
Abstract
Background
Physical inactivity is considered one of the main modifiable risk factors for noncommunicable diseases. It has been proven that an active lifestyle is an efficient means of preventing and managing noncommunicable diseases. Multiple barriers have been identified that hinder engagement in conventional physical activity programs and the achievement of physical activity recommendations. Digital interventions may expand opportunities to resolve these barriers and empower people with noncommunicable diseases to be physically active. This overview of systematic reviews aims to evaluate the efficacy of digital interventions on physical activity promotion among individuals with major noncommunicable diseases.
Method
A protocol was registered in the PROSPERO database (CRD42022364350). A qualitative synthesis method was applied to summarize the efficacy data. The assessment of methodological quality using AMSTAR-2 for each systematic review was performed by two independent reviewers.
Results
Searches in nine databases resulted in seven systematic reviews for inclusion. Most of the primary studies included in these seven reviews were conducted in high-income countries. The reviews addressed five populations: participants with cancers, cardiovascular diseases, chronic obstructive pulmonary disease, type 2 diabetes, and osteoarthritis. Digital interventions were classified into two categories: interventions based on digital activity trackers and remote interventions via digital facilities. Additional components were identified in both categories of interventions such as motivational content, counseling, goal setting, tailored feedback/reminders, and other behavioral change techniques. The overall quality of the reviews ranged from critically low to low. The findings provided some evidence that both categories of interventions were effective in promoting physical activity.
Conclusion
The findings of this overview suggest that some types of digital interventions, such as self-monitoring with digital activity trackers and remote interventions via digital facilities, may be effective means of promoting physical activity across major noncommunicable diseases. The findings should be interpreted cautiously since the methodological quality of the included reviews ranged from critically low to low, and there was no consistent assessment of the certainty of evidence. Further systematic reviews are required on efficacy of digital interventions with more rigorous conducting and reporting of systematic review methodologies.
Similar content being viewed by others


Background
Noncommunicable diseases (NCDs), comprising cardiovascular diseases (CVDs), type 2 diabetes (T2D), chronic pulmonary disease, stroke, cancer, and certain musculoskeletal diseases, such as osteoporosis, back pain, and osteoarthritis, are still significant worldwide health burdens [1, 2] that are considered prominent determinants of global morbidity [3] and mortality [4]. NCDs cause the death of 41 million people each year, corresponding to 74% of all deaths worldwide with major NCDs (CVD, caner, chronic pulmonary disease, diabetes) being the cause of over 80% of all premature NCD deaths [5].
Major NCDs cause significant economic pressure in the European Union countries as they account for at least 25% of total healthcare budgets [6]. Furthermore, NCDs are considered to be the biggest challenge of healthcare systems in the 21th century in different countries and regions [7,8,9,10,11,12,13]. These numbers are increasing because of the expansion of societies, rapid and uncontrolled urbanization, and the adoption of increasingly less active lifestyles [14,15,16].
Physical activity (PA) including exercise has been well known as medicine for prevention and management of a wide range of chronic diseases including NCDs [17], also to counteract the negative consequences of physical inactivity as one of the main modifiable risk factors for NCDs [15, 18]. Multiple barriers have been identified that hinder engagement in traditional PA programs and the achievement of PA recommendations. Conventional approaches, such as educational programs [19, 20] and environmental modifications [21] encounter problems such as communication issues between healthcare professionals and patients, unfavorable environmental conditions, or psychological barriers such as problems with self-monitoring and lack of motivation [22].
Resolving these common barriers requires the design and implementation of innovative approaches such as digital interventions (DIs) [23] to promote healthy behaviors like PA [24,25,26,27].
Digital health is an umbrella term that encompasses the application of digital technologies in health care [28]. The advent of DIs presents an opportunity to transform the way health services are delivered and to encourage people affected by NCDs to actively engage in PA. DIs contain various technologies, such as smartphone applications, short message service (SMS), activity trackers, electronic records, video-based interventions, virtual reality, web-based/internet-based interventions, and telehealth platforms. These novel approaches hold the extensive accessibility of technology, providing tailored, scalable, and cost-efficient solutions to promote PA [29,30,31,32,33,34,35,36].
Depending on the digital technology involved, the interventions can be classified into two main categories. One category of interventions is based on the use of digital activity trackers for the self-monitoring of PA. Self-monitoring is recognized as one of the BCTs to encourage PA [37, 38]. It has been defined as a procedure that allows individuals to record, observe, monitor, and modify their behavior [37,38,39]. As such, it may increase an individual’s adherence to PA-promoting interventions by taking a more active role in attaining a goal instead of being passive [40]. Moreover, digital activity trackers are known as a prevailing self-monitoring tool [40, 41] that can be an effective way to promote PA [40].
Another category refers to remote interventions (websites or apps) using various components of behavioral support for PA promotion via digital facilities (smartphones, websites, email, etc.). Remote interventions have been postulated in telehealth/telemedicine definitions as the use of electronic communications and information technologies to provide participants with remote health care services [28, 42]. Remote interventions are utilized to deliver PA-promoting programs and to communicate efficiently with participants [28]. They can offer an advantageous way to overcome barriers originating from the person-to-person delivery of interventional programs. Remote interventions may minimize the effects of these barriers by reducing the cost of traveling to undertake programs [43], encouraging more adherence to intervention [44], allowing better timing of programs [45], and reducing the time needed to participate in programs [46].
The efficacy of DIs on physical activity promotion (PAP) has been increasingly investigated in recent years. These interventions contain various behavior change techniques (BCTs), such as goal-setting, self-monitoring, counseling, and tailored feedback, to empower individuals with NCDs to adopt and maintain active lifestyles [25, 47,48,49,50,51,52,53].
Previous reviews have either focused on defined populations, such as individuals with CVD, T2D, chronic obstructive pulmonary disease (COPD) [54,55,56,57] or on defined types of DIs, such as telemedicine, mobile text messaging, digital games, and mobile apps [58,59,60,61]. These overviews have revealed that DIs can be effective for PAP among individuals with major NCDs. Despite the growing interest in DI studies targeting PAP, a summary of the efficacy of DIs on PAP in individuals with major NCDs is lacking to date. Therefore, this overview of systematic reviews aims to summarize and critically appraise the existing evidence on the efficacy of DIs on PA levels in people with major NCDs, in comparison to the interventions that do not include DIs such as usual care or to the complete absence of interventions.
Methods
This overview of systematic reviews was conducted and reported in accordance with the Cochrane Systematic Review Handbook [62, 63] and Preferred Reporting Items for Overviews of Reviews (PRIOR) guidelines [64]. A predefined protocol (CRD42022364350) was registered in the PROSPERO database on October 13th, 2022. Minor deviations from protocol were presented in Additional file 1.
Search strategy
A systematic literature search was conducted on 31th August 2022 (Since inception to date noted) by a single researcher (MK) in eight electronic databases, including PubMed, Embase, Web of Science, SportDiscus, CINAHL (via EBSCO), Scopus, PsychInfo (via Ovid), Social Services Abstracts, Sociological Abstracts, and the Sports Medicine and Education Index (ASSIA) (via ProQuest), and one register, CENTRAL (via the Cochrane library). A comprehensive and structured search strategy was developed based on relevant published reviews in this field prior to the final literature search. Preliminary literature searches were conducted using a predefined combination of MeSH terms and free-text keywords for the population, intervention, comparison, outcomes, and study design (PICOS) elements. The full search strategy used for all databases, the number of retrieved studies, and search considerations for each database can be found in Additional file 2. The following a priori-defined eligibility criteria were used to include studies according to the PICOS scheme (Table 1).
Screening and data collection
To facilitate the study selection process, all retrieved studies were imported into EndNote, version X9 (Clarivate, Philadelphia, PA). A two-stage selection process based on predefined inclusion and exclusion criteria was independently conducted by two reviewers (MK and SK). In the first stage, records (i.e., titles and abstracts of reports) were screened against the inclusion and exclusion criteria with English or German languages. Records from other languages were excluded. In the second stage, the reviewers thoroughly reviewed the reports (i.e., full-text documents supplying information about a particular study). Throughout both stages of study selection, any conflicts or disagreements between the reviewers were resolved through discussion until a consensus was reached. If needed, the reviewers sought input from another team member (KP).
The data extraction was performed by a single reviewer (MK) and verified by another reviewer (MI). A data extraction form was created in accordance with recommendations from the Cochrane Handbook using Microsoft Word. The following information was extracted from the included systematic reviews: title, authors, year of publication, number of primary studies included, total number of participants, name and number of databases used in the search strategy, date range of the search, systematic review population, interventions, comparators, primary and secondary outcomes, methodological quality/risk of bias (ROB), effect estimates of PAP (with 95% confidence intervals) or narrative estimates of PAP, measures of heterogeneity, limitations, and theoretical basis of interventions.
Moreover, data on the direction of the effect (see more details on vote-counting synthesis in “Data analysis”) and country of conduction were extracted directly from primary studies when the information provided in the reviews was insufficient. We contacted the study authors if we did not have access to the full texts.
Methodological quality assessment
The included reviews were assessed for methodological quality using A MeaSurement Tool to Assess systematic Reviews (AMSTAR-2), which is a critical appraisal tool specifically designed for systematic reviews that include randomized controlled trials (RCTs) and non-RCTs [69]. AMSTAR-2 consists of 16 domains, seven of which are considered critical [69]. As AMSTAR-2 is not intended to generate an overall score, confidence in the results of each systematic review was assessed by rating the fulfillment of critical domains and non-critical weaknesses.
The overall confidence in the results was rated as “high” if no weakness or only one non-critical weakness was observed. Furthermore, overall confidence was rated as “moderate” if more than one non-critical weakness was observed, “low” if there was one critical flaw with or without non-critical weaknesses, and “critically low” if more than one critical flaw with or without non-critical weaknesses was observed [69].
The assessment of methodological quality using AMSTAR-2 for each systematic review was performed by two independent reviewers (MK and MI). Any conflicts or disagreements between the reviewers were resolved through discussion until a consensus was reached.
Internal validity and certainty of evidence of the overall body of evidence for primary studies
In this overview, we extracted and summarized the internal validity (methodological quality or ROB) and certainty of the evidence assessment’s data conducted by the authors of each review. Common tools used by review authors to assess internal validity were the PEDro scale [70], the Cochrane Collaboration ROB assessment tools 1 and 2 [71, 72], and the Jadad scale [73]. Certainty of evidence was assessed by the authors of the included systematic reviews using Grading of Recommendations Assessment, Development, and Evaluation (GRADE) [74].
Assessing primary study overlap within the included systematic review
To map out the overlap between the primary studies included in the reviews, we used the method of Pieper et al. [75] to calculate the corrected cover area (CCA) index and the steps of the overlap mapping method developed by Hennessy, Johnson [76]. The first occurrence of a primary publication is defined as the index publication. CCA is calculated as a measure of overlap by dividing the frequency of repeated occurrences of the index publication in other reviews by the product of index publications and reviews, reduced by the number of index publications [75].
In these methodologies, subsequent to the creation of a citation matrix, the overall CCA percentage was calculated. The CCA was then calculated for each subsample of the primary studies to determine overlap within each category. The CCA percentage was interpreted as slight (0–5%), moderate (6–10%), high (11–15%), and very high (over 15%) overlap of the primary studies included in the reviews [75].
Data analysis
A qualitative synthesis was applied in this overview because of the diversities in population, interventions, and outcome measures as well as the inconsistencies in effect measurement and reported data (in both meta-analyses and qualitative syntheses) throughout the included reviews. To synthesize the data from the reviews with meta-analyses, the extracted effect size of PAP with a 95% confidence interval (CI) was summarized. Magnitudes of effect were interpreted according to the effect sizes, with standardized mean difference (SMD) ≥ 0.2 = small, SMD ≥ 0.5 = moderate, and SMD ≥ 0.8 = large effect sizes [77].
For reviews without meta-analysis, vote counting based on the direction of effect was applied, which is an accepted method for qualitative synthesis according to the Cochrane Handbook [78]. Within this method, each effect estimate is categorized as showing benefit (favoring the use of DI) or inferiority (favoring the use of non-DI) based on the observed direction of effect alone [78]. In addition, a sign test was used to determine the existence of any evidence of an effect (the two-tailed p-value significance level was 0.05), as recommended in the Cochrane Handbook. The sign test was implemented using the GraphPad QuickCalcs website [79] (accessed September 2023). Because at least six studies were required to achieve a significant two-tailed p-value with the sign test, the sign test calculation was not performed if fewer than six studies were included in each individual analysis. An effect direction plot was created [80] and then an estimate of the proportion of effects favoring the DI was calculated (p = u/n, u = number of effects favoring the DI, and n = number of reviews/primary studies) along with a CI using the Wilson methods [81] for each outcome domain (objective, subjective PA).
Results from vote counting based on the direction of effect were categorized according to the decision rules presented by Weir et al. [82] based on the percentage of primary studies (outcomes) favoring DIs: 0% = no effect, 1% to 33% = generally ineffective, 34% to 66% = mixed effect, 67% and over = generally effective. When the information reported in any systematic review without meta-analysis was insufficient to perform a vote-counting synthesis, the primary studies included in the review were examined to obtain information on the direction of effect. Data analysis was performed by a researcher (MK), and the method used was reviewed by a second researcher (AJ).
Results
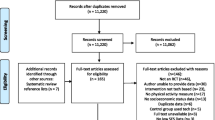
Figure 1 illustrates the various stages involved in the search and retrieval processes for this study. The initial database search yielded 4012 records. After removing duplicates (1025 records) and ineligible records (n = 34), 2953 unique records remained. Out of the initial pool, 311 reports remained and underwent a comprehensive assessment of eligibility in full text. The reasons for exclusion were documented and can be found in Additional file 3. As a result of the second stage, eight systematic reviews were identified. However, one systematic review was subsequently excluded during the data extraction process because it applied all the included remote intervention programs through landline phone calls, which did not meet the DI definition in the inclusion criteria (see Table 1). Ultimately, seven individual studies were used for data synthesis and summarization in this research.

Study selection
Description of included reviews
The characteristics of the seven included systematic reviews are presented in Additional file 4. These reviews encompassed 130 reports describing 128 RCTs conducted in 19 countries. Most of the primary studies included in these seven reviews were conducted in high-income countries. The trials were distributed across various regions, including North America (n = 53), Europe (n = 42), Australia (n = 16), Asia (n = 16), and Latin America (n = 1). The publication dates of the reviews ranged from 2010 to 2022.
Description of population
The total number of participants for each review ranged from 693 to 4,255. The combined total number of participants with major NCDs across all the included reviews in this overview was 13,631; their mean age was over 50 years. The reviews addressed five populations: participants with all types of cancers at any stage of treatment (n = 2) [83, 84]; CVDs (n = 2) [85, 86], those with COPD (n = 1) [87], those with T2D (n = 1) [88], and those with different major NCDs, such as osteoarthritis, CVDs, T2D, and COPD (n = 1) [89]. No reviews focusing on participants with back pain or osteoporosis that fit our inclusion criteria were found.
Description of interventions
Interventions based on the use of digital activity trackers for the self-monitoring of PA as the main component within either remote or non-remote interventions
The digital activity trackers mentioned in the reviews included pedometers, accelerometers, and other activity trackers, such as Fitbit, Polar, and Garmin, which have an embedded accelerometer.
Of the seven included reviews, five [83,84,85, 87, 89] focused on the use of digital activity trackers for the self-monitoring of PA among individuals with major NCDs. Three of the five reviews in this category [85, 87, 89] reported different interventional components, such as motivational content, counseling, and goal setting. Three reviews [84, 87, 89] described the motivational components of the interventions. In the same way, four reviews [84, 85, 87, 89] reported counseling components.
Furthermore, three reviews [85, 87, 89] asserted goal setting to promote PA. Except for Schaffer et al. [83], all the other reviews distinguished promoting habitual PA from structured exercise programs. Only Schaffer et al. [83] and Allet et al. [89] reported information regarding the setting of the intervention (group-based or home-based). Furthermore, except for Schaffer et al. [83], all the reviews outlined the theoretical bases of the interventions.
In the review by Allet et al. [89], the authors included primary studies using pedometers or accelerometers for long-term monitoring under free-living conditions. The authors reported the combined use of the transtheoretical model, motivational theory, alongside cognitive behavioral strategies (3 primary studies), and a combination of social cognitive theory, implementation intentions, and dual process theory (one primary study).
Armstrong et al. [87] included primary studies in which pedometers were used to provide real-time feedback on daily steps. The use of the social cognitive theory was reported in the design of one primary study.
Kanejima et al. [85] included primary studies in which the interventions utilized pedometers or accelerometers as self-monitoring tools to modify a participant’s PA behavior. They also reported the use of websites, smartphones, and tablets to check and record participants’ PA information. For one primary study they report the use of the self-efficacy theory.
Schaffer et al. [83] included primary studies in which the interventions focused on promoting exercise, defined as an intentional, structured, and repetitive activity aimed at improving physical fitness. Pedometers and accelerometers were used for self-monitoring during the exercise interventions.
Singh et al. [84] included primary studies that aimed to improve PA using pedometers or other digital activity trackers with embedded accelerometers (e.g., Fitbit, Polar, and Garmin). The authors reported uses of the theory of planned behavior (six primary studies), the transtheoretical model combined with social cognitive theory (three primary studies), the social cognitive theory (three primary studies), the self-determination theory (one primary study), the health action process approach (one primary study), a combination of social cognitive theory, theory of planned behavior, and transtheoretical model, as well as motivational interviewing (one primary study), only the transtheoretical model (one primary study), only motivational interviewing (one primary study), and a combination of multiple theories, such as the I-Change model with social cognitive theory (one primary study).
Remote interventions (websites or apps) using various components of behavioral support for PA promotion via digital facilities (smartphones, websites, email, etc.), but without digital activity trackers
Electronic communications and information technologies, such as websites, email, SMS, and smartphones, have been noted in reviews under this category to educate participants, control PA adherence, receive feedback from professionals, and deliver information. In this category of interventions, we sometimes observed the use of digital activity trackers when they were only used as a tool to objectively measure PA.
Of the seven reviews, two [86, 88] focused on remote interventions to promote PA among individuals with major NCDs. Both reviews reported different interventional components, such as computer-assisted sessions with a coach, tailored feedback/reminders, informative booklets, and smartphone apps. In addition, only Kongstad et al. [88] outlined the motivational components of the interventions. Kongstad et al. [88] asserted that a few of the interventions were in addition to usual or standard care. None of the reviews contained information regarding the setting of the intervention (group-based versus home-based). Furthermore, only Pfaeffli Dale et al. [86] outlined the theoretical basis of the interventions. In Kongstad et al. [88] review, the authors included primary studies of interventions using remote feedback about the participant’s PA behavior for the purpose of PAP. For this, the authors reported the use of text-based feedback via webpages, email, and SMS. In Pfaeffli Dale et al. [86] review, the interventions were delivered through various digital remote technologies. Additionally, the transtheoretical model (one primary study), and self-efficacy theory (one primary study) were used in the interventions’ designs.
Methodological quality assessment
Seven reviews underwent quality assessments using AMSTAR-2 [69]. Details are presented in Table 2.
The overall quality of the reviews ranged from critically low to low. Four of the seven reviews [83, 85, 87, 89] were rated as having critically low quality due to multiple critical flaws and non-critical weaknesses. Three of the seven reviews [84, 86, 88] were rated as having low quality due to one critical flaw and non-critical weaknesses.
All the included reviews developed research questions and inclusion criteria based on the components of PICOS. They also provided explanations for their selection of study designs for the inclusion criteria. None of the reviews reported the source of funding for the primary studies. Data extraction was performed in duplicate in all reviews except for one [85]. Similarly, all reviews except one [83] used a satisfactory or partially satisfactory technique to assess ROB in the individual primary studies included in the review. Furthermore, all reviews except one [89] provided satisfactory explanations and discussions of any observed heterogeneity in the results.
Internal validity and certainty of evidence of the primary studies included in the reviews
Two of the seven reviews [87, 89] used the PEDro scale to assess the methodological quality of the primary studies. The mean (± SD) PEDro scores reported in these reviews were 6.3 ± 0.3 points and 9.29 ± 1 points, respectively, which were interpreted as having good and excellent methodological quality [90], respectively. Four of the seven reviews [84,85,86, 88] used the Cochrane Collaboration ROB assessment tool [63] to assess ROB, and one review [83] did not perform any assessment of internal validity.
Considering that four of the seven reviews used the Cochrane Collaboration ROB assessment tool, it can be summarized that in all four reviews, the included primary studies had low ROB in random sequence generation (RSG). Three out of four of these reviews reported low ROB in allocation concealment (AC) and incomplete outcome data (IOD) of their included primary studies. However, more than half of the reviews included primary studies with high ROB in blinding of participants and personnel (BPP) and selective outcome reporting (SOR). The ROBs varied across primary studies regarding blinding of outcome assessments.
The review by Pfaeffli Dale et al. [86] also used the Jadad-scale to assess internal validity, reporting that only a few primary studies were judged as having high quality (4 out of 5 points).
Only one review [88] assessed the certainty of evidence using GRADE. In this review, the certainty of evidence was downgraded one step as a result of substantial inconsistency. It was downgraded a further step as a result of imprecision in the estimate, ranging from low to moderate effect, in addition to serious ROB. The overall certainty of evidence in this review was graded as low for overall PA level as an outcome.
Primary studies overlap within the included systematic review
The seven reviews included 121 primary studies with PA assessments as an outcome. A total of 110 primary studies (without overlap) were included across all seven reviews. Five of the seven [83,84,85, 87, 89] were related to interventions in which activity trackers were the main component of a PAP program. The two remaining reviews [86, 88] were related to remote interventions via digital means for PAP. A matrix (see Additional file 5) with 110 rows (single primary studies) and seven columns (included reviews) was created. The CCA percentage across the entire matrix to map overlap among all the reviews was 1.666%, which indicated a slight overlap.
The calculated CCA percentage among five reviews for the category of digital activity trackers was 3.086%, a result that was judged as slightly overlapping. In the same way, the CCA for the two reviews related to remote interventions was calculated as 0%, indicating no overlap between the two reviews. For two reviews [83, 84], the calculated CCA percentage (25.714%) showed a very high overlap. Since these reviews were not in the same subgroup analyses, both were retained in accordance with Step 2 of the method elaborated by Hennessy, Johnson [76].
Summary of the reported effects
Interventions based on the use of digital activity trackers for self-monitoring of PA as the main component within either remote or non-remote interventions
Additional file 6 presents the details for a summary of the effects. Five of the reviews [83,84,85, 87, 89] reported the efficacy of interventions based on the use of digital activity trackers. In three out of these reviews [84, 85, 87], meta-analysis was performed, while qualitative synthesis was conducted in the other two reviews [83, 89].
Overall, these interventions demonstrated a positive impact on PAP among individuals with major NCDs. Nine meta-analyses were reported across three reviews of this category. Four meta-analyses reported effects on subjectively measured PA (moderate effect, n = 1; large effect, n = 1; no effect (non-significant decrease), n = 2), four to objectively measured PA (moderate effect, n = 3; large effect, n = 1), and one referred to mixed subjective and objective PA measuring (moderate effect). In addition, four vote counting based on direction of effect was performed for two reviews, of which two referred to subjective PA measurements (both generally effective), and the others two referred to objective PA measurements (mixed effect, n = 1; generally effective n = 1). However, an effect could only be confirmed in two cases using the sign test.
In the review by Allet et al. [89], three and eleven primary studies reported subjectively and objectively measured PA, respectively. The use of digital activity trackers for self-monitoring on PAP was classified as “generally effective,” with two of three primary studies favoring the interventions (67%; 95%-CI: [21%, 94%]). However, no sign test could be performed because of the low number of primary studies reporting subjectively measured PA (n < 6); therefore, we were unable to confirm that there was evidence of an effect. All three primary studies were judged as studies with high methodological quality (see Additional file 7 for effect direction plots and vote-counting details). For objectively measured PA, there was evidence that interventions based on the use of digital activity trackers for the self-monitoring of PA had an effect on PAP, with 10 of 11 primary studies favoring the intervention (91%; 95%-CI: [62%, 98%]; p = 0.0117). Seven of 11 primary studies were judged as high methodological quality studies, while three of 11 primary studies were judged as studies with fair methodological quality (see Additional file 7 for effect direction plot and vote-counting details).
In the review by Armstrong et al. [87], there was evidence that interventions based on pedometers had a moderate effect on objectively measured PA (daily steps) versus interventions implementing usual care (SMD = 0.53; 95%-CI: 0.29–0.77; p < 0.00001; methodological quality: Excellent). Sub-group analysis provided evidence of an effect on the daily steps for the use of pedometers in addition to pulmonary rehabilitation in comparison to pulmonary rehabilitation alone (SMD = 0.51; 95%-CI: 0.13–0.88; p = 0.006; methodological quality: Excellent).
In the review by Kanejima et al. [85], there was evidence that self-monitoring interventions via pedometers and accelerometers had a large effect on improving objectively measured PA compared to control groups that did not use digital activity trackers but employed usual care, or a cardiac rehabilitation program with the same exercise sessions, or only received PA recommendations (SMD = 0.97; 95%-CI: 0.71–1.22; p < 0.01; unclear ROB).
In the review by Schaffer et al. [83] nine and five primary studies reported subjectively and objectively measured PA, respectively. Concerning subjectively measured PA, there was evidence that interventions based on the use of digital activity trackers for self-monitoring of PA had an effect on PAP, with nine primary studies favoring the intervention (100%; 95%-CI: [70%, 100%]; p = 0.0039) (see Additional file 7 for effect direction plot and vote-counting details). For objectively measured PA, there were “mixed effects” on PA for the use of digital activity trackers for self-monitoring, with three of the five primary studies favoring the intervention (60%; 95%-CI: [23%, 88%]). Furthermore, no sign test could be performed because of the low number of primary studies reporting on objectively measured PA (n < 6). No methodological quality/ROB assessment was reported for the primary studies included in this review. See Additional file 7 for effect direction plot and vote-counting details.
In the review by Singh et al. [84], there was evidence that interventions based on pedometers and other activity trackers in addition to other interventional components (such as counseling) had a large effect on subjectively measured duration of moderate-intensity PA (SMD = 0.87; 95%-CI: 0.43–1.32; p < 0.05; high ROB), a moderate effect on subjectively measured duration of moderate-to vigorous-intensity PA (SMD = 0.61; 95%-CI: 0.36–0.86; p < 0.05; high ROB), on objectively and subjectively measured total PA (SMD = 0.62; 95%-CI: 0.39–0.84; p < 0.05; high ROB), and on objectively measured daily steps (SMD = 0.54; 95%CI: 0.30–0.78, p < 0.05; high ROB) compared to non-DIs. However, no effect was found on subjectively measured duration of low-intensity PA (SMD = 0.05; 95%-CI: -0.12–0.22; p = 0.54; high ROB) or subjectively measured duration of vigorous-intensity PA (SMD = 0.36; 95%-CI: -0.04–0.77; p = 0.08; high ROB).
Remote interventions (websites or apps) using various components of behavioral support for PA promotion via digital facilities (smartphones, websites, email, etc.) but without digital activity trackers
Two out of seven reviews [86, 88] reported the efficacy of remote interventions using various components of behavioral support via digital facilities for PA promotion. One of the reviews [88] performed meta-analysis. In addition, one vote count based on direction of effect for subjective PA measurement was performed for the Pfaeffli Dale et al. [86] review.
In the review by Kongstad et al. [88], there was evidence that remote feedback intervention via digital facilities had a small effect (SMD = 0.33; 95%-CI: 0.17–0.49; p = 0.015; certainty of evidence: low) in comparison to standard treatment. Five of the primary studies differed from the usual treatment by including remote feedback on PA, while all other components remained identical. The other 22 primary studies included additional intervention components (such as diet hints or social support) to the remote feedback. The meta-regression analysis showed a non-significant decrease in effect size for primary studies in which the only difference was the implementation of remote feedback. (SMD = -0.164; 95%-CI: -0.703–0.374; p = 0.536; certainty of evidence: low; high ROB).
In the review by Pfaeffli Dale et al. [86], two primary studies used remote interventions with various components of behavioral support for PAP. The remote interventions were classified as “generally effective,” as both primary studies showed improvement of subjectively measured PA (100%; 95%-CI: [34.24%, 100%]). As only two primary studies were too few for the sign test, we were unable to confirm the evidence of an effect. Both studies were rated as high methodological quality studies (see Additional file 7 for effect direction plot and vote-counting details).
Discussion
In this overview of reviews we aimed at evaluating the efficacy of DIs on PA among individuals with major NCDs. Our findings provide some evidence that the use of certain types of DIs can be an effective approach for PAP among this target group. While physical inactivity was considered one of the main risk factors, it was shown that different types of DI can promote PA to manage and prevent major NCDs. To the best of our knowledge, no overarching evaluation had been conducted in a single study to provide a holistic overview of the of different types of DI on PA in people with major NCDs. In previous studies, authors evaluated the efficacy of subcategories of DIs and NCD populations. By synthesizing data from single reviews limited to small proportions of DI or a narrow range of NCDs we were cautiously able to draw a conclusion on efficacy of two types of DIs on PAP.
According to our analysis, interventions based on the use of digital activity trackers show positive effects on subjective as well as objective PA measures in individuals suffering from major NCDs. This finding is consistent with previous reviews in this field that have focused on adults [91] and on specific populations, such as individuals with CVDs [50] and COPD [34].
However, Alam et al. [92] reported that systematic reviews of interventions utilizing digital activity trackers to self-monitor PA showed variability in qualitative synthesis findings on PA measures among patients with CVDs; nevertheless, meta-analyses reported in this overview favored the DIs. Alam et al. [92] reported that the observed variability in the qualitative synthesis’s findings may be representative of insufficient rigorous difference assessment between intervention and control groups in terms of components used.
In the same way, our analysis provided some evidence that remote interventions via digital facilities show efficacy on PA (both subjective and objective PA measures) in individuals suffering from T2D and CVDs. This finding is in agreement with overviews focusing on individuals suffering from COPD [55], CVDs [54], or T2D [56] or on specific types of remote interventions, such as mobile text messaging or websites [60, 61] or apps [58, 93].
Our results suggest that the evidence regarding the efficacy of DIs to promote PA is fairly consistent among individuals with CVD, cancer, COPD, and T2D. However, the magnitude of effect varied across populations. Furthermore, there was no conclusive evidence for individuals with osteoarthritis due to a low number of primary studies.
Moreover, the results of the present overview are consistent with previous overviews of reviews evaluating the effects of DIs to promote PA in other populations. There is evidence that DIs can be effective to promote PA in both clinical (e.g. individuals with obesity, chronic pain) [52, 94,95,96], and healthy populations [58, 97].
Limitations
Even though a large number of reviews was retrieved in our search, only seven met the inclusion criteria. The inclusion of the diverse range of NCDs and DIs in this overview provides some evidence into the efficacy of these interventions. However, not all types of NCDs, such as obesity and depression, could be included in this overview because we restricted the search to the major NCDs [14, 65, 98]. In addition, identified reviews encompass digital technologies, such as electronic activity trackers and remote digital facilities (smartphones and apps, tablets, SMS, email, and web pages), while reviews including other types of digital technologies, such as virtual/augmented reality and digital gamification, were searched but did not meet our inclusion criteria.
While the included reviews provided some insights, it is essential to acknowledge some methodological considerations that might influence the interpretation of the findings. Diversity in the use of tools for assessing methodological quality and ROB made it difficult to draw conclusions about the internal validity of primary studies. Moreover, only one review reported the certainty of evidence, which is crucial in translating research findings into action. This overview of reviews was limited to published systematic reviews in English and German, and including reviews published in other languages might have changed the nature of the findings.
Additionally, only systematic reviews of RCTs were included in this overview, and more holistic results may be achieved by covering other forms of reviews (e.g., short or rapid reviews) and their included trials (non-randomized, non-controlled, or pre-post design). In addition, because of the diversity in PICOS elements, meta-analysis as a more powerful method of data synthesis was not possible. Furthermore, vote counting based on the direction of the effect method [99] could not provide information on the magnitude of the effect in all cases.
Furthermore, in both identified DIs categories, the interventions not only applied digital technologies but also used non-DI components in their implemented programs (e.g., counseling, motivational interviewing, diet, etc.; see Additional file 6). Therefore, these additional components limit our ability to attribute the causality of benefits to the digital technologies used rather than to the overall intervention. Finally, the methodological quality assessment via AMSTAR-II of the included reviews in this overview showed overall qualities ranging from critically low to low, which may cast doubt on the results. By increasing the availability of reviews with higher methodological quality, the certainty of the results may be strengthened.
Besides, review’s authors reported some more limitations about the review methodology and included primary studies. The majority of reviews reported that the literature search was conducted in English, so publishing bias may have happened due to excluding non-English primary studies. As well, most of the reviews reported heterogeneity regarding outcomes measurement, population, and content of interventions in the primary studies. In addition, some of the reviews conducted the screening of records or data extraction by a single researcher rather than in duplicate. Detailed limitations of each review are provided in Additional file 8.
Implication for clinical practice
From a practical standpoint, healthcare professionals and policy makers can benefit from the insights provided by this study. Digital approaches providing tailored, scalable, and cost-efficient solutions [29,30,31,32,33,34,35,36] have the potential to minimize some barriers against PAP among individuals with major NCDs. Some barriers such as hardships in reaching the site of PA and unfavorable weather conditions, and lack of time [22] can be attenuated by use of the remote interventions to distance-delivery of contents, and providing participants with counseling, motivational interviewing and reminders via digital facilities such as online platforms, apps, and SMS instead of person-to-person implementation.
Furthermore, some psychological barriers such as self-monitoring problems [22], can be reduced by implementing interventions based on the use of activity trackers as self-monitoring tool. Incorporating these interventions into clinical practice could enhance patient engagement and support disease management. However, integrating these technologies into existing healthcare systems requires careful consideration of factors such as data security [100] and the training of healthcare professionals [101].
Furthermore, the majority of the individuals with major NCDs in this overview were over 50 years old. Any hardship during the presentation of such new technologies for this age group should be recognized and attenuated by providing them with support and an effective method of education [102]. The rapidly growing number of published systematic reviews on different types of DI and NCDs also makes it difficult for policy makers to make use of the evidence in this field. Our overview approach, which synthesized a broad range of data, may help policy makers to design feasible and effective action plans for PAP when conventional interventions face obstacles.
Implication for further research
While our study has shed light on the efficacy of DIs in PAP among individuals with major NCDs, there remain several areas that require further investigation. The diversity of DIs warrants more in-depth exploration. This study primarily focused on interventions based on the use of digital activity trackers for self-monitoring PA and remote interventions via digital facilities. However, emerging technologies, such as virtual/augmented reality and digital gamification (e.g., exergames and console-based video games), hold the potential for enhancing engagement and sustaining long-term PA behavior change [103, 104].
In addition, the methodological quality of the included reviews varied. The reviews demonstrated critical flaws, highlighting the need for more rigorous and transparent conducting and reporting of systematic review methodologies on this topic. In addition, to further advance the field, future research should delve into the comparative analysis of the efficacy of various types of DIs. Comparisons between different components of interventions, such as theory basis, educational content, and especially technologies and their applications, such as smartphone apps, wearable devices, virtual/augmented reality, and exergames, can elucidate the most effective approaches for specific populations of NCDs.
In addition, we realized that only a few of the behavioral components in the DIs were developed on a theoretical basis. As various behavioral change theories have been discussed in the field of PAP [105, 106] further research should identify the types of DIs that are compatible with behavior change theories and determine how BCTs can be integrated within the DIs. For instance, Yang et al. [107] showed that the majority of implementation of PA promoting interventions via mobile apps favored the use of BCTs with modest evidence bases rather than BCTs with higher evidence of efficacy.
In another study, Mercer et al. [108] categorized the BCTs used in various digital activity trackers. They revealed that, for example, BCTs related to planning of PA, or the reduction of negative feelings (e.g., fear) to perform PA, were absent in design and use of activity trackers, while BCTs providing information were the most common. Furthermore, BCTs presenting instructions on how to concretely perform PA were scarce in design and use of activity trackers. In the same way, Schroé et al. [109] showed that differences in BCT combinations cause differences in the efficacy of DIs aiming at PAP. For example, action planning always showed more efficacy in PAP when it was combined with coping planning in e- and m-health interventions.
Moreover, the socio-cultural context and its impact on DIs cannot be overlooked. The findings of this study focused primarily on populations in developed countries, and future research should investigate the applicability and cultural adaptability of these interventions in diverse settings. In addition, it seems essential to determine the safety aspects of DI application, as some non-serious adverse events have been reported in the use of DIs to improve PA among patients with chronic conditions [110].
Finally, more evidence is needed on effects of DIs on physical function and physical fitness, as well as on sedentary behavior. Thus, further overviews of reviews are needed to address these issues that could not be implemented in our study (please see Additional file 1).
Conclusion
The findings of this overview suggest that some types of DIs, such as self-monitoring with digital activity trackers and remote interventions via digital facilities, may be effective means of promoting PA across major NCDs. The findings should be interpreted cautiously since the methodological quality of included reviews ranged from critically low to low. Additionally, there was no homogenous assessment for the certainty of evidence. Further systematic reviews are required on the efficacy of DIs with more rigorous conducting and reporting of systematic review methodologies.
Availability of data and materials
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Abbreviations
- NCD:
-
Noncommunicable disease
- CVD:
-
Cardiovascular disease
- T2D:
-
Type 2 diabetes
- PA:
-
Physical activity
- DI:
-
Digital intervention
- PAP:
-
Physical activity promotion
- BCT:
-
Behavior change technique
- COPD:
-
Chronic obstructive pulmonary disease
- PRIOR:
-
Preferred Reporting Items for Overviews of Reviews
- PICOS:
-
Population, intervention, comparison, outcomes, and study design
- RCT:
-
Randomized controlled trial
- ROB:
-
Risk of bias
- AMSTAR-2:
-
A MeaSurement Tool to Assess systematic Reviews
- GRADE:
-
Grading of Recommendations Assessment, Development, and Evaluation
- CCA:
-
Corrected cover area
- CI:
-
Confidence interval
- SMD:
-
Standardized mean difference
- SMS:
-
Short Message Service
- RSG:
-
Random sequence generation
- AC:
-
Allocation concealment
- IOD:
-
Incomplete outcome data
- BPP:
-
Blinding of participants and personnel
- SOR:
-
Selective outcome reporting
References
WHO: Global health estimates 2020: deaths by cause, age, sex, by country and by region, 2000–2019. https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (2020). Accessed.
WHO. Global status report on noncommunicable diseases 2014. vol WHO/NMH/NVI/15.1. Geneva: World Health Organization; 2014.
Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–223.
Naghavi M, Abajobir AA, Abbafati C, Abbas KM, Abd-Allah F, Abera SF, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1151–210.
WHO: Noncommunicable diseases. 2019. Available at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases. Accessed 14 Mar 2024.
Vandenberghe D, Albrecht J. The financial burden of non-communicable diseases in the European Union: a systematic review. Eur J Public Health. 2020;30(4):833–9.
Azadnajafabad S, Mohammadi E, Aminorroaya A. et al. Non-communicable diseases’ risk factors in Iran; a review of the present status and action plans. J Diabetes Metab Disord; 2021. https://doi.org/10.1007/s40200-020-00709-8.
Finland S: Official Statistics of Finland (OSF): Causes of death, Accessed 3 March 2024, available at http://www.stat.fi/til/ksyyt/2020/ksyyt_2020_2021-12-10_tie_001_en.html. (2021). Accessed.
Dhimal M, Karki KB, Sharma SK, Aryal KK, Shrestha N, Poudyal A, et al. Prevalence of selected chronic non-communicable diseases in Nepal. J Nepal Health Res Counc. 2019;17(3):394–401.
Rahim HFA, Sibai A, Khader Y, Hwalla N, Fadhil I, Alsiyabi H, et al. Non-communicable diseases in the Arab world. Lancet. 2014;383(9914):356–67.
Bigna JJ, Noubiap JJ. The rising burden of non-communicable diseases in sub-Saharan Africa. Lancet Glob Health. 2019;7(10):e1295–6.
Muka T, Imo D, Jaspers L, Colpani V, Chaker L, van der Lee SJ, et al. The global impact of non-communicable diseases on healthcare spending and national income: a systematic review. Eur J Epidemiol. 2015;30:251–77.
Purnamasari D. The emergence of non-communicable disease in Indonesia. Acta Med Indones. 2019;50(4):273.
Wagner K-H, Brath H. A global view on the development of non communicable diseases. Prev Med. 2012;54:S38–41.
Katzmarzyk PT, Friedenreich C, Shiroma EJ, Lee I-M. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br J Sports Med. 2022;56(2):101–6.
Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1· 9 million participants. Lancet Global Health. 2018;6(10):e1077–86.
Pedersen BK, Saltin B. Exercise as medicine–evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. 2015;25:1–72.
WHO. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. Geneva: WHO Document Production Services; 2013.
Conn VS, Hafdahl AR, Brown SA, Brown LM. Meta-analysis of patient education interventions to increase physical activity among chronically ill adults. Patient Educ Couns. 2008;70(2):157–72.
Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet. 2012;380(9838):272–81.
Sallis JF, Floyd MF, Rodríguez DA, Saelens BE. Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation. 2012;125(5):729–37.
Cavallo M, Morgana G, Dozzani I, Gatti A, Vandoni M, Pippi R, et al. Unraveling Barriers to a Healthy Lifestyle: Understanding Barriers to Diet and Physical Activity in Patients with Chronic Non-Communicable Diseases. Nutrients. 2023;15(15):3473.
Meskó B, Drobni Z, Bényei É, Gergely B, Győrffy Z. Digital health is a cultural transformation of traditional healthcare. Mhealth. 2017;3.
Sullivan AN, Lachman ME. Behavior change with fitness technology in sedentary adults: a review of the evidence for increasing physical activity. Front Public Health. 2017;4:289.
Natalucci V, Marmondi F, Biraghi M, Bonato M. The Effectiveness of Wearable Devices in Non-Communicable Diseases to Manage Physical Activity and Nutrition: Where We Are? Nutrients. 2023;15(4):913.
Marcus B, Owen N, Forsyth L, Cavill N, Fridinger F. Physical activity interventions using mass media, print media, and information technology. Am J Prev Med. 1998;15(4):362–78.
Lewis BA, Napolitano MA, Buman MP, Williams DM, Nigg CR. Future directions in physical activity intervention research: expanding our focus to sedentary behaviors, technology, and dissemination. J Behav Med. 2017;40(1):112–26. https://doi.org/10.1007/s10865-016-9797-8.
Herold F, Theobald P, Gronwald T, Rapp MA, Müller NG. Going digital–a commentary on the terminology used at the intersection of physical activity and digital health. Eur Rev Aging Phys Act. 2022;19(1):17.
Rose T, Barker M, Jacob CM, Morrison L, Lawrence W, Strömmer S, et al. A systematic review of digital interventions for improving the diet and physical activity behaviors of adolescents. J Adolesc Health. 2017;61(6):669–77.
Western MJ, Armstrong ME, Islam I, Morgan K, Jones UF, Kelson MJ. The effectiveness of digital interventions for increasing physical activity in individuals of low socioeconomic status: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2021;18(1):1–21.
Stockwell S, Schofield P, Fisher A, Firth J, Jackson SE, Stubbs B, et al. Digital behavior change interventions to promote physical activity and/or reduce sedentary behavior in older adults: A systematic review and meta-analysis. Exp Gerontol. 2019;120:68–87. https://doi.org/10.1016/j.exger.2019.02.020.
De Santis KK, Jahnel T, Matthias K, Mergenthal L, Al Khayyal H, Zeeb H. Evaluation of digital interventions for physical activity promotion: Scoping review. JMIR Public Health Surveill. 2022;8(5): e37820.
Blount DS, McDonough DJ, Gao Z. Effect of Wearable Technology-Based Physical Activity Interventions on Breast Cancer Survivors’ Physiological, Cognitive, and Emotional Outcomes: A Systematic Review. J Clin Med. 2021;10(9):2015. https://doi.org/10.3390/jcm10092015.
Qiu S, Cai X, Wang X, He C, Zuegel M, Steinacker JM, et al. Using step counters to promote physical activity and exercise capacity in patients with chronic obstructive pulmonary disease: a meta-analysis. Ther Adv Respir Dis. 2018;12:1753466618787386.
Douma JA, Verheul HM, Buffart LM. Feasibility, validity and reliability of objective smartphone measurements of physical activity and fitness in patients with cancer. BMC Cancer. 2018;18:1–7.
Martínez-García MDM, Ruiz-Cárdenas JD, Rabinovich RA. Effectiveness of Smartphone Devices in Promoting Physical Activity and Exercise in Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review. COPD J Chron Obstructive Pulm Dis. 2017;14(5):543–51. https://doi.org/10.1080/15412555.2017.1358257.
Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008;27(3):379.
Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med. 2013;46(1):81–95.
Cooper JO, Heron TE, Heward WL. Applied behavior analysis (2 nd edition). J Appl Behav Anal. 2010;43(1):161–74.
Sanders JP, Loveday A, Pearson N, Edwardson C, Yates T, Biddle SJ, et al. Devices for self-monitoring sedentary time or physical activity: a scoping review. J Med Int Res. 2016;18(5): e90.
Page EJ, Massey AS, Prado-Romero PN, Albadawi S. The use of self-monitoring and technology to increase physical activity: A review of the literature. Perspect Behav Sci. 2020;43:501–14.
WHO. Telemedicine: opportunities and developments in member states. Report on the second global survey on eHealth. Geneva: World Health Organization; 2010.
Williams AM, Gift TL. Remote Health Interventions: Effectiveness, Cost, and Cost-Effectiveness Considerations. Sex Transm Dis. 2022;49(11S):S15–7.
Opdenacker J, Delecluse C, Boen F. A 2-year follow-up of a lifestyle physical activity versus a structured exercise intervention in older adults. J Am Geriatr Soc. 2011;59(9):1602–11.
Rogers LQ, Markwell SJ, Verhulst S, McAuley E, Courneya KS. Rural breast cancer survivors: exercise preferences and their determinants. Psycho-Oncol J Psychol Soc Behav Dimens Cancer. 2009;18(4):412–21.
Eng L, Pringle D, Su J, Shen X, Mahler M, Niu C, et al. Patterns, perceptions, and perceived barriers to physical activity in adult cancer survivors. Support Care Cancer. 2018;26:3755–63.
Stavric V, Kayes NM, Rashid U, Saywell NL. The effectiveness of self-guided digital interventions to improve physical activity and exercise outcomes for people with chronic conditions: a systematic review and meta-analysis. Front Rehabil Sci. 2022;3: 925620.
Palmer M, Sutherland J, Barnard S, Wynne A, Rezel E, Doel A, et al. The effectiveness of smoking cessation, physical activity/diet and alcohol reduction interventions delivered by mobile phones for the prevention of non-communicable diseases: A systematic review of randomised controlled trials. PLoS ON. 2018;13(1):e0189801. https://doi.org/10.1371/journal.pone.0189801.
Mair JL, Salamanca-Sanabria A, Frese B, Jakob R, Kowatsch T, Haug S. Effective behavior change techniques in digital health interventions targeting non-communicable diseases: an umbrella review. OSF Preprints. 2023(Web).
Gold N, Yau A, Rigby B, Dyke C, Remfry EA, Chadborn T. Effectiveness of Digital Interventions for Reducing Behavioral Risks of Cardiovascular Disease in Nonclinical Adult Populations: Systematic Review of Reviews. J Med Int Res. 2021;23(5): e19688. https://doi.org/10.2196/19688.
Akinosun AS, Polson R, Diaz-Skeete Y, De Kock JH, Carragher L, Leslie S, et al. Digital Technology Interventions for Risk Factor Modification in Patients With Cardiovascular Disease: Systematic Review and Meta-analysis. JMIR Mhealth Uhealth. 2021;9(3): e21061. https://doi.org/10.2196/21061.
Ferguson T, Olds T, Curtis R, Blake H, Crozier AJ, Dankiw K, et al. Effectiveness of wearable activity trackers to increase physical activity and improve health: a systematic review of systematic reviews and meta-analyses. Lancet Digit Heal. 2022;4(8):e615–26.
Roberts A, Fisher A, Smith L, Heinrich M, Potts H, Roberts AL, et al. Digital health behaviour change interventions targeting physical activity and diet in cancer survivors: a systematic review and meta-analysis. J Cancer Survivorship. 2017;11(6):704–19. https://doi.org/10.1007/s11764-017-0632-1.
Shi W, Green H, Sikhosana N, Fernandez R. Effectiveness of telehealth cardiac rehabilitation programs on health outcomes of patients with coronary heart diseases: an umbrella review. J Cardiopulm Rehabil Prev. 2023;10(1097):15–25.
Koh JH, Chong LCY, Koh GCH, Tyagi S. Telemedical Interventions for Chronic Obstructive Pulmonary Disease Management: Umbrella Review. J Med Int Res. 2023;25: e33185.
Whittemore R, Siverly L, Wischik DL, Whitehouse CR. An umbrella review of text message programs for adults with type 2 diabetes. Diabetes Educ. 2020;46(6):514–26.
Qiu L, Ye M, Tong Y, Jin Y. Promoting physical activity among cancer survivors: an umbrella review of systematic reviews. Support Care Cancer. 2023;31(5):301.
Rodríguez-González P, Iglesias D, Fernandez-Rio J, Gao Z. Effectiveness of interventions using apps to improve physical activity, sedentary behavior and diet: An umbrella review. Complement Ther Clin Pract. 2022;101711:1–6.
Parisod H, Pakarinen A, Kauhanen L, Aromaa M, Leppanen V, Liukkonen TN, et al. Promoting children’s health with digital games: A review of reviews. Games Health. 2014;3(3):145–56. https://doi.org/10.1089/g4h.2013.0086.
Eze ND, Mateus C, Hashiguchi TCO. Telemedicine in the OECD: An umbrella review of clinical and cost-effectiveness, patient experience and implementation. PLOS ONE. 2020;15(8). https://doi.org/10.1371/journal.pone.0237585.
Hall AK, Cole-Lewis H, Bernhardt JM. Mobile Text Messaging for Health: A Systematic Review of Reviews. Annu Rev Public Health. 2015;36(1):393–415. https://doi.org/10.1146/annurev-publhealth-031914-122855.
Pollock M, Fernandes RM, Becker LA, Pieper D, Hartling L. Chapter V: overviews of reviews. Cochrane handbook for systematic reviews of interventions version. 2020;6.
Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. Chichester: John Wiley & Sons Ltd, The Atrium, Southern Gate; 2019.
Gates M, Gates A, Pieper D, Fernandes RM, Tricco AC, Moher D, et al. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ. 2022;378.
Geidl W, Schlesinger S, Mino E, Miranda L, Pfeifer K. Dose–response relationship between physical activity and mortality in adults with noncommunicable diseases: a systematic review and meta-analysis of prospective observational studies. Int J Behav Nutr Phys Act. 2020;17(1):1–18.
Burr J, Shephard R, Cornish S, Vatanparast H, Chilibeck P. Arthritis, osteoporosis, and low back pain: evidence-based clinical risk assessment for physical activity and exercise clearance. Can Fam Physician. 2012;58(1):59–62.
Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):646–56.
Bailey J, Murray E, Rait G, Mercer C, Morris R, Peacock R, et al. Computer-based interventions for sexual health promotion: systematic review and meta-analyses. Int J STD AIDS. 2012;23(6):408–13.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:1–9.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–21.
Corbett MS, Higgins JP, Woolacott NF. Assessing baseline imbalance in randomised trials: implications for the Cochrane risk of bias tool. Res Synth Methods. 2014;5(1):79–85.
Sterne JA, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:1–8.
Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1–12.
Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–94.
Pieper D, Antoine S-L, Mathes T, Neugebauer EA, Eikermann M. Systematic review finds overlapping reviews were not mentioned in every other overview. J Clin Epidemiol. 2014;67(4):368–75.
Hennessy EA, Johnson BT. Examining overlap of included studies in meta-reviews: Guidance for using the corrected covered area index. Res Synth Methods. 2020;11(1):134–45.
Cohen J. The concepts of power analysis. Statistical power analysis for the behavioral sciences. Hillsdale: Elrbaum; 1988. p. 1–17.
McKenzie JE, Brennan SE. Synthesizing and presenting findings using other methods, chapter 12. Cochrane handbook for systematic reviews of interventions. Chichester: John Wiley & Sons Ltd, The Atrium, Southern Gate. 2019. p. 321–47.
GraphPad. https://www.graphpad.com/quickcalcs/binomial1/ (2023). Accessed 2023.
Boon MH, Thomson H. The effect direction plot revisited: application of the 2019 Cochrane Handbook guidance on alternative synthesis methods. Res Synth Methods. 2021;12(1):29–33.
Brown LD, Cai TT, DasGupta A. Interval estimation for a binomial proportion. Stat Sci. 2001;16(2):101–33.
Weir MC, Ryan R, Mayhew A, Worswick J, Santesso N, Lowe D, et al. The Rx for Change database: a first-in-class tool for optimal prescribing and medicines use. Implement Sci. 2010;5(1):1–9.
Schaffer K, Panneerselvam N, Poh Loh K, Herrmann R, Kleckner IR, Dunne RF, et al. Systematic review of randomized controlled trials of exercise interventions using digital activity trackers in patients with cancer. J Natl Compr Cancer Netw. 2019;17(1):57–63. https://doi.org/10.6004/jnccn.2018.7082.
Singh B, Zopf EM, Howden EJ. Effect and feasibility of wearable physical activity trackers and pedometers for increasing physical activity and improving health outcomes in cancer survivors: A systematic review and meta-analysis. J Sport Health Sci. 2022;11(2):184–93.
Kanejima Y, Kitamura M, Izawa KP. Self-monitoring to increase physical activity in patients with cardiovascular disease: a systematic review and meta-analysis. Aging Clin Exp Res. 2019;31(2):163–73. https://doi.org/10.1007/s40520-018-0960-7.
Pfaeffli Dale L, Dobson R, Whittaker R, Maddison R. The effectiveness of mobile-health behaviour change interventions for cardiovascular disease self-management: A systematic review. Eur J Prev Cardiol. 2016;23(8):801–17. https://doi.org/10.1177/2047487315613462.
Armstrong M, Winnard A, Chynkiamis N, Boyle S, Burtin C, Vogiatzis I. Use of pedometers as a tool to promote daily physical activity levels in patients with COPD: A systematic review and meta-analysis. Eur Respir Rev. 2019;28(154). https://doi.org/10.1183/16000617.0039-2019.
Kongstad MB, Valentiner LS, Ried-Larsen M, Walker KC, Juhl CB, Langberg H. Effectiveness of remote feedback on physical activity in persons with type 2 diabetes: A systematic review and meta-analysis of randomized controlled trials. J Telemed Telecare. 2019;25(1):26–34. https://doi.org/10.1177/1357633X17733772.
Allet L, Knols RH, Shirato K, de Bruin ED. Wearable Systems for Monitoring Mobility-Related Activities in Chronic Disease: A Systematic Review. Sensors. 2010;10(10):9026–52. https://doi.org/10.3390/s101009026.
Cashin AG, McAuley JH. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J Physiother. 2019;66(1):59-.
Laranjo L, Ding D, Heleno B, Kocaballi B, Quiroz JC, Tong HL, et al. Do smartphone applications and activity trackers increase physical activity in adults? Systematic review, meta-analysis and metaregression. Br J Sports Med. 2021;55(8):422–32.
Alam S, Zhang M, Harris K, Fletcher LM, Reneker JC. The impact of consumer wearable devices on physical activity and adherence to physical activity in patients with cardiovascular disease: a systematic review of systematic reviews and meta-analyses. New Rochelle: Telemed e-Health; 2022.
Edwards D, Williams J, Carrier J, Davies J. Technologies used to facilitate remote rehabilitation of adults with deconditioning, musculoskeletal conditions, stroke, or traumatic brain injury: an umbrella review. JBI Evid Synth. 2022;20(8):1927–68. https://doi.org/10.11124/JBIES-21-00241.
Li C, Chen X, Bi X. Wearable activity trackers for promoting physical activity: A systematic meta-analytic review. Int J Med Inform. 2021;152. https://doi.org/10.1016/j.ijmedinf.2021.104487.
Longhini J, Marzaro C, Bargeri S, Palese A, Dell’Isola A, Turolla A, et al. Wearable devices to improve physical activity and reduce sedentary behaviour: an umbrella review. Sports Med Open. 2024;10(1):9.
Adamse C, Dekker-Van Weering MG, van Etten-Jamaludin FS, Stuiver MM. The effectiveness of exercise-based telemedicine on pain, physical activity and quality of life in the treatment of chronic pain: a systematic review. J Telemed Telecare. 2018;24(8):511–26.
Fiedler J, Eckert T, Wunsch K, Woll A. Key facets to build up eHealth and mHealth interventions to enhance physical activity, sedentary behavior and nutrition in healthy subjects–an umbrella review. BMC Public Health. 2020;20:1–21.
Habib SH, Saha S. Burden of non-communicable disease: global overview. Diabetes Metab Syndr Clin Res Rev. 2010;4(1):41–7.
Borenstein M, Hedges L, Rothstein H. Meta-analysis methods based on direction and p-values. Introduction to Meta-Analysis. Chichester, UK: John Wiley & Sons; 2009. p. 325–30.
Stoumpos AI, Kitsios F, Talias MA. Digital transformation in healthcare: technology acceptance and its applications. Int J Environ Res Public Health. 2023;20(4):3407.
Wootton R, Geissbuhler A, Jethwani K, Kovarik C, Person DA, Vladzymyrskyy A, et al. Long-running telemedicine networks delivering humanitarian services: experience, performance and scientific output. Bull World Health Organ. 2012;90:341–7.
McGarrigle L, Todd C. Promotion of physical activity in older people using mHealth and eHealth technologies: rapid review of reviews. J Med Int Res. 2020;22(12): e22201.
Ng Y-L, Ma F, Ho FK, Ip P, Fu K-w. Effectiveness of virtual and augmented reality-enhanced exercise on physical activity, psychological outcomes, and physical performance: a systematic review and meta-analysis of randomized controlled trials. Comput Hum Behav. 2019;99:278–91.
Peng W, Crouse JC, Lin J-H. Using active video games for physical activity promotion: a systematic review of the current state of research. Health Educ Behav. 2013;40(2):171–92.
Rhodes RE, McEwan D, Rebar AL. Theories of physical activity behaviour change: a history and synthesis of approaches. Psychol Sport Exerc. 2019;42:100–9.
Hagger MS, Chatzisarantis NL. An integrated behavior change model for physical activity. Exerc Sport Sci Rev. 2014;42(2):62–9.
Yang C-H, Maher JP, Conroy DE. Implementation of behavior change techniques in mobile applications for physical activity. Am J Prev Med. 2015;48(4):452–5.
Mercer K, Li M, Giangregorio L, Burns C, Grindrod K. Behavior change techniques present in wearable activity trackers: a critical analysis. JMIR Mhealth Uhealth. 2016;4(2): e4461.
Schroé H, Van Dyck D, De Paepe A, Poppe L, Loh WW, Verloigne M, et al. Which behaviour change techniques are effective to promote physical activity and reduce sedentary behaviour in adults: a factorial randomized trial of an e-and m-health intervention. Int J Behav Nutr Phys Act. 2020;17(1):1–16.
Zangger G, Bricca A, Liaghat B, Juhl CB, Mortensen SR, Andersen RM, et al. Benefits and Harms of Digital Health Interventions Promoting Physical Activity in People With Chronic Conditions: Systematic Review and Meta-Analysis. J Med Int Res. 2023;25: e46439.
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was not specifically funded.
Author information
Authors and Affiliations
Contributions
MK, KP and AJ contributed to study conceptualization and design. MK conducted the literature search. MK and SK conducted title/abstract and full text screening. MK and MI conducted the data extraction and methodological quality assessment, MK and AJ analyzed and interpreted the results. MK wrote the original manuscript draft. KP, AJ, and WG critically revised the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 2. Microsoft Word file. Search strategy. Full search strategy for all the databases.
44247_2024_97_MOESM3_ESM.docx
Additional file 3. Microsoft Word file. Reason for exclusion. Reasons for excluding records in the second stage of screening.
44247_2024_97_MOESM7_ESM.docx
Additional file 7. Microsoft Word file. Effect direction plot. Details of vote-counting and data analysis for reviews with narrative synthesis method.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kardan, M., Jung, A., Iqbal, M. et al. Efficacy of digital interventions on physical activity promotion in individuals with noncommunicable diseases: an overview of systematic reviews. BMC Digit Health 2, 40 (2024). https://doi.org/10.1186/s44247-024-00097-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s44247-024-00097-6