
Abstract
Antimicrobial resistance poses a global threat to human health. Analyzing monitoring data on antimicrobial resistance can assist clinicians in making strategic decisions and promptly identifying outbreaks of antimicrobial-resistant organisms. The China Antimicrobial Surveillance Network (CHINET) was established in 2004 to monitor the trends in bacterial epidemiology and antimicrobial resistance. In this study, we analyzed the distribution and changing antimicrobial resistance profiles of Enterobacter spp. isolated from 53 hospitals across China between 2015 and 2021 using the CHINET data. Over the seven-year period, a total of 37,966 clinical isolates of Enterobacter spp. were obtained, accounted for 2.5% of all isolates and 5.7% of Enterobacteriaceae isolates. Among those isolates, Enterobacter cloacae was the most prevalent, comprising 93.7% (35,571/37,966). The majority of strains were isolated from respiratory tract samples (44.6%), followed by secretion, pus (16.4%), and urine samples (16.0%). As for patient composition, 37,966 Enterobacter spp. strains were predominantly isolated from inpatients (92.9%), whereas 7.1% were isolated from outpatients and emergency patients. Among inpatients, isolates from patients in surgical ward accounted for the highest percentage (24.4%). E. cloacae exhibited the lowest rates of resistance to amikacin, tigecycline, polymyxin B, imipenem, and meropenem (resistance rates < 8%). However, the percentage of carbapenem-resistant Enterobacter spp. was 10.0%, presenting a rising tendency over the 7-year study period. Antimicrobial resistance profiles of Enterobacter spp. isolates varied according to the department of isolation and patient age (adult or child), with the intensive care unit having the highest proportion of carbapenem-resistant Enterobacter spp. isolates.
Similar content being viewed by others
Introduction
The genus Enterobacter belongs to the ESKAPE group (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species) and is one of the main pathogens that cause nosocomial infections, due to its multiple resistance mechanisms and the ability to "evade" antimicrobial therapy. Those group of bacteria can cause a multitude of hospital-acquired infections and less common community-acquired infections, including bacteremia, urinary tract infections, respiratory infections, soft tissue infections, osteomyelitis, and endocarditis [1].
As the third-ranked Enterobacteriaceae, E. cloacae is naturally resistant to ampicillin, amoxicillin-clavulanate, first-generation cephalosporins, and cefoxitin due to the production of low levels of inducible AmpC β-lactamase. This cephalosporinase is highly inducible in the presence of some β-lactams (e.g., third generation cephalosporins, aztreonam). Overexpression of this enzymes can lead to resistance to broad-spectrum cephalosporins, with the exception of cefepime. Consequently, even when third-generation cephalosporins show sensitivity, cautious consideration should be given to their clinical use in treating severe infections caused by Enterobacter cloacae [2, 3]. Moreover, our statistics have shown that the abundance of carbapenem-resistant E. cloacae (CR-ECL) is increasing. Antimicrobial resistance (AMR) poses an enormous health and economic burden [4, 5], particularly with respect to Enterobacteriaceae, which are third-generation cephalosporin-resistant, carbapenem-resistant, and multidrug-resistant bacteria. Therefore, it is imperative for clinical laboratories and public health organizations to remain vigilant regarding the evolving landscape antimicrobial resistance in Enterobacter spp., especially E. cloacae.
The China Antimicrobial Surveillance Network (CHINET, www.chinets.com) is one of the most influential antimicrobial resistance surveillance networks in China, with members covering 30 provinces, autonomous regions and municipalities directly under the central government in China to date. All members voluntarily apply to join the network and undergo verification to ensure the laboratory capacity and data meet satisfactory standards. They perform antimicrobial resistance surveillance in accordance with a unified surveillance program to ensure that data are uniform, accurate and comprehensive. The data for this study were obtained from 53 hospitals (42 tertiary hospitals and 11 secondary hospitals or 46 general and 7 children’s hospitals) spanning 29 provinces and cities across China.
Results
Proportion of Enterobacter spp.
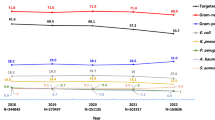
A total of 37,966 nonduplicated isolates of Enterobacter spp. were obtained from the CHINET Antimicrobial Resistance Surveillance Program between 2015 and 2021. These isolates accounted for 2.5% of all clinical isolates (37,966 of 1,500,839) and 5.7% of Enterobacteriaceae isolates (37,966 of 661,336). The isolation rate of Enterobacter spp. exhibited a fluctuating trend over the study period (Supplementary Table 1). Among the isolates, 93.7% (35,571 strains) were identified as E. cloacae, 3.3% (1,239 strains) as Enterobacter asburiae, and 0.8% (292 strains) as Enterobacter gergeoviae. The remaining Enterobacter spp. included Enterobacter cancerogenus (formerly Enterobacter taylorae), with 121 strains; Enterobacter amnigenus, with 118 strains; and 625 strains of Enterobacter spp. that were not successfully identified to species. Compared with 2015, there was a decrease in the proportion of E. cloacae among Enterobacter spp., but the proportion of E. asburiae was significantly increased (Supplementary Table 2).
Regarding the specimen sources of E. cloacae isolates, respiratory secretion specimens were the most common, accounting for 44.6% of isolates, followed by secretions/pus, urine, blood/bone marrow, bile, thoracoabdominal fluid, and cerebrospinal fluid. The percentage of respiratory samples demonstrated a downward trend over the 7-year study period whereas the proportions of secretions/pus, blood/bone marrow, and drainage fluid increased (Supplementary Table 3).
Departmental distribution of Enterobacter spp.
Among Enterobacter spp. isolates, those from adult patients (≥ 18 years old) accounted for 85.9% of the total, with an average proportion from inpatients was 92.9%. Isolates were predominantly obtained from the surgical department (24.4%), followed by the department of medicine (20.1%), intensive care unit (ICU, 11.9%), and pediatric department (10.4%). The proportion of isolates from pediatric patients decreased over the 7-year period whereas the number from patients in the ICU and neurology departments increased significantly, the proportion of patients in the outpatient and emergency departments also exhibited a sawtooth increase (Supplementary Table 4).
Resistance of Enterobacter spp. to different antimicrobial drugs
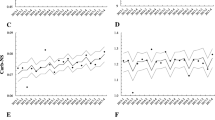
Isolated Enterobacter spp. mainly included E. cloacae, E. asburiae, E. gergoviae, and E. cancerogenus. Antimicrobial susceptibility testing revealed that E. cloacae was resistant to most cephalosporins, including ceftazidime (32.8%) and cefotaxime (41.6%); however, the rate of resistance to cefepime was low, at approximately 15.0%. The antimicrobial activities of amikacin, polymyxin B, meropenem, and imipenem were the most effective, with sensitivity rates of over 90%. E. cloacae showed an increasing trend of resistance to a wide range of antimicrobial drugs including carbapenems, cephalosporins (except for cefotaxime), β-lactamase inhibitors, and quinolones over the 7 years from 2015 to 2021 (P < 0.005). No significant trend was observed in the rates of resistance against cefotaxime, gentamicin, nitrofurantoin, polymyxin B and sulfamethoxazole-trimethoprim (P > 0.05) over the 7-year study period (Supplementary Table 5, Fig. 1).

Resistance rates of E. cloacae to antimicrobial agents from 2015 to 2021. Analysis of the chi-square test results revealed a significant linear trend in the distribution of antimicrobial resistance (P < 0.005). AK, amikacin; IMP, imipenem; MEM, meropenem; FEP, cefepime; CZ, ceftazidime; CRO, ceftriaxone; SCF, cefoperazone-sulbactam; TZP, piperacillin-tazobactam; CIP, ciprofloxacin; TGC, tigecycline
E. cloacae had a higher rate of resistance to various antimicrobial drugs compared to E. asburiae and E. gergoviae, except for polymyxin B; the rates of resistance to polymyxin B were as follows: E. cloacae 3.9%, E. asburiae 19.7%, and E. gergoviae 10.5%. E. asburiae had the lowest resistance rates to amikacin, gentamicin, cefepime, and carbapenems (≤ 8%). E. gergoviae demonstrated lower resistance rates than E. cloacae and E. asburiae to ceftazidime (14.3% vs. 32.8%, 24.9%), ceftriaxone (23.3% vs. 38.8%, 29.4%), cefotaxime (20.5% vs. 41.6%, 35%), and ciprofloxacin (10.8% vs. 23.8%, 17.2%). E. cancerogenus displayed significantly lower rates of resistance to most antimicrobial drugs than other Enterobacter spp. isolates, except for cefazolin (92.3% vs. 28.4%), cefuroxime (43.8% vs. 32.3%), cefoxitin (94.7% vs. 34.5%), ampicillin (84.6% vs. 34.6%), and ampicillin-sulbactam (60.0% vs. 18.9%) (Supplementary Tables 5 and 6, Fig. 2).

Resistance rates of Enterobacter strains to antimicrobial agents from 2015 to 2021. AK, amikacin; CN, gentamicin; IMP, imipenem; MEM, meropenem; FEP, cefepime; CZ, ceftazidime; CRO, ceftriaxone; CTX, cefotaxime; SCF, cefoperazone-sulbactam; FOX, cefoxitin; CXM, cefuroxime; KZ, cefazolin; TZP, piperacillin-tazobactam; AMP, ampicillin; SAM, ampicillin-sulbactam; CIP, ciprofloxacin; NIT, nitrofurantoin; TGC, tigecycline; PB, polymyxins B; SXT, sulfamethoxazole-trimethoprim
Rates of antimicrobial resistance among isolates from different departments
Antimicrobial resistance of E. cloacae varied among different departments. Isolates from patients in the ICU showed higher rates of resistance to most antimicrobial agents compared to isolates from outpatients, emergency patients, and other hospitalized non-ICU patients (P < 0.05), except for ciprofloxacin, nitrofurantoin, tigecycline, polymyxin B, and sulfamethoxazole-trimethoprim. Additionally, isolates from pediatric patients (< 18 years of age) generally displayed lower resistance rates than those from adult hospitalized non-ICU patients, except for carbapenems, where resistance rates were higher among pediatric than adult patients (P < 0.05). Isolates from surgical patients were more frequently resistant to cephalosporins and enzyme inhibitor complex antimicrobials compared to those from medical patients (P < 0.05) (Supplementary Table 7).
Carbapenem-resistant Enterobacter
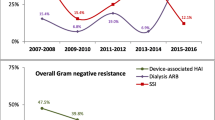
Among isolated Enterobacter spp., 93.7% were E. cloacae. The proportion of CR-ECL increased over the years from 8.4% in 2015 to 10.2% in 2021, showing an increasing trend (P < 0.05). The prevalence of carbapenem-resistant E. asburiae and E. gergoviae fluctuated and was slightly lower overall than that of CR-ECL across the previous 7 years (7.8%, 9.1% vs. 10.2%) (Supplementary Table 8). The highest rate of CR-ECL was observed in ICU patients, averaging 16.1%, followed by outpatients and emergency patients (averaging 11.4%), inpatient non-ICU patients age < 18 years, (averaging 10.4%), and surgical (averaging 9.5%) and medical patients (averaging 7.9%) (Supplementary Table 9, Fig. 3).

Prevalence of carbapenem-resistant E. cloacae isolated from different departments between 2015 and 2021. Analysis based on the trend chi-square test showed that the 2015–2021 CHINET Antimicrobial Resistance Surveillance Program revealed a linear increase in carbapenem-resistant Enterobacter cloacae over time in medical, surgical, and pediatric patients. ICU, intensive care unit
Discussion
Enterobacter was first described in 1960, and those there have been ongoing taxonomic reversion. Several species that formerly belonged to this genus have been reclassified into several new genera [6]. In 2019, Enterobacter aeogenes underwent taxonomic reclassification and was renamed Klebsiella aerogenes in both Clinical and Laboratory Standards Institute (CLSI) [7] and European Committee on Antimicrobial Susceptibility Testing (EUCAST) [8], which resulted a significant difference in both the strain distribution and antimicrobial resistance rates of Enterobacter spp. E. cloacae emerged as the predominant species within this genus. In this study, we analyzed the distribution and variability in antimicrobial resistance among all suspected pathogenic Enterobacter spp. isolated from health care facilities across most regions of China.
Our analysis showed that E. cloacae among all clinically isolated Enterobacter spp., comprising an overall proportion of 93.7% between 2015 and 2021. This was followed by E. asburiae (3.3%) and E. gergoviae (0.8%). Notably, 92.9% of strains were isolated from hospitalized patients with the majority originating from respiratory secretion samples (44.4%). Regarding ward distribution, surgical wards had the highest number of bacterial isolates (24.4%), followed by medical wards (20.1%), and the ICU and pediatric wards. The percentage of isolates from pediatric patients decreased from 13.9% in 2015 to 9.0% in 2021, whereas the percentage of isolates from patients in the ICU increased. Moreover, ICU isolates demonstrated higher rates of resistance to gentamicin, carbapenems, cephalosporins, and enzyme inhibitor combinations compared to isolates from outpatients and hospitalized non-ICU patients. Antimicrobial sensitivity testing results showed that Enterobacter spp., particularly E. cloacae, exhibited the lowest resistance to amikacin, polymyxin B, imipenem, meropenem, and tigecycline, with resistance rates all < 8%. Additionally, resistance rates of E. asburiae, E. gergoviae, and E. cancerogenus to most antimicrobial drugs were lower than those of E. cloacae.
Regarding changing trends in antimicrobial resistance, E. cloacae displayed an increasing trend toward resistance to various antibacterial drugs, except for gentamicin, nitrofurantoin, cefotaxime, polymyxin B, and sulfamethoxazole-trimethoprim; in particular, the rate of carbapenem resistance showed a significant increase. After a brief decline in 2016, antimicrobial resistance rates have recently been on the rise. The average proportion of carbapenem-resistant Enterobacter spp. over the 7-year period was 10.0%, making it the second-leading carbapenem-resistant Enterobacteriaceae (CRE), following a decreasing trend in K. pneumoniae [9]. Global antimicrobial resistance surveillance data from 2008–2018 indicate a CR-ECL proportion of 2.2%. However, we found that this proportion in China reached 12.1% in 2021, warranting urgent attention. The trend in CR-ECL observed in this study aligns with global and European trends in rates of resistance, which have continued to rise following a decline in 2016 [9]. An increase in CRE can contribute to increased mortality rates, with reports suggesting that 26% to 44% of all-cause deaths are caused by CRE infection [10]. The rates of 30- and 90-day all-cause mortality caused by carbapenem-resistant Gram-negative bacteria infections were 19% and 31% [11]. Carbapenem-resistant Enterobacter spp. were mainly isolated from ICU wards. More seriously, the percentage of CRE during the year from 2015 to 2021 showed an increasing trend each year. Admission to the ICU has been identified as an independent risk factor for acquiring CR-ECL. Autoimmune diseases, lung infections, and recent corticosteroid use are also associated with an increased risk of CR-ECL infection [12]. Medical institutions should focus on monitoring individuals with these risk factors. The primary mechanism of carbapenem resistance in E. cloacae is the production of carbapenem-hydrolyzing β-lactamases [13]. The prevalence of carbapenemase types varies across regions, with NDM being predominant in China [12,13,14]. However, cefozoxime-avibactam, a new drug for the treatment of CRE infections, is less susceptible to CR-ECL strains with NDM-type metallocarbapenemases as the primary mechanism of resistance in China than to other CREs. Additionally, a high prevalence of the mcr gene (mobile colistin resistance) in E. cloacae increases the risk of colistin resistance, thereby complicating the treatment of CR-ECL [15].
Our analysis showed that E. cloacae strains had a high percentage of resistance to third-generation cephalosporin antimicrobials, such as ceftazidime, ceftriaxone and cefotaxime (above 32.8%), but only 15% of strains were resistant to cefepime. This is because E. cloacae contains chromosomally encoded inducible ampC genes, due to de-deterrent mutations of the ampC gene or the acquisition of a plasmid-borne ampC, overproduction of AmpC β-lactamase leads to the resistance to broad spectrum cephalosporins. Third-generation cephalosporins, are unstable during AmpC enzyme hydrolysis and are easily destroyed by hydrolysis; in contrast, cefepime has been shown to be stable against such hydrolysis. High-producing AmpC-type enzyme resistant strains also often co-produce extended spectrum beta-lactams, further enhancing their resistance to broad-spectrum cephalosporins [16, 17]. Consequently, it is imperative for clinical microbiology laboratories and healthcare providers to closely monitor patients infected with these strains.
Conclusions
Antimicrobial susceptibility data for Enterobacter spp. isolated from various regions across China over a 7-year period (2015–2021) showed an increasing trend of resistance to multiple antibiotics. In particular, the proportion of CR-ECL among isolates exceeded global average significantly. It is therefore crucial to remain vigilant regarding carbapenem-resistant Enterobacter spp. and implement measures to mitigate the occurrence of antimicrobial resistance. Surveillance data of resistance facilitate clinical decision-making and reduce the unnecessary and ineffective use of antimicrobials.
Materials and methods
Bacterial isolates
This is a retrospective epidemiologic surveillance study of Enterobacter spp. infection during 2015–2021. All Enterobacter isolated from outpatients and inpatients in 53 CHINET member institutions (42 tertiary hospitals and 11 secondary hospitals or 46 general and 7 children’s hospitals), covering 29 provinces, autonomous regions, and municipalities directly under the central government during the period 2015–2021 were included. The names, grades, and geographic locations of the 53 hospitals are shown in Supplementary materials (Supplementary Table 10). Isolates from open sites such as pharyngeal swabs and feces were rejected. In addition, the same strain isolated from the same site in the same patient were rejected. Strain identification was performed by each member unit and confirmed by the central laboratory using matrix-assisted laser desorption ionization-time of fight mass spectrometry (BioMérieux, Marcy I'Etoile, France).
Antimicrobial susceptibility testing
Antimicrobial drugs monitored in this study included amikacin, gentamicin, ampicillin, ampicillin-sulbactam, piperacillin-tazobactam, cefoperazone-sulbactam, cefazolin, cefuroxime, cefoxitin, cefotaxime, ceftazidime, cefepime, imipenem, meropenem, ciprofloxacin, sulfamethoxazole-trimethoprim, nitrofurantoin (urine specimens), tigecycline, and polymyxin B. The antibiotics tested varied slightly across the years, (e.g., polymyxin B was tested after 2016). The antimicrobial susceptibility test was performed followed CLSI and the unified technical protocol specified of CHINET [18]. Antimicrobial susceptibility testing was co-produce using commercial automated systems (VITEK 2, bioMérieux, Inc., Hazelwood, MO, USA; Phoenix™, BD, Inc., Sparks, NV, USA; DL-96, Zhuhai DL Biotech. Co., Ltd., Zhuhai, China) or disk diffusion method, micro broth dilution method and E-test. All ranges of antimicrobial drug concentrations with a commercial automated antimicrobial sensitivity detector must meet the CLSI antimicrobial drug determination criteria. As required by the CHINET technical protocol, for antimicrobial drugs that are not covered by automated antimicrobial sensitivity detectors or whose concentrations do not meet the CLSI criteria for antimicrobial drug determination, other methods must be used to supplement the sensitivity test for that drug. The interpretation of susceptibility data was based on the 2021 CLSI M100-S31 guidelines [19]. Polymyxin B minimum inhibitory concentrations (MICs) were interpreted using EUCAST breakpoint for colistin [20], and tigecycline susceptibility was assessed according to the criteria of the U.S. Food and Drug Administration [21]. The methodology used was consistent across all participating hospitals over the five-year sampling period.
Strains resistant to any carbapenem antibiotics, including imipenem, meropenem, or ertapenem, were classified as CRE [22].
Statistical analysis
All medical institutions imported and shared routine antimicrobial susceptibility testing data using WHONET 5.6 software (http://www.whonet.org). We performed statistical analysis using IBM SPSS version 27.0 software (IBM Corp., Armonk, NY, USA). We analyzed the dynamic trend in the rates of resistance to different antimicrobial drugs over time using the trend chi-square test, and the variability of resistance rates among isolates from patients in different departments was analyzed using the chi-square test. A P value < 0.05 was considered statistically significant. Strain information, sample information, the departmental distribution, and resistance data information for every year between 2015 and 2021 were recorded for all datasets (Supplementary Tables 1–9).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- ICU:
-
Intensive care unit
- CLSI:
-
Clinical and Laboratory Standards Institute
- AK:
-
Amikacin
- CRE:
-
Carbapenem-resistant Enterobacteriaceae
- IMP:
-
Imipenem
- MEM:
-
Meropenem
- FEP:
-
Cefepime
- CZ:
-
Ceftazidime
- CRO:
-
Ceftriaxone
- CN:
-
Gentamicin
- CTX:
-
Cefotaxime
- SCF:
-
Cefoperazone-sulbactam
- TZP:
-
Pipracillin-tazobactam
- CIP:
-
Ciprofloxacin
- TGC:
-
Tigecycline
- SXT:
-
Sulfamethoxazole-trimethoprim
- CR-ECL:
-
Carbapenem-resistant Enterobacter cloacae
- EUCAST:
-
European Committee on Antimicrobial Susceptibility Testing
References
Ramirez D, Giron M. Enterobacter infections. Treasure Island: StatPearls Publishing; 2023.
Jacoby GA. AmpC beta-lactamases. Clin Microbiol Rev. 2009;22(1):161–82.
Guerin F, Isnard C, Cattoir V, Giard JC. Complex regulation pathways of AmpC-mediated beta-Lactam resistance in Enterobacter cloacae Complex. Antimicrob Agents Ch. 2015;59(12):7753–61.
Cassini A, Hogberg LD, Plachouras D, Quattrocchi A, Hoxha A, Simonsen GS, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19(1):56–66.
Word Health Organization. Antimicrobial resistance. https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance. Accessed 17 Dec 2023.
Iversen C, Mullane N, McCardell B, Tall BD, Lehner A, Fanning S, et al. Cronobacter gen. nov., a new genus to accommodate the biogroups of Enterobacter sakazakii, and proposal of Cronobacter sakazakii gen. nov., comb. nov., Cronobacter malonaticus sp. nov., Cronobacter turicensis sp. nov., Cronobacter muytjensii sp. nov., Cronobacter dublinensis sp. nov., Cronobacter genomospecies 1, and of three subspecies, Cronobacter dublinensis subsp. dublinensis subsp. nov., Cronobacter dublinensis subsp. lausannensis subsp. nov. and Cronobacter dublinensis subsp. lactaridi subsp. nov. Int J Syst Evol Micr. 2008;58(6):1442–7.
Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing. https://clsi.org/media/z2uhcbmv/m100ed31_sample.pdf. Accessed 17 Aug 2023.
European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 9.0. 2019. https://www.eucast.org/ast_of_bacteria/previous_versions_of_documents. Accessed 25 Feb 2024.
Rossolini GM, Stone G, Kantecki M, Arhin FF. In vitro activity of aztreonam/avibactam against isolates of Enterobacterales collected globally from ATLAS in 2019. J Glob Antimicrob Re. 2022;30:214–21.
Falagas ME, Tansarli GS, Karageorgopoulos DE, Vardakas KZ. Deaths attributable to carbapenem-resistant Enterobacteriaceae infections. Emerg Infect Dis. 2014;20(7):1170–5.
Babiker A, Clarke LG, Saul M, Gealey JA, Clancy CJ, Nguyen MH, et al. Changing epidemiology and decreased mortality associated with carbapenem-resistant gram-negative bacteria, 2000–2017. Clin Infect Dis. 2021;73(11):e4521–30.
Han M, Liu C, Xie H, Zheng J, Zhang Y, Li C, et al. Genomic and clinical characteristics of carbapenem-resistant Enterobacter cloacae complex isolates collected in a Chinese tertiary hospital during 2013–2021. Front Microbiol. 2023;14:1127948.
Davin-Regli A, Lavigne JP, Pages JM. Enterobacter spp.: update on taxonomy, clinical aspects, and emerging antimicrobial resistance. Clin Microbiol Rev. 2019;32(4):1–32.
De La Cadena E, Correa A, Munoz JS, Rojas LJ, Hernandez-Gomez C, Pallares C, et al. Molecular characterisation of carbapenem-resistant Enterobacter cloacae complex in Colombia: blaKPC and the ‘changing landscape’. J Glob Antimicrob Re. 2018;13:184–9.
Kim JS, Yu JK, Jeon SJ, Park SH, Han S, Park SH, et al. Distribution of mcr genes among carbapenem-resistant Enterobacterales clinical isolates: high prevalence of mcr-positive Enterobacter cloacae complex in Seoul, Republic of Korea. Int J Antimicrob Ag. 2021;58(5):106418–24.
Tamma PD, Doi Y, Bonomo RA, Johnson JK, Simner PJ. A primer on AmpC beta-Lactamases: necessary knowledge for an increasingly multidrug-resistant world. Clin Infect Dis. 2019;69(8):1446–55.
Davin-Regli A, Pages JM. Enterobacter aerogenes and Enterobacter cloacae; versatile bacterial pathogens confronting antibiotic treatment. Front Microbiol. 2015;6:392.
China Antimicrobial Surveillance Network. https://www.chinets.com. Accessed 1 Mar 2024.
Clinical And Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing[S]. Wayne: M100-S31; 2021.
European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 14.0. 2024. https://www.eucast.org/clinical_breakpoints/. Accessed 25 Dec 2024.
Food and Drug Administration. Tigecycline-injection products. https://www.fda.gov/drugs/development-resources/tigecycline-injection-products. Accessed 24 Mar 2023.
Centers for disease control and prevention (CDC). CRE Technical Information. https://www.cdc.gov/hai/organisms/cre/technical-info.html#Definition. Accessed 24 Mar 2023.
Acknowledgements
We sincerely thank all the CHINET members for their contribution in the collection of the isolates for this study, as following: Yang Yang, Fupin Hu and Demei Zhu from Institute of Antibiotics, Huashan Hospital, Fudan University; Yi Xie and Mei Kang from West China Hospital, Sichuan University; Fengbo Zhang and Ping Ji from First Affiliated Hospital, Xinjiang Medical University; Zhidong Hu and Jin Li from Tianjin Medical University General Hospital; Sufang Guo from Affiliated Hospital of Inner Mongolia Medical University; Han Shen and Wanqing zhou from Nanjing Drum Tower Hospital; Yingchun Xu and Xiaojiang Zhang from Peking Union Medical College Hospital, Chinese Academy of Medical Sciences&Peking Union Medical Colleg; Xuesong Xu and Chao Yan from China-Japan Union Hospital; Chuanqing Wang and Pan Fu from Children's Hospital of Fudan University; Wei Jia and Gang Li from General Hospital of Ningxia Medical University; Yuanhong Xu and Ying Huang from The First Affiliated Hospital of Anhui Medical University; Dawen Guo and Jinying Zhao from First Affiliated Hospital of Harbin Medical University; Wenen Liu and Yanming Li from Xiangya Hospital Central South University; Hua Yu and Xiangning Huang from Sichuan Province People's Hospital; Bin Shan and Yan Du from The First Affiliated Hospital of Kunming Medical University; Shanmei Wang and Yafei Chu from Henan Province People's hospital; Yuxing Ni and Jingyong Sun from Ruijin Hospital Affiliated to Shanghai Jiaotong University School of Medicine; Yunsong Yu and Jie Lin from Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University; Chao Zhuo and Danhong Su from The First Affiliated Hospital of Guangzhou Medical University; Lianhua Wei and Fengmei Zou from Gansu Provincial Hospital; Yan Jin and Chunhong Shao from Shandong Provincial Hospital; Jihong Li from The Second Hospital of Hebei Medical University; Lixia Zhang and Juan Ma from Shaanxi People's Hospital; Yunzhuo Chu and Sufei from TianThe First Affiliated Hospital of China Medical University; Jinju Duan and Jianbang Kang from The Second Hospital of Shanxi Medical University; Ruizhong Wang and Hua Fang from Shanghai Pudong New Area People's Hospital; Fangfang Hu from Guizhou Provincial People's Hospital; Yunjian Hu and Xiaoman Ai from Beijing Hospital; Fang Dong and Zhiyong Lv from Children's Hospital of Beijing, Capital Medical University; Hong Zhang and Chun Wang from Shanghai Children's Hospital, Shanghai Jiaotong University; Yong Zhao and Ping Gong from People's Hospital of Zigui County, Hubei Province; Lei Zhu and Jinhua Meng from Shanxi Children's Hospital; Xiaobo Ma adn Yanping Zheng from The First Affiliated Hospital of Xiamen University; Jinsong Wu and Yuemei Lu from Shenzhen People's Hospital; Ruyi Guo and Yan Zhu from First Hospital of Quanzhou City, Fujian Province; Kaizhen Wen and Yirong Zhang from Hospital of Jinjiang City, Fujian province; Chunlei Yue from Jiutai District People's Hospital of Jilin Province; Jiangshan Liu from Jinchang Hospital of Integrated Traditional Chinese and Western Medicine, Gansu Province; Wenhui Huang from Qinghai University Affiliated Hospital, Qinghai Province; Shunhong Xue from The People's Hospital of Huzhu County; Xuefei Hu from The First Affiliated Hospital of Nanchang University; Hongqin Gu from the People's Hospital of Guangrao County, Shandong Province; Jiao Feng from the People’s Hospital of Linshui, Sichuan Province; Shuping Zhou and Yan Zhou from Jiangxi Provincial Children's Hospital; Yunsheng Chen and Qing Meng from Shenzhen Children's Hospital; Bixia Yu from Zhenhai Longsai Hospital; Jilu Shen from The Fourth Affiliated Hospital of Anhui Medical University; Rui Dou from Lixin County People's Hospital Bozhou City, Anhui province; Shifu Wang from Qilu Children's Hospital of Shandong University; Wen He from Yingkou Economic and Technological Development Zone Central Hospital; Longfeng Liao from the People's Hospital of Ganxian District, Jiangxi Province; Lin Jiang from the People's Hospital of Huixian, Henan Province.
Author information
Authors and Affiliations
Consortia
Contributions
All the authors participated in the design and coordination of the study. S.Y. participated in the design of the study, performed the statistical analysis of the data and wrote the paper. Y.Y. collected the data. Z.S., Z.C. and D.Z. conceived the study, participated in its design and helped draft the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of Huashan Hospital, Fudan University (no. 2019–460).
Competing interests
The authors declare that they have no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table 1.
Proportion of Enterobacter spp. from 2015 to 2021. Table 2. Distribution of Enterobacter spp. over the period between 2015 and 2021. Table 3. Changes in the distribution of E. cloacae in different specimens from 2015 to 2021. Table 4. Distribution of Enterobacter spp. isolates in different clinical department from 2015 to 2021. Table 5. Susceptibility and resistance rates of E. cloacae to antimicrobial agents from 2015 to 2021. Table 6. Susceptibility and resistance rates of Enterobacter strains to antimicrobial agents from 2015 to 2021. Table 7. Susceptibility and resistance rates of E. cloacae to antimicrobial agents in different departments. Table 8. Changes in the prevalence of carbapenem-resistant Enterobacter strains from 2015 to 2021. Table 9. The incidence of carbapenem-resistant E. cloacae across various departments from 2015 to 2021. Table 10. The names, grades and geographical locations of the 53 hospitals.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yan, S., Sun, Z., Yang, Y. et al. Changing antimicrobial resistance profile of Enterobacter spp. isolates in hospitals across China: a seven-year analysis from the CHINET antimicrobial resistance surveillance program (2015–2021). One Health Adv. 2, 11 (2024). https://doi.org/10.1186/s44280-024-00044-0
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44280-024-00044-0