
Abstract
Continuous monitoring for immunosuppressive status, infection and complications are a must for kidney transplantation (KTx) recipients. Traditional monitoring including blood sampling and kidney biopsy, which caused tremendous medical cost and trauma. Therefore, a cheaper and less invasive approach was urgently needed. We thought that a breath test has the potential to become a feasible tool for KTx monitoring. A prospective-specimen collection, retrospective-blinded assessment strategy was used in this study. Exhaled breath samples from 175 KTx recipients were collected in West China Hospital and tested by online ultraviolet photoionization time-of-flight mass spectrometry (UVP-TOF–MS). The classification models based on breath test performed well in classifying normal and abnormal values of creatinine, estimated glomerular filtration rate (eGFR), blood urea nitrogen (BUN) and tacrolimus, with AUC values of 0.889, 0.850, 0.849 and 0.889, respectively. Regression analysis also demonstrated the predictive ability of breath test for clinical creatinine, eGFR, BUN, tacrolimus level, as the predicted values obtained from the regression model correlated well with the clinical true values (p < 0.05). The findings of this investigation implied that a breath test by using UVP-TOF–MS for KTx recipient monitoring is possible and accurate, which might be useful for future clinical screenings.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Kidney transplantation (KTx) is the optimal treatment for end-stage kidney disease (ESKD) [1], offering significantly improved quality of life and reduced mortality risk compared to dialysis [2,3,4]. However, KTx recipients require ongoing monitoring due to the sophisticated immunosuppressive regimens they are on, which make them susceptible to infection, cancer, and cardiovascular disease (CVD) [5]. Additionally, individuals with underlying ESKD often have numerous comorbidities that require close monitoring [6].
After the first 3 to 6 months post-transplant, KTx patients are typically seen by general nephrologists or internists who may also handle their comorbidities, depending on the availability of resources near the patient [5]. While transplant nephrologists should be involved in the care of KTx patients for the duration of the graft, limited resources often make this difficult to achieve. Many transplant centers are located in large cities, making it inconvenient for a significant portion of KTx recipients to access. Additionally, the evaluation of new ESKD patients who require KTx and the management of post-transplant complications can be time-consuming for transplant nephrologists. Some tests are only available in special transplant centers, which can result in KTx recipients having to travel long distances, leading to unforeseen consequences [7]. Hence, there is an urgent need for a convenient and accurate screening tool that can be used for monitoring KTx recipients.
Conventional monitoring approaches, including blood sampling and kidney biopsy, are both invasive, resources-intensive, and pose risks of infection and bleeding. These risks can be life-threatening and cause significant burden to KTx recipients. As a result, less or non-invasive and more economical approaches have emerged [8]. Currently, there are three commercially available diagnostic kits are available on the market: CareDx's AlloSure and Natera's Prospera identify donor-derived cell-free DNA (dd-cfDNA) in blood, and Transplant Genomics' Trugraf identifies differentially expressed genes [9, 10]. However, each of these tests still requires blood sampling and costs approximately $3000 per test, moreover, their efficacy has yet to be validated [11].
Compared to sampling the interior environment sampling such as blood, the exterior environment may provide a more comprehensive picture of an organism's overall status. At the onset of a disease, the excess water, salt, electrolyte, proteins, DNAs, and RNAs are excreted into the exterior environment to maintain homeostatic balance [12]. In this circumstance, sampling the interior environment might miss early signals or markers [13]. Thus, the exterior environment, which allows for early detection, has advantages for advantages for identifying biomarkers to monitor KTx recipients. Exhaled breath and urine are the most available resources for noninvasive biomarkers. Exhaled breath, in comparison to urine, is more convenient and easier to obtain.
Human exhaled breath is composed mainly of nitrogen, oxygen, carbon dioxide, water vapor, volatile organic compounds (VOCs), and other inert gases. Among these, VOCs are considered a representative of body metabolic status because most of them are synthesized by the human body [14]. In the 1970s, Pauling et al. used gas chromatography technology to examine VOCs from exhaled human breath [14]. They found that approximately 200 VOCs existed within exhaled human breath [14]. Since then, VOC changes have been tested as biomarkers for several different diseases. For example, Rowland et al. tested 10 type I diabetic mellitus patients who exhaled breath and identified 100 significant VOCs. They also claimed that the VOC methyl nitrate could be used as a predictor of blood glucose [15]. Other reports also claimed that VOCs can be used to diagnose lung cancer and breast cancer [16, 17]. Although VOC examination has many advantages, major issues still need to be addressed. First, there is a lack of unified and standardized analysis methods cross different facilities, which can lead to different results for the same issue. Second, there is a lack of simple and efficient techniques for the effective separation and identification of VOCs in exhaled breath samples. Compared with chemical tests that are already widely used in blood and urine analysis, the current basic instruments for exhaled breath analysis (e.g., mass spectrometry) are more complex and require specialized operators. Third, the physiological significance and metabolic pathways of many VOCs in exhaled breath are still unclear, and one VOC may respond to several disease states. This metabolic uncertainty hinders the application of exhaled breath analysis to real clinical practice.
Overall, KTx recipients need constant kidney function monitoring and traditional methods are far from meeting the current need. Therefore, despite these above limitations, we hypothesized that a machine capable of non-invasively, easily and conveniently collecting and analyzing VOCs could significantly contribute to the monitoring of post-transplantation KTx recipients. In our current study, we used real-time online ultraviolet photoionization time-of-flight mass spectrometry (UVP-TOF–MS) to analyze VOCs in exhaled breath, which proved to be a feasible and noninvasive monitoring device for KTx recipients.
Results
Study overview and baseline characteristics
Of all the 175 KTx participants, 120 (69%) were male, with a mean (SD) age of 34.4 (± 10.6) years. All recipients were confirmed as KTx recipients by validation with Chinese Transplantation Registrations, and all samples were randomly allocated to the discovery (70%) and validation (30%) data sets. Table 1 showed the baseline characteristics of all eligible participants. The majority of KTx recipients were of Han nationality (84%). The overall body weight index was 20.9 (± 3.0). The median dialysis duration before KTx was 30.8 (± 32.2) months. The KTx recipients also included ABO-incompatible KTx and sensitized recipients, and all causes leading to end-stage renal disease were also included. The majority of KTx recipients received triple immunosuppressive therapy, including tacrolimus, mycophenolate mofetil, and steroids. In general, the KTx recipients who participated in the current study may represent the general KTx recipient population.
UVP-TOF–MS exhibited satisfying efficacy in exhaled breath tests
All people who we approached to join in the study agreed to participate the test, resulting in a 100% patient acceptance rate, and we were able to successfully collect samples from every single KTx recipient. No negative effects or discomforts were observed while collecting breath samples. Peaks with m/z < 29 and > 300 were excluded from the data analysis due to their low content. The mass spectrum (m/z 29 ~ 300) of breath sample was shown in Fig. 1. Each mass spectra were accumulated for 50 s, and it only took 1 min to detect each sample.

Flow diagram of study design
UVP-TOF–MS is a promising tool for identifying malfunctioning kidney transplant recipients.
As a screening tool, the primary objective was to identify abnormal situations from normal ones. Therefore, we developed a series of classification models based on exhaled VOCs. For KTx recipients, kidney function was the primary concern. Serum creatinine (SCr), estimated glomerular filtration rate (eGFR), and blood urea nitrogen (BUN) were the most commonly used clinical parameters for kidney function.
The SCr threshold was set at 108 µmol/L, and values below 108 µmol/L were considered normal. In the enrolled population of this study, there were 46 subjects with normal SCr values and 129 subjects with abnormal values. By using 200% SMOTE resampling to produce a balanced dataset (138 normal-129 abnormal), we generated a classification model with 70% data and validated it with the rest 30% data. Figure 2a showed that area under the curve (AUC) of the receiver operating characteristic (ROC) curve was 0.889 for SCr classification with validation dataset (normal, n = 41; abnormal, n = 39), indicating a satisfying classification efficacy (sensitivity = 0.846, specificity = 0.805). Furthermore, a classification model with 46 normal and 46 abnormal SCr subjects (under-sampling for the majority) produced an AUC value of 0.878 (sensitivity = 0.857, specificity = 0.857). These results suggested that the classification model performed well in separating normal SCr values from abnormalities by both oversampling or under-sampling, so exhaled VOCs could be used as a monitoring method for warning of abnormal serum creatinine status.eGFR was set as normal (> 90 ml/min/1.73 m2), mildly decreased (60–89 ml/min/1.73 m2), moderately decreased (30–59 ml/min/1.73 m2), and severely decreased (< 30 ml/min/1.73 m2) [18]. We firstly tested whether exhaled VOCs could differentiate each eGFR category using a multi-classification model. However, the multi-classification model demonstrated poor efficiency (overall accuracy = 0.51). We then tested whether VOCs could differentiate mild impairment from moderate and severe impairments. As shown in Fig. 2b, the ROC (AUC = 0.850) revealed good classification result for classify mild (normal + mild decrease, n = 78) and serious status (moderate + severe decrease, n = 97) with sensitivity 0.828 and specificity 0.782.

Mass spectrogram of breath sample using UVP-TOF-MS
BUN was defined as 50 mmol/L, with 50 normal and 125 abnormal values. The classification model by using 150% SMOTE resampling (125 normal, 125 abnormal) for the minority produced an AUC value of 0.847 (Fig. 2c, sensitivity = 0.811, specificity = 0.703). In addition, we developed a classification model by under-sampling for the majority (50 normal, 50 abnormal) produced an AUC value of 0.836 (sensitivity 0.800, specificity 0.800).
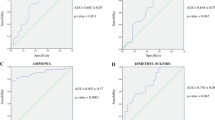
In addition to kidney function, immunosuppressants is also crucial in monitoring KTx recipients. High levels of tacrolimus could lead to severe kidney toxicity, while low levels could not achieve adequate immune suppression. It has to be closely monitored between 5 ~ 8 ng/ml. We tried a multi-classification model for three categories, which demonstrated a poor accuracy of 0.56. Therefore, to achieve higher efficacy for clinical usage, we then generated four two-classification models based on exhaled VOCs to identify low or high tacrolimus levels from normal levels. As shown in Fig. 3a-d, the validation results demonstrated that VOCs can successfully identify low or high tacrolimus levels from normal levels (low, n = 47; normal, n = 38; high, n = 63). Overall, RF classification models based on exhaled VOCs by using UVP-TOF–MS could successfully identify abnormal KTx recipients, and the classification results were summarized in Table 2.
The regression models of UVP-TOF–MS in exhaled breath correlated well with clinical parameters.
Encouraged by the excellent classification ability of exhaled VOCs, we then built regression models to determine whether exhaled VOCs could predict the actual clinical parameters. All the regression models were trained by 70% of the dataset and validated by 30% of the dataset. For kidney function parameters, the regression models exhibited acceptable correlations between clinical true values and model predicted values for creatinine (r = 0.511, p < 0.001), eGFR (r = 0.567, p < 0.001), and BUN (r = 0.269, p = 0.051). Tacrolimus levels also demonstrated good correlation efficacy (r = 0.518, p < 0.001). The correlations between true values and model predicted values were shown in Fig. 2d-f and Fig. 3e, respectively.

Classification and regression efficacy of essential kidney function parameters based on exhaled VOCs
Acetone was identified as significant exhaled content for KTx Monitoring
The above investigations have demonstrated that by using UVP-TOF–MS for the examination of VOCs from exhaled breath could either identify abnormal KTx recipients or correlate with clinical parameters. Further investigation of which VOCs contributed to the classification of KTx recipients would shed some light on the potential mechanism underlying the phenotype. A total of 52 features were found significant difference between high and low SCr gourps. The top 5 features (p < 0.01) included m/z 44, m/z 61, m/z 76, m/z 147, m/z 237 (Fig. 4a). The different exhaled breath VOCs between normal/mild decreased and moderate/severe decreased eGFR were also identified (68 features); the top 5 features (p < 0.001) were m/z 43, m/z 61, m/z 76, m/z 142, m/z 237 (Fig. 4b). In addition, 5 top VOC features, including m/z 88, m/z 198, m/z 200, m/z 261, m/z 275 (Fig. 4c), were found to be significant based on BUN levels. For tacrolimus levels, 44 VOC features showed significant differences among low, normal and high groups, and the top 5 VOCs (p < 0.01) were m/z 39, m/z 41, m/z 69, m/z 83, m/z 142 (Fig. 4d). The possible compounds corresponding to each m/z were shown in Table 3. Amone these different metabolic contents, acetone was found to be the crutial elements. Bioinformatic investigation based on the metabolic contents revealed above, we also identified that the butanoate metabolism, and propanoate metabolism were significantly affected metabolic pathways (Supplementary Fig. 5–7). This also confirmed the importance of acetone as a biomarker in monitoring kidney function.

Classification and regression efficacy of immunosuppressants (tacrolimus) concentration based on exhaled VOCs
The results of UVP-TOF–MS also showed positive correlation with other clinical parameters.
Liver function and other clinical parameters were also measured. And a regression model was generated and validated as well. Since the data were highly biased based on the discriminative analysis, the classification analysis was not performed. The regression data demonstrated that clinical true values of direct bilirubin, alanine aminotransferase, triglycerides and blood glucose were significantly correlated with model predicted values (r = 0.349, p = 0.01; r = 0.344, p = 0.011; r = 0.338, p = 0.013; r = 0.323, p = 0.018; respectively). In contrast, regression models showed ordinary performance in other clinical parameters, including total bilirubin, indirect bilirubin, total bile acids, aspartate aminotransferase, alkaline phosphatase, glutamyl transpeptidase and uric acid (Supplementary Fig. 1). Furthermore, classification model based on exhaled breath test demonstrated good discriminative efficacy for glucose status distinction (Supplementary Fig. 2). Seven exhaled VOCs showed significant difference between normal and abnormal blood glucose status (Supplementary Fig. 3).
Discussion
Exhaled breath analysis has garnered significant attention in recent years, and it might become the preferred method of choice for various applications in medical diagnostics and customized treatment monitoring in the future [19]. The UVP-TOF–MS for the VOCs analysis sheds light on a person's metabolic status through online analysis of exhaled breath is even more significant and advantageous because the results are available immediately rather than having to send samples to a lab and wait for test time [20]. Breath may be obtained in literally infinite volumes, its analysis is painless for the patient being monitored, and its online analysis enables the continuous monitoring of metabolic health, disease development, and medicine concentration in short time intervals. Furthermore, in certain critical situations, such as the emergency room, for proper treatment of a dangerous infection such as pneumonia, when consumption of potentially dangerous drugs must be determined, in doping control, or in other situations where immediate action is needed, this approach may become indispensable [21]. Exhaled breath analysis could potentially reveal novel biomarkers for diseases, allow disease phenotyping, become a low-cost alternative to established new test approaches, allow bedside or even home monitoring, and allow cost-effective and frequent checks of disease progression, therapy effectiveness, and medication adherence.
However, there are some obstacles to overcome. Exhaled breath analysis is still far from being well-established and standardized. And, currently, it is only commonly utilized in clinical practice for a few applications (lung and liver diseases, diabetes, etc.). With relatively low numbers of participants, many studies might be overfitted, therefore, biomarker candidates discovered in case‒control studies must be validated with adequate sample sizes [22]. Data treatment, particularly data processing and chemical identification, suffers from a lack of standards and reporting. There are a variety of analytical procedures that might be used, however, they all have problems with reproducibility, batch effects, temporal drift, and confounding variables. The requirements for very high sensitivity, large dynamic range to detect metabolites with widely varying concentrations, and chemical selectivity to analyze the complex mixture of compounds found in exhaled breath are at odds with the requirements for very low cost and portability of instrumentation.
The main mass spectrometry methods for detecting VOCs and subsequent analysis were selected ion flow tube mass spectrometry (SIFT-MS), proton transfer reaction mass spectrometry (PTR-MS), and secondary electrospray ionization mass spectrometry (SESI-MS) [23]. This high-resolution mass spectrometry would significantly increase the detection rate of thousands of VOCs and possibly reveal unknown compounds. However, the complex specimen and analysis processing process raised the threshold for clinical screening applications. SIFT-MS has major drawbacks due to its low MS resolution. The concept of PTR-MS itself determines the detectability limit. Proton transfer can only ionize VOCs with a greater proton affinity (PA) than H2O, allowing them to be identified using this approach. The fundamental disadvantage of SESI-MS is that it does not yet allow for absolute measurement in the gas phase. In terms of direct mass spectrometry, UVP-TOF–MS has a simpler structure than SIFT-MS, which is easier to maintain and use. And, it has simpler ionization results than PTR-MS, facilitating the understanding of the biological significance of characteristic features. Therefore, UVP-TOF–MS requires no sample preparation or VOC enrichment, and it only takes 60 s to analyze a sample compared to other MS. It also improves resolution, allowing for more accurate VOC detection and quantification. However, a potential disadvantage of UVP-TOF–MS is the aging of the UV lamp, which can cause a decrease in detection sensitivity over time. Due to its high ionization efficiency, high molecular ion yield, and low degree of fragmentation, it is one of the most potent and popular soft ionization methods for online monitoring of trace VOCs.
Therefore, in the current study, we aimed to address the limitation of traditional approaches by UVP-TOF–MS to achieve better performance and a rapid analysis process. To the best of our knowledge, this is the first study evaluating exhaled breath VOCs by using UVP-TOF–MS in monitoring KTx recipients. The results demonstrated promising outcomes and had great potential in clinical transition possibilities. Although the regression based on particular blood analysis was not as perfect as expected, the classification results were more than qualified to be a screening tool.
Although using biomarkers from the exterior environment have many advantages, there are also some major drawbacks that need to be considered. Unlike the interior environment, the exterior environment contains many different types of materials, resulting in a high degree of content diversity and variation in exhaled breath and urine. This diversity and variation can make it challenging to identify the targeted signals. Food, the environment, and other disease-irrelevant elements have some impact on exhaled breath VOCs, which increases the difficulties in classification and regression. To minimize these interferences, we collected exhaled breath before breakfast to exclude food interference. However, on the other hand, this process might hinder wider application of UVP-TOF–MS on screening KTx recipients. Therefore, there is still room for improvement. It is worth noting that certain patients experience inconvenience when giving exhaled breath samples before breakfast. Thus, future research should focus on removing confounding factors in exhaled breath samples. This will not only simplify the whole process but also provide accurate results to both clinicians and patients.
Our study identifies acetone in exhaled breath as a potential biomarker for monitoring kidney transplant (KTx) recipients. Acetone is a type of ketone that can be associated with various metabolic conditions, such as ketosis, lung cancer, dietary fat loss, and diabetes, as demonstrated by previous research. [24,25,26]. During periods of fasting, exercise, or diabetes mellitus (DM), acetone is one of the three ketone bodies synthesized via metabolic pathways in the liver by breaking down and oxidizing fatty acids to produce energy [27]. Following metabolism, acetone is circulated through the bloodstream and is expelled from the body through exhalation due to its high volatility. Research has indicated that breath acetone is a potential biomarker for diabetes and correlates with blood glucose levels [28]. Additionally, in cachexia, particularly in the end-stage of advanced diseases such as cancer, ketone bodies, including acetone, increase due to protein metabolism [29]. The kidney is a metabolically active organ that primarily derives its energy from fatty acids, lactate, glutamine, and to a lesser extent, glucose. However, during periods of energy stress or certain conditions, ketones play a critical role in maintaining cellular energy balance [30]. Upon filtration by the renal glomeruli, ketones are actively reabsorbed by tubular epithelial cells through the sodium-coupled monocarboxylate transporter 2 (SMCT2), thus minimizing urinary excretion of these valuable compounds during fasting [31]. Moreover, human positron emission tomography studies suggest that the kidney possesses a significant capacity for ketone utilization, indicating exciting prospects for future research in renal medicine. Although clinical data remain insufficient, several emerging cellular and animal experiments proposed that exogenous ketone supplementation might help safeguard the kidney against acute stress, disease conditions, and pathological alterations that occur during aging [32]. In our proposal, we suggest that impaired acetone metabolism by the kidney following transplantation may elevate the concentration of acetone in the bloodstream, resulting in an increase in exhaled breath acetone. While clinical data remain insufficient, human positron emission tomography studies suggest that the kidney possesses significant capacity for ketone utilization, indicating exciting prospects for future research in renal medicine.
Exhaled breath analysis is emerging since it can be easily obtained, the analysis is noninvasive, and the patient being analyzed is not burdened. In brief time intervals, online breath analysis also enables rapid and precise results, which is critical in instances where immediate action is needed. This approach is likely to create a new window into body metabolism and give further diagnostic insight due to the large spectrum of identified metabolites and the sensitivity and selectivity to differentiate particular molecules in exhaled breath. Exhaled breath analysis, we believe, will become the method of choice for diagnosis in a small number of specialized applications in the near future. In the long run, if validation studies with sufficient sample sizes are successful and major industries and diagnostics sectors adopt breath-based technologies, it is easy to imagine that breath-based diagnostics would replace the established tests based on urine or blood samples due to the ease and convenience of obtaining breath samples and the immediate availability of results.
Methods
Participant recruitment and study design
The Standards for Reporting of Diagnostic Accuracy (STARD) reporting standard was followed in this investigation [33]. The whole study design was presented in Fig. 5, and it employed a prospective-specimen collection, retrospective-blinded assessment (PROBE) design [34]. The Ethics Committee Board of West China Hospital, Sichuan University authorized this study, and all subjects provided written informed permission (No.2019–748). KTx recipients were recruited in the outpatient and inpatient Urology Department and Organ Transplant Center of West China Hospital, Sichuan University. In order to include all kinds of different complications post KTx, the only inclusion criterion was set as patients aged over 18 years old. Anyone who did not want to participate in the study was excluded. According to the sample size calculation by G-power, when the given significance level (α) is 0.05, power value (1-β) is 0.90, and effort size (d) is 0.5, the required sample size for each group is 73. And other studies utilizing exhaled breath as a diagnostic test which is similar to our study demonbstrated that sample size over 150 is considered acceptable [35,36,37,38]. Therefore, a total of 175 KTx recipients were recruited in our study. Samples were collected from November 1st, 2021 to March 1st 2022.

Top 5 significant different exhaled features (m/z) for KTx monitoring. (A. Creatinine; B. eGFR; C. BUN; D. Tacrolimus.)
Exhaled breath collection
Trained investigators collected all exhaled breath samples according to the collection protocol. All individuals' exhaled breath samples were taken in the morning before breakfast. To collect alveolar air, subjects were required to exhale into a Bio-VOC syringe until they felt mild resistance. The syringe expelled the dead space air from mouth and upper airway and kept the end-tidal breath gas (150 mL), which were then transferred into a 0.5L Tedlar bag. For each patient, three consecutive breaths were collected and injected into the Tedar bag. To exclude environmental contamination, we also collected room air from the same day as a negative control. All VOC tests were performed on the same day as the collection date.
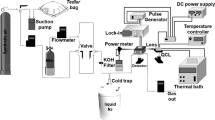
UVP-TOF–MS
Ultraviolet photoionization time-of-flight mass spectrometry (UVP-TOF–MS, ALIBEN Science & Technology Chengdu) utilized a krypton lamp as the ionization source, which produced photons with an energy of 10.6 eV. Compounds (M) into the ion source will be ionized by photons to produce cations (M +), which is formed as M + hν → M + + e. Most VOCs have an ionization potential lower than 10.6 eV and can be ionized directly. Mass spectrum peaks with mass-to-charge ratio (m/z) < 500 were detected by UVP-TOF–MS. High efficiency ion analyzer TOF can realize high-throughput and simultaneous analysis of multiple substances. The parameters of UVP-TOF–MS were set as follows: ion-source pressure 95 mbar, ion-source current 1.00 mA, and the signal accumulation time for each sample testing 50 s.
The UVP-TOF–MS is a direct mass spectrometry. Its sample introduction and detection processes are very simple, without preprocessing and parameter optimization. The mass spectrometry is in a vacuum state, with a vacuum degree of 500 Pa. When testing samples, the gaseous components will be automatically absorbed into the ion source and be ionized. Mass spectrometry can achieve a signal acquisition time of 1 s-60 s. The length of the acquisition time is related to the degree of signal accumulation. The longer the acquisition time, the higher the signal. In this work, we used a 50 s acquisition time with about 70 ml to 100 ml gas to perform exhaled breath samples detection.
Data analysis
The original UVP-TOF–MS data were preprocessed by peak integration and alignment to generate a data matrix of samples (n = 175) × features (n = 270 from m/z 29 to m/z 300). Then, standardization (Z score) made the data matrix to a common scale without distorting differences in the value ranges or losing information. Feature selection was based on mutual information scores, which measured the contribution of a feature toward reducing uncertainty about the label value. Decision forest regression and decision forest classification were used for regression and classification analysis. Parameter turning for each model was based on a random grid search algorithm. The data matrix was divided into 70% for model training and 30% for model testing. Resampling based on Synthetic Minority Oversampling Technique (SMOTE) and under-sampling by randomly sampling from the majority were used in the classification models to handle the unbalanced dataset. Statistical tests of features between different classes were made through nonparametric tests (Mann–Whitney U test for two class, Kruskal–Wallis test for multiclass), and p < 0.05 was considered statistically significant. Data processing was implemented by Python (Edition 2020.1.3) and SPSS (version 21). For bioinformatic investigations, we used KEGGREST software to map the names of metabolites of interest to corresponding KEGG compound numbers. Subsequently, pathway enrichment analysis was conducted using the clusterprofiler software against the background of all KEGG compounds. Finally, the Pathview package was employed to map the metabolites with their respective compound numbers onto the corresponding pathway maps.
Conclusion
Current breath testing may be a reliable approach for KTx recipient monitoring, and UVP-TOF–MS may provide quick, noninvasive and precise detection of exhaled breath, according to the findings of this diagnostic trial. Exhaled breath has the potential to be used in KTx recipient monitoring.
Availability of data and materials
The data supporting this study are available from the corresponding author upon reasonable request.
References
Suthanthiran M, Strom TB. Renal transplantation. N Engl J Med. 1994;331:365–76. https://doi.org/10.1056/NEJM199408113310606.
Schnuelle P, Lorenz D, Trede M, Van Der Woude FJ. Impact of renal cadaveric transplantation on survival in end-stage renal failure: evidence for reduced mortality risk compared with hemodialysis during long-term follow-up. J Am Soc Nephrol JASN. 1998;9:2135–41. https://doi.org/10.1681/ASN.V9112135.
Port FK, Wolfe RA, Mauger EA, Berling DP, Jiang K. Comparison of survival probabilities for dialysis patients vs cadaveric renal transplant recipients. JAMA. 1993;270:1339–43.
Ojo AO, Port FK, Wolfe RA, Mauger EA, Williams L, Berling DP. Comparative mortality risks of chronic dialysis and cadaveric transplantation in black end-stage renal disease patients. Am J Kidney Dis Off J Natl Kidney Found. 1994;24:59–64. https://doi.org/10.1016/s0272-6386(12)80160-0.
Josephson MA. Monitoring and managing graft health in the kidney transplant recipient. Clin J Am Soc Nephrol CJASN. 2011;6:1774–80. https://doi.org/10.2215/CJN.01230211.
Prichard SS. Comorbidities and their impact on outcome in patients with end-stage renal disease. Kidney Int. 2000;57:S100–4. https://doi.org/10.1046/j.1523-1755.2000.07417.x.
Fishman JA. Infection in Organ Transplantation. Am J Transplant Off J Am Soc Transplant Am Soc Transpl Surg. 2017;17:856–79. https://doi.org/10.1111/ajt.14208.
Danovitch GM, Bunnapradist S, Cohen D, Hariharan S, McKay D, Ratner L, et al. Tests for the noninvasive diagnosis of kidney transplant rejection should be evaluated by kidney transplant programs. Am J Transplant. 2021;21:3811–3811. https://doi.org/10.1111/ajt.16711.
Bloom RD, Bromberg JS, Poggio ED, Bunnapradist S, Langone AJ, Sood P, et al. Cell-Free DNA and Active Rejection in Kidney Allografts. J Am Soc Nephrol JASN. 2017;28:2221–32. https://doi.org/10.1681/ASN.2016091034.
Friedewald JJ, Kurian SM, Heilman RL, Whisenant TC, Poggio ED, Marsh C, et al. Development and clinical validity of a novel blood-based molecular biomarker for subclinical acute rejection following kidney transplant. Am J Transplant Off J Am Soc Transplant Am Soc Transpl Surg. 2019;19:98–109. https://doi.org/10.1111/ajt.15011.
Puttarajappa CM, Mehta RB, Roberts MS, Smith KJ, Hariharan S. Economic analysis of screening for subclinical rejection in kidney transplantation using protocol biopsies and noninvasive biomarkers. Am J Transplant Off J Am Soc Transplant Am Soc Transpl Surg. 2021;21:186–97. https://doi.org/10.1111/ajt.16150.
Grouse LD, Soffer A. Internal Milieu. Arch Intern Med. 1983;143:214. https://doi.org/10.1001/archinte.1983.00350020032006.
Gao Y. Urine is a better biomarker source than blood especially for kidney diseases. Adv Exp Med Biol. 2015;845:3–12. https://doi.org/10.1007/978-94-017-9523-4_1.
Buszewski B, Kesy M, Ligor T, Amann A. Human exhaled air analytics: biomarkers of diseases. Biomed Chromatogr BMC. 2007;21:553–66. https://doi.org/10.1002/bmc.835.
Novak BJ, Blake DR, Meinardi S, Rowland FS, Pontello A, Cooper DM, et al. Exhaled methyl nitrate as a noninvasive marker of hyperglycemia in type 1 diabetes. Proc Natl Acad Sci U S A. 2007;104:15613–8. https://doi.org/10.1073/pnas.0706533104.
Phillips M, Cataneo RN, Ditkoff BA, Fisher P, Greenberg J, Gunawardena R, et al. Volatile markers of breast cancer in the breath. Breast J. 2003;9:184–91. https://doi.org/10.1046/j.1524-4741.2003.09309.x.
Sánchez C, Santos JP, Lozano J. Use of Electronic Noses for Diagnosis of Digestive and Respiratory Diseases through the Breath. Biosensors. 2019;9:35. https://doi.org/10.3390/bios9010035.
Chapter 1: Definition and classification of CKD. Kidney Int Suppl 2013;3:19–62. https://doi.org/10.1038/kisup.2012.64.
Davis MD, Fowler SJ, Montpetit AJ. Exhaled breath testing - A tool for the clinician and researcher. Paediatr Respir Rev. 2019;29:37–41. https://doi.org/10.1016/j.prrv.2018.05.002.
Bhadra S, Zhang Z, Zhou W, Ochieng F, Rockwood GA, Lippner D, et al. Analysis of potential cyanide antidote, dimethyl trisulfide, in whole blood by dynamic headspace gas chromatography-mass spectroscopy. J Chromatogr A. 2019;1591:71–8. https://doi.org/10.1016/j.chroma.2019.01.058.
Bruderer T, Gaisl T, Gaugg MT, Nowak N, Streckenbach B, Müller S, et al. On-Line Analysis of Exhaled Breath Focus Review. Chem Rev. 2019;119:10803–28. https://doi.org/10.1021/acs.chemrev.9b00005.
Meng S, Li Q, Zhou Z, Li H, Liu X, Pan S, et al. Assessment of an Exhaled Breath Test Using High-Pressure Photon Ionization Time-of-Flight Mass Spectrometry to Detect Lung Cancer. JAMA Netw Open 2021;4:e213486. https://doi.org/10.1001/jamanetworkopen.2021.3486.
Gaugg MT, Bruderer T, Nowak N, Eiffert L, Martinez-Lozano Sinues P, Kohler M, et al. Mass-Spectrometric Detection of Omega-Oxidation Products of Aliphatic Fatty Acids in Exhaled Breath. Anal Chem. 2017;89:10329–34. https://doi.org/10.1021/acs.analchem.7b02092.
Hakim M, Broza YY, Barash O, Peled N, Phillips M, Amann A, et al. Volatile organic compounds of lung cancer and possible biochemical pathways. Chem Rev. 2012;112:5949–66. https://doi.org/10.1021/cr300174a.
Wang Z, Wang C. Is breath acetone a biomarker of diabetes? A historical review on breath acetone measurements. J Breath Res 2013;7:037109. https://doi.org/10.1088/1752-7155/7/3/037109.
Worrall AD, Qian Z, Bernstein JA. Water-Resistant Polymeric Acid Membrane Catalyst for Acetone Detection in the Exhaled Breath of Diabetics. Anal Chem. 2018;90:1819–26. https://doi.org/10.1021/acs.analchem.7b03808.
Laffel L. Ketone bodies: a review of physiology, pathophysiology and application of monitoring to diabetes. Diabetes Metab Res Rev. 1999;15:412–26. https://doi.org/10.1002/(SICI)1520-7560(199911/12)15:6%3c412::AID-DMRR72%3e3.0.CO;2-8.
Ruzsányi V, Péter Kalapos M. Breath acetone as a potential marker in clinical practice. J Breath Res 2017;11:024002. https://doi.org/10.1088/1752-7163/aa66d3.
Haick H, Broza YY, Mochalski P, Ruzsanyi V, Amann A. Assessment, origin, and implementation of breath volatile cancer markers. Chem Soc Rev. 2014;43:1423–49. https://doi.org/10.1039/c3cs60329f.
Baverel G, Ferrier B, Martin M. Fuel selection by the kidney: adaptation to starvation. Proc Nutr Soc. 1995;54:197–212. https://doi.org/10.1079/PNS19950049.
Sapir DG, Owen OE. Renal conservation of ketone bodies during starvation. Metabolism. 1975;24:23–33. https://doi.org/10.1016/0026-0495(75)90004-9.
Cuenoud B, Hartweg M, Godin JP, Croteau E, Maltais M, Castellano CA, Carpentier AC, Cunnane SC. Metabolism of Exogenous D-Beta-Hydroxybutyrate, an Energy Substrate Avidly Consumed by the Heart and Kidney. Front Nutr. 2020;7:13. https://doi.org/10.3389/fnut.2020.00013.
Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig L, et al. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015;351:h5527. https://doi.org/10.1136/bmj.h5527.
Ransohoff DF. The process to discover and develop biomarkers for cancer: a work in progress. J Natl Cancer Inst. 2008;100:1419–20. https://doi.org/10.1093/jnci/djn339.
Plantier L, Smolinska A, Fijten R, Flamant M, Dallinga J, Mercadier JJ, et al. The use of exhaled air analysis in discriminating interstitial lung diseases: a pilot study. Respir Res. 2022;23:12. https://doi.org/10.1186/s12931-021-01923-5.
Dreßler M, Salzmann-Manrique E, Zielen S, Schulze J. Exhaled NO as a predictor of exercise-induced asthma in cold air. Nitric Oxide Biol Chem. 2018;76:45–52. https://doi.org/10.1016/j.niox.2018.03.004.
Di W, Ran Q, Yang H, Lu J, Hou Y, Wang X, et al. Use of graft-derived cell-free DNA as a novel biomarker to predict allograft function after kidney transplantation. Int J Urol Off J Jpn Urol Assoc. 2021;28:1019–25. https://doi.org/10.1111/iju.14638.
Smith AD, Cowan JO, Taylor DR. Exhaled nitric oxide levels in asthma: Personal best versus reference values. J Allergy Clin Immunol. 2009;124:714-718.e4. https://doi.org/10.1016/j.jaci.2009.07.020.
Acknowledgements
This research was gratefully supported by the Sichuan Science and Technology Program, China (2022YFG0082), and Post Doctor Research Project, West China Hospital, Sichuan University (2020HXBH149).
Funding
Sichuan Science and Technology Program,China,2022YFG0082,Zhongjun Zhao,Post Doctor Research Project,West China Hospital,Sichuan University,2020HXBH149,Shijian Feng.
Author information
Authors and Affiliations
Contributions
Shijian Feng: Collected the sample, performed the experiments, analyzed the data, drafted the manuscript. Xiangcheng Fang: Designed the study, collected the sample, performed the experiments, analyzed the data. Yushi He: Collected the sample, performed the experiments, analyzed the data. Zhuoya Li: Collected the sample, performed the experiments, analyzed the data Zhongjun Zhao: Performed the experiments, analyzed the data. Bohan Liu: Performed the experiments, analyzed the data. Zhaofa Yin: Performed the experiments, analyzed the data. Qiyu He: Performed the experiments, analyzed the data. Yanting Yang: Analyzed the data. Zhongli Huang: Interpreting the data, revised the manuscript. Tao Lin: Interpreting the data, revised the manuscript. Wenwen Li: Supervised the study, analyzed the data, drafted the manuscript. Yixiang Duan: Supervised the study, analyzed the data, drafted the manuscript. All authors have read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This research is approved by the Ethics Committee Board of West China Hospital, Sichuan University (No.2019-748), and all subjects provided written informed permission.
Competing interests
The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure 1.
Correlations between clinical true values and regression model predicted values of blood glucose, triglycerides, uric acid, total bilirubin, direct bilirubin, indirect bilirubin, total bile, aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, glutamyl transpeptidase of KTx patients. Figure 2. RF model for glucose status (135 normal and 40 high) classification by 200% SMOTE resampling (left, 135 normal vs 120 high) and under-sampling (right, 40 normal vs 40 high). Figure 3. Significant exhaled compounds (p<0.01) between normal (<5.9mmol/L) and high blood glucose status (>5.9 mmol/L). Figure 4. Raw mass spectra of standards of significant exhaled compounds. Figure 5. KEGG pathway analysis based on different exhaled metabolic contents. Figure 6. Crucial different metabolic contents identified by UVP-TOF-MS involved inbutanoate metabolism. Figure 7. Crucial different metaboliccontents identified by UVP-TOF-MS involved in propanoate metabolism.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Feng, S., Xiang, C., He, Y. et al. Assessment of an exhaled breath test using ultraviolet photoionization time-of-flight mass spectrometry for the monitoring of kidney transplant recipients. Mol Biomed 4, 19 (2023). https://doi.org/10.1186/s43556-023-00130-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43556-023-00130-6