: a progressive role for topical nonsteroidal anti-inflammatory drugs. J Multidiscip Healthc. 2013;6:133–7.
McPherson ML, Cimino NM. Topical NSAID formulations. Pain Med. 2013;14:s35–9.
El Mahrab RM, Kalia YN. New developments in topical antifungal therapy. Am J Drug Deliv. 2006;4:231–47.
Jiménez-Rodríguez A, Guardado-Félix D, Antunes-Ricardo M. Challenges and strategies for topical and transdermal delivery of bioactive peptides. Crit Rev Ther Drug Carrier Syst. 2022;39:1–31.
Bseiso E, Nasr M, Abd El Gawad N, Sammour O. Recent advances in topical formulation carriers of antifungal agents. Indian J Dermatol Venereol Leprol. 2015;81:457–63.
Shah H, Nair AB, Shah J, Jacob S, Bharadia P, Haroun M. Proniosomal vesicles as an effective strategy to optimize naproxen transdermal delivery. J Drug Deliv Sci Technol. 2021;63:1–10.
Myneni GS, Radha GV, Soujanya GVRL. Novel vesicular drug delivery systems: a review. Indo Am J Pharm Res. 2021;11:1650–64.
Mosallam S, Albash R, Abdelbari MA. Advanced vesicular systems for antifungal drug delivery. AAPS PharmaSciTech. 2022;23:1–11.
Rao BN, Reddy KR, Mounika B, Fathima SR, Tejaswini A. Vesicular drug delivery system: a review. Int J ChemTech Res. 2019;12:39–53.
Nasr M, Mansour S, Mortada ND, Elshamy AA. Vesicular aceclofenac systems: a comparative study between liposomes and niosomes. J Microencapsul. 2008;25:499–512.
Carter P, Narasimhan B, Wang Q. Biocompatible nanoparticles and vesicular systems in transdermal drug delivery for various skin diseases. Int J Pharm. 2019;555:49–62.
Kumar S, Maurya H. An overview on advance vesicles formulation as a drug carrier for n.d.d.s. European J Biomed Pharm Sci. 2018;5:292–303.
Mosallam S, Ragaie MH, Moftah NH, Elshafeey AH, Abdelbary AA. Use of novasomes as a vesicular carrier for improving the topical delivery of terconazole: in vitro characterization, in vivo assessment and exploratory clinical experimentation. Int J Nanomedicine. 2021;16:119–32.
Yasam VR, Jakki SL, Natarajan J, Kuppusamy G. A review on novel vesicular drug delivery: proniosomes. Drug Deliv. 2014;21:243–9.
Mohanty D, Jhansi M, Bakshi DV, Haque MA. Proniosome: a novel polymeric vesicular drug carrier. J Glob Trends Pharm Sci. 2018;9:5083–95.
Rajendar M, Chandrashekar KB, Srinivas DA. Ethosomes as novel drug delivery carriers – a review. Indo Am J Pharm Sci. 2016;3:1639–43.
Abdulbaqi IM, Darwis Y, Khan NA, Abou Assi R, Khan AA. Ethosomal nanocarriers: the impact of constituents and formulation techniques on ethosomal properties, in vivo studies, and clinical trials. Int J Nanomedicine. 2016;11:2279–304.
Bajaj KJ, Parab BS, Shidhaye SS. Nano-transethosomes: a novel tool for drug delivery through skin. Indian J Pharm Educ Res. 2021;55:s1-10.
Mosallam S, Sheta NM, Elshafeey AH, Abdelbary AA. Fabrication of highly deformable bilosomes for enhancing the topical delivery of terconazole: in vitro characterization, microbiological evaluation, and in vivo skin deposition study. AAPS PharmSciTech. 2021;22:1–12.
Palekar-Shanbhag P, Lande S, Chandra R, Rane D. Bilosomes: superior vesicular carriers. Curr Drug Ther. 2020;15:312–20.
Garg G, Saraf S, Saraf S. Cubosomes: an overview. Biol Pharm Bull. 2007;30:350–3.
Kakkar S, Kaur IP. Spanlastics—a novel nanovesicular carrier system for ocular delivery. Int J Pharm. 2011;413:202–10.
Liu Y, Wang Y, Yang J, Zhang H, Gan L. Cationized hyaluronic acid coated spanlastics for cyclosporine A ocular delivery: prolonged ocular retention, enhanced corneal permeation and improved tear production. Int J Pharm. 2019;565:133–42.
Fathi-Azarbayjani A, Ng KX, Chan YW, Chan SY. Lipid vesicles for the skin delivery of diclofenac: cerosomes vs. other lipid suspensions. Adv Pharm Bull. 2015;5:25–33.
Ammar HO, Ghorab M, El-Nahhas SA, Higazy IM. Proniosomes as a carrier system for transdermal delivery of tenoxicam. Int J Pharm. 2011;405:142–52.
Wen MM, Farid RM, Kassem AA. Nano-proniosomes enhancing the transdermal delivery of mefenamic acid. J Liposome Res. 2014;24:280–9.
Kommana N, Babu MK. Formulation and evaluation of soyalecithin based emulsomes for topical administration of lornoxicam. Ind J Res Pharma Biotech. 2016;4:28–38.
Kaur G, Negi K, Kumar K, Teotia D. Development and evaluation of pharmacosome formulations of mefenamic acid. GSC Biol Pharm Sci. 2021;16:229–34.
Tawfeek HM, Abdellatif AAH, Abdel-Aleem JA, Hassan YA, Fathalla D. Transfersomal gel nanocarriers for enhancement the permeation of lornoxicam. J Drug Deliv Sci Technol. 2020;56:1–10.
Shaji J, Lal M. Preparation, optimization and evaluation of transferosomal formulation for enhanced transdermal delivery of a COX-2 inhibitor. Int J Pharm Pharm Sci. 2014;6:467–77.
Chourasia MK, Kang L, Chan SY. Nanosized ethosomes bearing ketoprofen for improved transdermal delivery. Results Pharma Sci. 2011;1:60–7.
Sakdiset P, Amnuaikit T, Pichayakorn W, Pinsuwan S. Formulation development of ethosomes containing indomethacin for transdermal delivery. J Drug Deliv Sci Technol. 2019;52:760–8.
Kaul S, Jain N, Nagaich U. Ultra deformable vesicles for boosting transdermal delivery of 2-arylpropionic acid class drug for management of musculoskeletal pain. J Pharm Investig. 2022;52:217–31.
Garg V, Singh H, Bhatia A, Raza K, Singh SK, Singh B, et al. Systematic development of transethosomal gel system of piroxicam: formulation optimization, in vitro evaluation, and ex vivo assessment. AAPS PharmSciTech. 2017;18:58–71.
Al-mahallawi AM, Abdelbary AA, Aburahma MH. Investigating the potential of employing bilosomes as a novel vesicular carrier for transdermal delivery of tenoxicam. Int J Pharmaceutics. 2015;485:329–40.
Salama A, El-Hashemy HA, Darwish AB. Formulation and optimization of lornoxicam-loaded bilosomes using 23 full factorial design for the management of osteoarthritis in rats: modulation of MAPK/Erk1 signaling pathway. J Drug Deliv Sci Technol. 2022;69:1–12.
Hundekar YR, Saboji DJK, Patil SM, Nanjwade DBK. Preparation and evaluation of diclofenac sodium cubosomes for percutaneous administration. World J Pharm Pharm Sci. 2014;3:523–39.
Salah S, Mahmoud AA, Kamel AO. Etodolac transdermal cubosomes for the treatment of rheumatoid arthritis: ex vivo permeation and in vivo pharmacokinetic studies. Drug Deliv. 2017;24:846–56.
Alaaeldin E, Abou-Taleb HA, Mohamad SA, Elrehany M, Gaber SS, Mansour HF. Topical nano-vesicular spanlastics of celecoxib: enhanced anti-inflammatory effect and down-regulation of TNF-α, NF-кB and COX-2 in complete freund’s adjuvant-induced arthritis model in rats. Int J Nanomedicine. 2021;16:133–45.
Farghaly DA, Aboelwafa AA, Hamza MY, Mohamed MI. Topical delivery of fenoprofen calcium via elastic nano-vesicular spanlastics: optimization using experimental design and in vivo evaluation. AAPS PharmSciTech. 2017;18:2898–909.
Thimmaraju DR, Kurnool A. Proniosomal gel: formulation and charecterization of an antifungal drug (Butenafine Hcl) loaded proniosomes for topical delivery. Glob J Med Res. 2020;20:35–46.
Radha G, Rani Ts, Sarvani B. A review on proniosomal drug delivery system for targeted drug action. J Basic Clin Pharma. 2013;4:42–8.
Mohamed LK, Abdel-mottaleb MMA, Geneidi AS. Formulation and characterization of proniosomal gels loaded with levofloxacin for dermal drug delivery. Arch Pharm Sci Ain Shams Univ. 2021;5:288–303.
Gill B, Singh J, Sharma V, Hari KS. Emulsomes: an emerging vesicular drug delivery system. Asian J Pharm. 2012;6:87–94.
Eita AS, Makky AMA, Anter A, Khalil IA. Atorvastatin-loaded emulsomes foam as a topical antifungal formulation. Int J Pharms:X. 2022;4:1–20.
Varshosaz J, Raghami F, Rostami M, Jahanian A. PEGylated trimethylchitosan emulsomes conjugated to octreotide for targeted delivery of sorafenib to hepatocellular carcinoma cells of HepG2. J Liposome Res. 2019;29:383–98.
Bhingare U, Khadabadi DSS, Shinde N. Pharmacosomes: a novel drug delivery system. Int J Pharm Res Allied Sci. 2014;3:14–20.
Supraja B, Mulangi S. An updated review on pharmacosomes, a vesicular drug delivery system. J Drug Deliv Ther. 2019;9:393–402.
Semalty A, Semalty M, Rawat BS, Singh D, Rawat M. Pharmacosomes: the lipid-based new drug delivery system. Expert Opin Drug Deliv. 2009;6:599–612.
Bhasin B, Londhe VY. An overview of transfersomal drug delivery. Int J Pharm Sci Res. 2018;9:2175–84.
Hua S. Lipid-based nano-delivery systems for skin delivery of drugs and bioactives. Front Pharmacol. 2015;6:1–5.
Opatha SAT, Titapiwatanakun V, Chutoprapat R. Transfersomes: a promising nanoencapsulation technique for transdermal drug delivery. Pharmaceutics. 2020;12:1–23.
Kumar A, Pathak K, Bali V. Ultra-adaptable nanovesicular systems: a carrier for systemic delivery of therapeutic agents. Drug Discov Today. 2012;17:1233–41.
Fernández-García R, Lalatsa A, Statts L, Bolás-Fernández F, Ballesteros MP, Serrano DR. Transferosomes as nanocarriers for drugs across the skin: quality by design from lab to industrial scale. Int J Pharm. 2020;573:1–15.
Kumar L, Verma S, Bhardwaj A, Vaidya S, Vaidya B. Eradication of superficial fungal infections by conventional and novel approaches: a comprehensive review. Artif Cells Nanomed Biotechnol. 2014;42:32–46.
Shaji J, Bajaj R. Transethosomes: a new prospect for enhanced transdermal delivery. Int J Pharm Sci Res. 2018;9:2681–5.
Albash R, El-Nabarawi MA, Refai H, Abdelbary AA. Tailoring of PEGylated bilosomes for promoting the transdermal delivery of olmesartan medoxomil: in-vitro characterization, ex-vivo permeation and in-vivo assessment. Int J Nanomedicine. 2019;14:6555–74.
Abdelbari MA, El-Gazar AA, Abdelbary AA, Elshafeey AH, Mosallam S. Brij® integrated bilosomes for improving the transdermal delivery of niflumic acid for effective treatment of osteoarthritis: in vitro characterization, ex vivo permeability assessment, and in vivo study. Int J Pharm. 2023;640:1–13.
Chilkawar RN, Nanjwade BK, Idris SAM, Nwaji MS, Mohamied AS, Idris NF. Bilosomes based drug delivery system. J Chem App. 2015;2:1–5.
Dhadwal A, Sharma DR, Pandit V, Ashawat MS, Kumar P. Cubosomes: a novel carrier for transdermal drug delivery. J Drug Delivery Ther. 2020;10:123–30.
Gaballa S, El Garhy O, Abdelkader H. Cubosomes: composition, preparation, and drug delivery applications. J Adv Biomed Pharm Sci. 2019;3:1–9.
Omar S, Ismail A, Hassanin K, Hamdy S. Formulation and evaluation of cubosomes as skin retentive system for topical delivery of clotrimazole. J Adv Pharm Res. 2019;3:68–82.
Huang J, Peng T, Li Y, Zhan Z, Zeng Y, Huang Y, et al. Ocular cubosome drug delivery system for timolol maleate: preparation, characterization, cytotoxicity, ex vivo, and in vivo evaluation. AAPS PharmSciTech. 2017;18:2919–26.
Gan L, Han S, Shen J, Zhu J, Zhu C, Zhang X, et al. Self-assembled liquid crystalline nanoparticles as a novel ophthalmic delivery system for dexamethasone: improving preocular retention and ocular bioavailability. Int J Pharmaceutics. 2010;396:179–87.
Abdelbari MA, El-mancy SS, Elshafeey AH, Abdelbary AA. Implementing spanlastics for improving the ocular delivery of clotrimazole: in vitro characterization, ex vivo permeability, microbiological assessment and in vivo safety study. Int J Nanomedicine. 2021;16:6249–61.
Ansari MD, Saifi Z, Pandit J, Khan I, Solanki P, Sultana Y, et al. Spanlastics a novel nanovesicular carrier: its potential application and emerging trends in therapeutic delivery. AAPS PharmSciTech. 2022;23:1–12.
Ahmed S, Amin MM, Sayed S. A comprehensive review on recent nanosystems for enhancing antifungal activity of fenticonazole nitrate from different routes of administration. Drug Delivery. 2023;30:1–16.
Yang X, Tang Y, Wang M, Wang Y, Wang W, Pang M, et al. Co-delivery of methotrexate and nicotinamide by cerosomes for topical psoriasis treatment with enhanced efficacy. Int J Pharm. 2021;605:1–16.
Strati F, Mukhina T, Neubert RHH, Opalka L, Hause G, Schmelzer CEH, et al. Cerosomes as skin repairing agent: mode of action studies with a model stratum corneum layer at liquid/air and liquid/solid interfaces. BBA Advances. 2022;2:1–11.
Carneiro R, Salgado A, Raposo S, Marto J, Simões S, Urbano M, et al. Topical emulsions containing ceramides: effects on the skin barrier function and anti-inflammatory properties. Eur J Lipid Sci Technol. 2011;113:961–6.
Funding
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB). This review was financed by the authors.
Author information
Authors and Affiliations
Contributions
MAA: data collection, writing, visualization, data curation.
AHE: data curation, assessment, editing, and reviewing.
AAA: data curation, conceptualization, editing, and reviewing.
SM: data curation, assessment, reviewing, and editing.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Abdelbari, M.A., Elshafeey, A.H., Abdelbary, A.A. et al. Implementing Nanovesicles for Boosting the Skin Permeation of Non-steroidal Anti-inflammatory Drugs. AAPS PharmSciTech 24, 195 (2023). https://doi.org/10.1208/s12249-023-02649-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1208/s12249-023-02649-x