
Abstract
Background
Pulmonary vein thrombosis is a rare condition with a non-specific presentation with multiple underlying etiologies such as malignancy or lung surgery. In rare instances, no etiology could be encountered. Instead, it has a broad spectrum of clinical manifestations, from dyspnea to lung infarction with a compromise to hemodynamics.
Case presentation
A 71 years old male with a history of shortness of breath. The patient tested positive for COVID-19; the prolonged exertional fatigue led to undergoing CTPA (CT pulmonary angiography), which revealed pulmonary vein thrombosis. This case emphasizes the importance of maintaining a high index of clinical suspicion in the absence of other possible diagnoses. Furthermore, diagnostic work-up and treatment strategies depend highly on the patient’s presentation and risk factors.
Conclusions
Pulmonary vein thrombosis is an infrequent entity reported in the medical literature and underdiagnosed because of its ambiguous presentation. Early diagnosis is paramount to prevent complications.
Similar content being viewed by others


Background
Pulmonary vein thrombosis (PVT), in which a thrombus or a blood clot is formed and lodged into pulmonary veins, is an uncommon condition; however, it is a life-threatening disease.
It is commonly associated with lung malignancy, including primary or metastatic lung surgeries such as lobectomy, polycythemia vera, or blunt chest trauma as reported in most literature cases, and some cases have been reported the condition idiopathic [1]. PVT presentation is usually nonspecific, making it challenging to diagnose; however, patients primarily present with dyspnea, pleuritic chest pain, and occasionally hemoptysis.
Because it is difficult to diagnose, diagnosing PVT needs a high clinical suspicion and a combination of different diagnostic modalities, including laboratory and radiological tools. Pulmonary CT angiography is usually the initial diagnostic method; other modalities include transesophageal ECHO and MRI.
Management of PVT is usually by using anticoagulation in case of the absence of contraindications to them. However, it can include antibiotics, thrombectomy, or even pulmonary resection. We reported a case of a 71-year-old male diagnosed with pulmonary vein thrombosis with the aid of pulmonary CT angiography and was started on anticoagulation for 6 months.
Case presentation
A 71-year-old male patient presented to the emergency department complaining of shortness of breath of 2 days in duration that was not relieved with symptomatic treatment. He denied a history of cough, fever, chills, palpitations, or chest pain; there was no history of urinary or abdominal symptoms. There was no history of sick contacts at home. He was fully vaccinated against COVID, including a booster dose. He received two doses of the inactivated SARS-CoV2 Sinopharm vaccine in March and April 2021, followed by a booster dose of the Pfizer-BioNTech COVID-19 vaccine in August 2021.
His past medical history includes chronic obstructive pulmonary disease and benign prostatic hyperplasia.
His vital signs on arrival were a temperature of 36.7 °C, a blood pressure of 112/78 mmHg, a heart rate of 99 bpm, a respiratory rate of 25 breaths per minute, and an oxygen saturation of 95% on 2 L of oxygen via nasal cannula. Examination of the chest revealed equal bilateral air entry with scattered wheezes over all lung fields.
Complete laboratory investigations were done, including COVID-19 PCR that came out positive, so the patient was shifted to a COVID-19 facility; all other laboratory investigation was within the normal range, including complete blood count, renal function test, liver function test, coagulation profile, and inflammatory markers.
During his stay in COVID-19 treatment facility, the patient was kept on nebulizers, oxygen via nasal cannula, dexamethasone 8 mg intravenously, and antiviral medications (remdesivir) for 5 days as per Bahrain’s National COVID-19 treatment protocol [2].
Oxygen requirements were being gradually tapered off as tolerated with a target saturation of 88–92% until patient maintained saturation on room air and no longer complained of shortness of breath. Hence, patient was discharged home in stable condition.
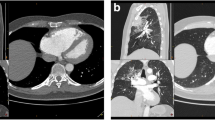
Two weeks later, the patient presented again to the emergency department with similar complaint. His vital signs on arrival were a temperature of 36.6 °C, a blood pressure of 110/72 mmHg, a heart rate of 127 bpm, a respiratory rate of 35 breaths per minute, and an oxygen saturation of 98% on 4 L of oxygen via nasal cannula. His arterial blood gas showed a pH of 7.41, pO2 of 79.9 mmHg, pCO2 42.1 mmHg, HCO3− of 25.4 mmol/L, and SpO2 of 95.5%. COVID-19 Rapid Ag was done as the patient’s main presentation to the emergency department was respiratory symptoms and reported positive for COVID-19. Hence, patient was re-admitted in COVID-19 treatment facility and was started on nebulizers and continued on oxygen via nasal cannula. During his second admission, the patient was noted to be tachycardic and tachypneic with a D-dimer level of 0.72 µg/mL and complained of worsening shortness of breath, especially on exertion. Hence, a decision to proceed with CT pulmonary angiography was made to rule out pulmonary embolism. Surprisingly, a left inferior pulmonary vein thrombosis was noted (Figs. 1 and 2). Thus, the hematology team was consulted regarding this radiological finding and advised for anticoagulation (dabigatran 150 mg twice daily orally) for 6 months.

The patient has severe emphysematous changes and consolidation in the left upper lobe

CTPA showing a filling defect in the left inferior pulmonary vein
During his subsequent visits to the pulmonology and hematology clinic, the patient was compliant with his medications (nebulizers and anticoagulation). The patient was symptomatically better and did not suffer from any respiratory symptoms or exacerbation that necessitated hospitalization.
Discussion
Pulmonary vein thrombosis is a rare thrombotic condition. However, it is a severe life-threatening disease. Moreover, diagnosing it is challenging given the nonspecific presenting symptoms [3,4,5,6]. The most reported causes of pulmonary vein thrombosis are primary lung malignancy, major lung surgeries such as lung transplants involving pulmonary veins, lung lobectomy, and even cases with radiofrequency ablation of atrial fibrillation [7].
Patients with pulmonary vein thrombosis are usually asymptomatic, making the disease challenging to diagnose. However, some individuals present with nonspecific symptoms, such as dyspnea, chest pain, or hemoptysis, and as a result, it can be misdiagnosed as pulmonary embolism. Our patient was mainly complaining of dyspnea along with the COVID-19 infection.
There are multiple explanations for the development of pulmonary vein thrombosis in our patient. In a study conducted by Rizkallah et al. [8], it was reported that patients with acute exacerbation of chronic obstructive pulmonary disease who require hospitalization may have pulmonary embolism and a diagnosis of pulmonary embolism should be considered in patients with severe exacerbation, particularly those with a high pretest probability of pulmonary embolism. Another reason for the development of thrombosis in our patient is COVID-19 infection itself as one of the major clinical manifestations of COVID-19 infection is coagulopathy due to endothelial injury, cytokine storm, complement activation, and induction of inflammatory response [9]. Lastly, in a study conducted by Bernardi et al., it has been reported that thromboembolic events were higher in patients receiving a viral-vector-based vaccine (Oxford-AstraZeneca) compared to the mRNA-based vaccine (Pfizer-BioNTech) [10]. Thus, several factors can explain the likelihood of developing thrombosis in our patient.
In pulmonary vein thrombosis, there will be an increase in pulmonary vasculature pressure secondary to the thrombus [4]. As a result, pulmonary arterial vasculature will go into vasoconstriction, leading to a rise in pulmonary arterial pressure and an increase in right ventricular pressure [4]. Consequently, the patient might end up with cor pulmonale if left untreated.
As discussed above, diagnosing pulmonary vein thrombosis is difficult, given the non-specific symptoms and the need for high clinical suspicion. However, a combination of diagnostic modalities, such as pulmonary CT angiography, the diagnostic method used in our patient, transesophageal ECHO, and MRI, has been used in the diagnosis. Nonetheless, pulmonary vein thrombosis is poorly discussed in the literature reviews and very few cases were described in literature.
The management of pulmonary vein thrombosis is merely based on the cause and the severity of the patient’s presentation and can include either antibiotics, anticoagulation, thrombectomy, or pulmonary resection [11]. Unfortunately, there is no agreement on the optimal management due to a scarcity of data. However, anticoagulation is recommended to reduce the risk of embolization and propagation as illustrated in this case report. In addition, there is no agreement on the preferred duration of anticoagulation or the type of anticoagulation [11]. Clinicians should also consider lifelong anticoagulation for idiopathic pulmonary vein thrombosis as proposed in Chest journal [11]. The role of antibiotics in pulmonary vein thrombosis is reserved in patients with lobectomy due to possibility of superimposed infection [6].
The decision to proceed with anticoagulation in the form of dabigatran is governed by the limited case reports available regarding the treatment of pulmonary vein thrombosis. The prognosis of this disease entity depends on the clot burden [12].
Various different studies described the association of COVID-19 infection with pulmonary embolism mainly affecting the arterial system [13, 14]. However, few cases in literature reported clot formation in the pulmonary veins. Hence, clinicians should be vigilant of other diagnosis such as pulmonary vein thrombosis as a diagnosis since early detection can affect the patient management plan.
In our case, the patient’s initial chest symptoms, including shortness of breath along with COVID infection and a history of smoking, were suggestive of acute COPD exacerbation, however with the acute onset of worsening shortness of breath, tachycardia, and tachypnea; it was essential to rule out other differential diagnoses such as pulmonary embolism, for that reason a CTPA was ordered and was unexpectedly reported, the presence of left inferior pulmonary vein thrombus.
Conclusions
Pulmonary vein thrombosis is a rare entity with an unknown incidence, as most literature includes case reports. However, the unique presentation of our patient with prolonged exertional fatigue led to further investigation to unveil the reason for his presentation. Early diagnosis is paramount for the early initiation of treatment and for preventing complications from occurring. Treatment should be tailored based on individual cases by systemic anticoagulation, thrombectomy, or pulmonary resection.
Availability of data and materials
Not applicable.
Abbreviations
- CTPA:
-
CT pulmonary angiography
- COVID-19:
-
Coronavirus disease 2019
- PVT:
-
Pulmonary vein thrombosis
- ECHO:
-
Echocardiography
- MRI:
-
Magnetic resonance imaging
- PCR:
-
Polymerase chain reaction
References
Selvidge SD, Gavant ML (1999) Idiopathic pulmonary vein thrombosis: detection by CT and MR imaging. AJR Am J Roentgenol 172(6):1639–1641
Bahrain COVID-19 protocols. NHRA. Available from: https://www.nhra.bh/. Accessed 15 July 2024
van Kruijsdijk RC, de Jong PA, Abrahams AC (2020) Pulmonary vein thrombosis in COVID-19. BMJ Case Rep 13(10):e239986
Chaaya G, Vishnubhotla P (2017) Pulmonary vein thrombosis: a recent systematic review. Cureus 9(1):e993
Stein PD, Denier JE, Goodman LR, Matta F, Hughes MJ (2018) Pulmonary vein thrombosis in patients with medical risk factors. Radiol Case Rep 13(6):1170–1173
Rana MA, Tilbury N, Kumar Y, Ahmad H, Naser K, Mady AF, Patel A (2016) Idiopathic pulmonary vein thrombus extending into left atrium: a case report and review of the literature. Case Rep Med 2016:3528393
Barreiro TJ, Kollipara VK, Gemmel DJ (2017) Idiopathic pulmonary vein thrombosis? Respirol Case Rep 6(1):e00277
Rizkallah J, Man SFP, Sin DD (2009) Prevalence of pulmonary embolism in acute exacerbations of COPD: a systematic review and metaanalysis. Chest 135(3):786–793
Sutanto H, Soegiarto G (2023) Risk of thrombosis during and after a SARS-CoV-2 infection: pathogenesis, diagnostic approach, and management. Hematol Rep 15(2):225–243
Bernardi FF, Mascolo A, Sarno M, Capoluongo N, Trama U, Ruggiero R, Sportiello L, Fusco GM, Bisogno M, Coscioni E, Iervolino A, Di Micco P, Capuano A, Perrella A (2023) Thromboembolic events after COVID-19 vaccination: an Italian retrospective real-world safety study. Vaccines (Basel) 11(10):1575
Goddard SA, Tran DQ, Chan MF, Honda MN, Weidenhaft MC, Triche BL (2021) Pulmonary vein thrombosis in COVID-19. Chest 159(6):e361–e364
Gharepapagh E, Rahimi F, Koohi A, Bakhshandeh H, Mousavi-Aghdas SA, Sadeghipoor P, Fakhari A, Amirnia M, Javadrashid R, Rashidi F (2023) Clot burden as a predictor of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: a cohort study. Thorac Res Pract 24(5):276–281
Badr OI, Alwafi H, Elrefaey WA, Naser AY, Shabrawishi M, Alsairafi Z, Alsaleh FM (2021) Incidence and outcomes of pulmonary embolism among hospitalized COVID-19 patients. Int J Environ Res Public Health 18(14):7645
El Rhalete A, Rhazi I, Bensaid A, Zaid I, Bkiyer H, Ismaili N, Elouafi N, Housni B (2021) Cardiovascular injuries during COVID-19 infection: a PROCESS-compliant case series from the Eastern Morocco. Ann Med Surg (Lond) 65:102309
Acknowledgements
None.
Funding
No funding was received for the study.
Author information
Authors and Affiliations
Contributions
NH and KA organized the manuscript. AH was the supervising consultant who supported NH and KA. GH and HE offered radiology input. NH, KA, and AH offered content input, edited the manuscript, and reviewed it in its final form. All authors were involved in the patient’s care.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethics approval was attained by the Research and Ethics Committee of the Institution (Bahrain Defence Force Hospital- Royal Medical Services).
Consent for publication
A written informed consent was obtained for the publication of this case report from the patient.
Competing interests
The authors declare no competing interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alaazmi, N.H., Yusuf, K.A., Al-Madani, A.H. et al. Pulmonary vein thrombosis in COVID-19 patient with chronic obstructive pulmonary disease: a case report. Egypt J Bronchol 18, 55 (2024). https://doi.org/10.1186/s43168-024-00308-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-024-00308-8