
Abstract
Background
Sleep disordered breathing (SDB) is a widespread disorder with a wide range of harmful outcomes including obstructive sleep apnea (OSA), central sleep apnea (CSA), or sleep-related hypoventilation.
Purpose
The aim of the present study was to screen for the occurrence of sleep apnea syndrome in patients with type 2 diabetes mellitus (DM) and to evaluate the relation between the presence of sleep apnea and the level of glycemic control.
Methods
This was a prospective clinical study that enrolled 59 patients who were previously diagnosed as type 2 DM. Sleep study level IV was done using overnight recording of oxygen saturation and pulse.
Results
Among the studied patients, 42 were females and 17 were males, Their mean age was 59.76 ± 11.13 years. Obstructive sleep apnea was diagnosed in 46 patients (78%). Thirty three (86.8%) patients among those with uncontrolled glycemic level were diagnosed as OSA, whereas 13(61.9%) patients with controlled glycemic level were diagnosed as OSA showing statistically significant difference, p = 0.047. There was no correlation between either HbA1c, age, Mallampati score, or BMI and ODI but there was a correlation between STOP-BANG questionnaire and ODI (P = 0.036). The variables that were significantly related to presence of OSA, were comorbidities, ESS, Mallampati score, STOP-BANG, and sleep symptoms (nocturia and snoring) P value (0.029), (0.031), (0.022), (0.005), (0.049), and (0.012), respectively.
Conclusion
Patients with type 2 diabetes showed a significant high prevalence of OSA. With significant higher prevalence among patients with uncontrolled DM versus controlled DM.
Similar content being viewed by others

Introduction
Sleep disordered breathing (SDB) is a widespread disorder with a wide range of harmful outcomes including obstructive sleep apnea (OSA), central sleep apnea (CSA) or sleep-related hypoventilation [1, 2]. The International Classification of Sleep Disorders, defined OSA as a chronic treatable disorder that has a clinical impact on lifespan. It is defined by repeated events of total (apnea) or partial (hypoapnea) blockage of the upper airway during sleep whereas respiratory efforts last, frequently causing arousals leading to intermittent hypoxemia, interrupted sleep, repeated arousals and sleep fragmentation [2]. The prevalence of OSA varies greatly between studies due to differences in the criteria used to define it as well as differences in the populations studied [3]. The estimated prevalence of OSA in the general adult public ranges from 9 to 38% [4,5,6]. Because chronic intermittent hypoxia (CIH) is a common component of OSA, it is a major cause of morbidity [7, 8].
Obesity, age, sex, race/ethnicity, and heritable factors are all well-documented risk factors in the pathology of sleep apnea [9]. Obese patients with OSA are more likely to develop type 2 diabetes [10,11,12]. Furthermore, Untreated OSA has been related to an increased risk of a number of illnesses and diseases over time, including hypertension, stroke, type 2 diabetes, obesity, dyslipidemia, metabolic syndrome, non-alcoholic fatty liver disease, cancer, and depression [13].
OSA is linked to glucose metabolism abnormalities such as insulin resistance and diabetes mellitus. Intermittent hypoxia, sleep fragmentation, aggravation of systemic inflammation, and elevation of sympathetic muscle activity are some of the pathophysiological mechanisms that relate OSA to DM [14].
Intermittent hypoxia, which can cause β cell malfunction and insulin resistance, is one proposed mechanism linking OSA to T2DM. An increase in adrenaline, norepinephrine, and cortisol secretion, in combination with oxyhemoglobin desaturation and hypercarbia, leads to increased gluconeogenesis. In many studies, continuous positive airway pressure (CPAP) was found to improve glycemic control, postprandial glucose levels, and HbA1c [15, 16].
OSA is also more common in overweight and obese people, and because excess body weight is also a key risk factor for T2DM, it is unclear whether the T2DM-OSA link is due to OSA-mediated changes in glucose metabolism or merely reflects a link with excess adiposity [17]. According to the previous findings, OSA is an independent risk factor for the development of type 2 diabetes, with 15–30% of OSA patients developing type 2 diabetes [18].
On the other hand, several studies have found a considerable increase in the prevalence of OSA among individuals with diabetes mellitus, with prevalence rates ranging between 73 and 86% [19]. The American Diabetes Association, the International Diabetes Taskforce on Epidemiology and Prevention, and the American Academy of Sleep Medicine (AASM) have announced clinical guidelines urging that patients with type 2 diabetes be screened for OSA on a regular basis [20, 21].
The aim of the present study was to screen for the occurrence of sleep apnea syndrome in patients with type 2 diabetes mellitus and to evaluate the relation between the presence of sleep apnea and the level of glycemic control.
Patients and methods
This was a prospective clinical study. The current study was conducted at the department of Diabetes and Metabolism, Alexandria Main University Hospital in the duration between May 2019 and May 2020.We enrolled 59 patients who were previously diagnosed as having type 2 DM. We enrolled Patients over 18 years of age diagnosed with type 2 DM. Exclusion criteria included patients known to have other sleep disorders, patients refusing to participate, type 1 diabetic patients, and critically ill patients. All patients enrolled in the study signed an informed consent before participation. The study was accepted by the local ethical committee of Alexandria Faculty of Medicine (available from www.med.alexu.edu.eg/wp-content/uploads/2012/04/ethics-guide.pdf). For every eligible patient the following data were collected: full history, smoking history, and history about any comorbid illness or drugs taken by the patients. Symptoms relevant to sleep disorders were reported as snoring, choking or gasping attacks at night, witnessed apneas, EDS, unrefreshing sleep, recurrent arousals, nocturia, morning headaches, memory and personality changes, morning dry mouth, morning laziness and fatigue. Anthropometric measurement were reported including BMI:(Quetelet’s index) [22], neck circumference was measured at mid-neck, between the midcervical spine and the mid anterior neck, on subjects standing upright and facing forwards, with shoulders relaxed. In men with a laryngeal prominence (Adam’s apple), it was measured just below the prominence [23] waist-hip ratio was measured according to WHO protocol [24]: waist circumference was measured at the end of several consecutive natural breaths, at a level parallel to the floor, midpoint between the top of the iliac crest and the lower margin of the last palpable rib in the mid axillary line. Hip circumference was measured at a level parallel to the floor, at the largest circumference of the buttocks. The subject was standing upright, with arms relaxed at the side, feet evenly spread apart [24]. Mallampati score [25] was assessed. The patient was instructed to open his or her mouth as wide as possible, while protruding the tongue as far as possible. Patients were instructed to not emit sounds during the assessment. A score (I–IV) was obtained by visual inspection of the soft palate, hard palate, and tongue. Assessment of excessive daytime sleepiness was done using Epworth sleepiness scale (ESS) [26]. STOP-BANG questionnaire was used to asses risk of having OSA [27]. Sleep study level IV was done using overnight recording of oxygen saturation and pulse by the use of Heal Force Prince-100F Handheld Pulse Oximeter, Shanghai, China.
Based on the cutoff for “significant” oxygen desaturations 3% during sleep, we considered patients diagnosed as OSA if ODI > 5 plus symptoms or > 15 without symptoms [28]. Laboratory assessment included fasting plasma glucose level, fasting insulin level and glycated hemoglobin (HbA1c). The American diabetes association (ADA) has determined glycosylated hemoglobin (A1C) as the best measure of glycemic control, level less than 7% as a goal of optimal blood glucose control to prevent the complications and to reduce overall disease management costs [29].
Assessment of insulin resistance by using Homeostasis Model Assessment 2 (HOMA2) calculator [30]. Complete lipid profile was done [31] (total serum cholesterol, high-density lipoprotein cholesterol (HDL-cholesterol), low-density lipoprotein cholesterol (LDL-cholesterol), serum triglycerides) [32].
Statistical analysis of the data
Data were fed to the computer and analyzed using IBM SPSS software package version 20.0. (Armonk, NY: IBM Corp.) [33]. Qualitative data were described using number and percent. The Kolmogorov-Smirnov test was used to verify the normality of distribution. Quantitative data were described using range (minimum and maximum), mean, standard deviation, median, and interquartile range (IQR). Significance of the obtained results was judged at the 5% level. The used tests were chi-square test: for categorical variables, to compare between different groups. Mann-Whitney test: for abnormally distributed quantitative variables to compare between two studied groups. Spearman coefficient: to correlate between two distributed abnormally quantitative variables. Student’s t test: for normally distributed quantitative variables, to compare between two studied groups. Fisher’s exact or Monte Carlo correction: correction for chi-square when more than 20% of the cells have expected count less than 5.
Results
Fifty-nine patients diagnosed as type 2 DM were enrolled in the current study in the period between May 2019 and May 2020. Among the studied patients, 42 (71.2%) were females and 17 (28.8%) were males, Their mean age was 59.76 ± 11.13 years (range 54–65.5 years). The mean BMI and neck circumference in the participants investigated was 34.56 ± 8.17 kg/m2 (range 20.7–54.6 kg/m2), and 40.49 ± 2.34 cm (range 36–45 cm) respectively. For waist/hip ratio, the mean value was 0.89 ± 0.09 ranging between 0.7 and 1.03. The distribution of the most common associated comorbidities other than DM was as follows: hypertension (HTN), ischemic heart diseases (IHD), asthma, atrial fibrillation (AF), hypothyroidism, chronic kidney diseases (CKD), and stroke in 46(78%), 16(27.1%), 8(13.6%), 4(6.8%), 2 (3.4%), 2 (3.4%), and 1 (1.7%) of the patients, respectively.
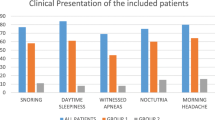
The most frequent presenting symptom was snoring which was reported in 44(74.6%) patients. This was followed by daytime sleepiness, nocturia, witnessed apnea and choking in 27 (45.8%), 24 (40.7%), 19(32.2%), and 7 (11.9%) patients, respectively. Their Epworth sleepiness scale ranged from 4 to 15 with a mean of 8.97 ± 2.74.
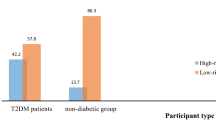
Patients were divided into two groups based on their OSA risk using STOP-BANG questionnaire: high risk (48(81.4%) patients) and low risk (11(18.6%) patients. STOP-BANG questionnaire score ranged from 1 to 7 with a mean of 4.48 ± 1.73. Mallampati score 4 was present in 32 (54.2%) patients, while Mallampati score 3 was in 4 (6.8%) patients, score 2 was in 14(23.7%) patients and score 1 was in 9 (15.3%) patients. The mean score was 3.0 ± 1.19 overnight pulse oximetry was used to screen for OSA and calculate ODI. Patients were diagnosed as OSA if ODI > 5 plus symptoms or > 15 without symptoms (Table 1).
Laboratory assessment of the studied patients was presented in Table 2. According to the results of the blood test, patients were classified as controlled or uncontrolled diabetes.
In our study, 33(86.8%) patients among those with uncontrolled glycemic level were diagnosed as OSA, whereas 13(61.9%) patients with controlled glycemic level were diagnosed as OSA showing statistically significant difference, p = 0.047 (Fig. 1). Thirty-three (71.7%) patients out of 46 patients were diagnosed as OSA had uncontrolled DM. Table 3 shows comparison between patients diagnosed as OSA and those not diagnosed as OSA regarding different variables.

The presence of OSA among patient with or without controlled DM (n = 59)
In our study, there was no correlation between HbA1c, age, Mallampati score, and BMI and ODI but there was a correlation between STOP-BANG questionnaire and ODI (P = 0.036), (Table 4).
By analyzing the effect of different variables on presence of OSA (Table 5). It was found that variables were significantly related to presence of OSA, which were comorbidities, ESS, Mallampati score, STOP-BANG, and symptoms of sleep (nocturia and snoring) P value was (0.029), (0.031), (0.022), (0.005), (0.049), and (0.012) respectively. Nevertheless, there was no variable taking the upper hand and affecting the other variables.
Discussion
Obstructive sleep apnea is one of the most major causes of sleep disruption (OSA) [34]. The purpose of this study was to assess presence of sleep apnea syndrome among patients with type 2 diabetes and if there was a link between sleep apnea and blood glucose levels.
We enrolled 59 persons with type 2 diabetes, with a mean age of 59.76 ± 11.13 years (more than 80% of the studied patient over 50 years). In the current study, 42 patients (71.2%) were females and 17 patients (28.8%) were males. This came in agreement with Megahed and Farag [35] who revealed that more than two thirds of their studied sample of diabetic patients were females. Similarly, two studies conducted in India by Dussa et al. [36] and Mufunda et al. [37] found that females represented more than two thirds of their studied diabetic patients. This could be explained by a study done in Denmark by Juel et al. [38], which showed that men react later to severe symptoms than women.
Regarding the incidence of other comorbidities, the most common was hypertension (HTN) in 78% of the patients, followed by Ischemic heart diseases (IHD), asthma, atrial fibrillation (AF), hypothyroidism, chronic kidney diseases (CKD), and stroke that were present in 16 (27.1%), 8 (13.6%), 4(6.8%), 2 (3.4%), 2 (3.4%), and 1 (1.7%) patient, respectively. In accordance with Souliotis et al. [39] who found a significant prevalence of hypertension in 58.9% of diabetics evaluated. These findings are in line with earlier studies, which found a higher prevalence of these disorders in diabetics. In a cohort study conducted by Arnold et al. [40] hypertension was estimated to be present in 76.3% of the participants.
In this study of hospitalized diabetic patients, patients were considered uncontrolled using the result of HbA1c.The number of uncontrolled patients versus the number of controlled were 38 (64.4%) versus 21 (35.6%) patients, respectively. This result was also in line with findings from a large-scale outpatients multicenter survey of nearly 240,000 patients across China, which stated that patients with T2DM do not meet the American Diabetes Association (ADA) and the Chinese Medical Society's treatment guideline of a HbA1c of less than 7%. Glycemic control, as defined by HbA1c < 7.0%, was attained by less than a third of those with type 2 DM [41]. In a research done in India by Borgharkar et al. [42]. Nearly 76.6% of patients had uncontrolled glycated hemoglobin (HbA1c) ≥ 7%, according to a systematic analysis of cross-sectional data collected from urban healthcare facilities across 26 states. This could be explained by the fact that in a developing country already overwhelmed with a growing population, inadequate resources, and rising life expectancy, sub-optimal DM therapy is expected. Patient education is seen as a critical element in the management of diabetes. Effective diabetes education leads to better disease control [43].
In the current study, the most frequent presenting symptom related to sleep disorders was snoring which was reported by 44(74.6%) of the total studied patients. This was followed by daytime sleepiness, nocturia, witnessed apnea and choking in 27 (45.8%) patients, 24 (40.7%) patients, 19(32.2%) patients, and 7 (11.9%) patients, respectively. A retrospective cross-sectional study done by Monti et al. [44] in a sample of 102 geriatric inpatients, snoring was present in 46.9% of patients diagnosed as OSA. A study done in an Egyptian university hospital on 421 patients by Yousif et al. [45] found that snoring was also the most common presenting symptoms of sleep disorders present (84.6%). Regarding nocturia, it was represented by (40.7%) patients. Similar result was found in a research by Monti et al. [44] nocturia was in 39.1% in those diagnosed with OSA.
Obesity raises the potential for having both diabetes and OSA [46]. In this study, those who had been diagnosed with OSA (46 patients) were separated into two groups. Those having uncontrolled DM and controlled DM, comparing between both groups according to result of BMI. In patients having uncontrolled DM 10(30.3%) patients were found to have BMI < 35 and 23(69.7%) were found to have BMI ≥ 35.While in patients with controlled DM those with BMI < 35 were 11(84.6%) and 2(15.4%) patients with BMI ≥ 35.there was significant difference between both groups. This came in accordance with Nsr-Allah et al. [47]. When comparing uncontrolled diabetes patients to controlled diabetic patients and healthy people, there were significant differences in BMI with increased obesity. These findings support those of Piniés et al. [48]. Who predicted that people with a BMI more than 40 kg/m2 were seven times more likely than persons with a normal BMI to acquire diabetes. According to the findings of a meta-analysis, overweight, and obesity are strongly linked to OSA, and obesity is a significant risk factor for OSA [49].
In this study, a significant statistical difference was present when comparing between patients with OSA and those without OSA regarding WHR (p = 0.018). Visceral obesity has been associated with increased risk of T2DM [50]. Obese adults with T2DM who had OSA had more visceral fat, WHR was significantly increased in OSA in a study by Lim et al. [51] (p = 0.003, female p = 0.001).
The comparison between the two groups diagnosed as OSA or not OSA regarding result of STOP-BANG questionnaire, showed that STOP-BANG questionnaire score was statistically significantly higher among patients with OSA versus those without (p = 0.009). Moreover, a positive correlation between STOP-BANG questionnaire and ODI was found (P = 0.036). Similarly, Chung et al. [52] found that the likelihood of severe OSA increases as the STOP-BANG score rises to 7 or 8.
High Mallampati score (3 and 4) was seen in 69.6% of patients with OSA. Our results agreed with Rodrigues et al. [53, 54] and Eldaboosy et al., who showed that about 65% of studied OSA patients were grouped in classes III and IV.
Patients with T2DM are more likely to develop OSA, yet many go undetected. In our study, among the 59 patients enrolled, OSA was detected in 46(77.9%) patients using the overnight pulse oximetry. We considered patients diagnosed as OSA if ODI > 5 plus symptoms or > 15 without symptoms. ODI from 5 to 15 with symptoms was found in 13(22%) patients, ODI from 15 to 30 in 12(20.33%) patients, and ODI > 30 in 21 patients (35.59%). Similar results were found in a study that enrolled 54 diabetic outpatients with symptoms of sleep disorders using full PSG to diagnose OSA by Buyukaydin et al. [55].
Thirty 8 patients (73%) were women, men made up 14 patients (27 percent). The mean age was 56 ± 7 years. The BMI mean was 32.4 ± 5.3 kg/m2. OSAS was found in 35 patients (67.3%). Another study in Bangkok was done by Nimitphong et al. [56] enrolled 81 participants (33 men and 48 women) attending the outpatient clinic with mean age 54.7 years, and mean HbA1c of 7.6. The mean BMI was 28.3 kg/m2. Sixty-five participants (80.2%) were diagnosed with OSA. A Japanese study done by Kashine et al. also reported similar results [57]. A total of 40 Japanese patients with T2DM who had been hospitalized were included in the study. An experienced polysomnographic technologist manually assessed all of the recordings. The main finding was that Japanese T2DM patients had a significant prevalence of SDB (77.5%). Another study done by Chen et al. [58] investigated sleep disorders and wound healing in diabetic foot ulcer patients. They discovered that the prevalence of SDB was alarmingly high, with 92% identified with SDB and 34% with severe SDB, using PSG. This study showed higher prevalence of SDB in diabetic patients than ours. This could be attributed to the use of PSG to diagnose sleep disorders which is more accurate than overnight pulse oximetry in addition to the presence of uncontrolled DM which could be linked to foot ulcers.
In an Egyptian study done by Shoukri et al. [59], there were 107 T2DM patients who were referred for sleep disorders evaluation, with 62 men (57.94%) and 45 women (42.05%), age ranged from 42 to 72 years old. Based on the results of nighttime pulse oximetry (OPO) and the PSG-detected apnea–hypopnea index, the patients were divided into two groups (AHI). Sixty-eight patients (63.55%) had moderate to severe OSA with considerable oxygen desaturation (≥ 15 desaturation events/hour), while 39 patients (36.44%) had a lower ODI (< 15 events/h) and minimal or mild OSA with AHI (< 15 events/h). Another population-based study done by Elmasry et al. involved 2668 men aged 40–79 years old, and the prevalence of severe OSA, defined as apnea–hypopnea index (AHI) ≥ 20, was significantly higher in diabetic patients than in normoglycemic subjects (36 vs. 14.5%, P < 0.05) [60]. Lower prevalence rates were found in a study by Einhorn et al. [61]. There were 330 patients with T2DM who were sent to a diabetes clinic, and 279 of them finished the study. The presence of a sleep problem was determined using a single channel recording device that captures disturbed breathing events from a nasal cannula airflow signal. The prevalence rate was 36% overall. Because of differences in the population investigated, study designs, and the method and criteria used to diagnose OSA, the prevalence of OSA varies significantly between studies. Furthermore, because obesity and age are key risk factors for OSA, it is expected that the prevalence of OSA will rise as the obesity and elderly populations grow.
There is a bidirectional link between OSA and type 2DM: T2DM is a risk factor for OSA, and OSA is a also risk factor for T2DM [62]. In an Egyptian retrospective analysis of 244 patients with OSA by Sweed et al. [63], it was found that DM was present in 50% of the studied patients. DM was the second most common comorbidity after systemic HTN in this cohort of Egyptian patients with OSA. Furthermore, there were 332 incident cases of T2DM in a meta-analysis of 5953 patients with OSA who were followed for 2–16 years [64]. Those with moderate to severe OSA were more likely to be affected [65]. In a study by Li et al. when compared to non SDB, SDB was linked to a 1.33 greater risk of developing diabetes (95% CI, 1.05–1.67) [66].
The Wisconsin Sleep Cohort supplied a completely unique possibility to inspect the connection among diabetes and SDB with both a cross-sectional and prospective analysis. In the cross-sectional study, discovered that patients with an AHI of 15 or more were three to four times more likely to have diabetes than patients with an AHI of less than 5. Same relation remained even after controlling risk elements which includes age, sex, and body habit. However, in their prospective analysis, they found no statistically significant causative connection between the chance of having type II diabetes and the severity of OSA (at the beginning of the study) [17].
Among our studied patients, comparing between controlled and uncontrolled diabetic patients regarding presence of OSA. Thirty-three (86.8%) patients having uncontrolled glycemic level were found to have OSA, while 13(61.9%) patients with controlled glycemic level were found to have OSA. There was a significant difference comparing between both groups (p = 0.047). In a study by Aronsohn et al. [67], despite controlling obesity and a number of other possible confounders, there was a clear inverse relation between OSA severity and glucose control in adults with type 2 diabetes. The adjusted mean HbA1c was 1.49% higher in patients with mild OSA, 1.93% higher in patients with moderate OSA, and 3.69% higher in patients with severe OSA as compared to individuals without OSA. Several other studies have found that OSA and severity of OSA were linked to poor glycemic control (HbA1c) [68, 69]. Shoukri [59] et al. reported that patients in group 1 with a greater ODI and moderate to severe OSA had significantly higher HbA1c levels than patients in group 2 with minimal or mild OSA and an ODI of less than 15 desaturation events/h. In another Egyptian study by Agha et al. [70], 25 patients were enrolled with T2DM and OSA in the patient group, and 17 patients with T2DM but no OSA in the control group. The presence of OSA had an impact on glucose management in patients with treated T2DM, with HbA1c values significantly higher in the patients’ group than in the control group. Most studies imply a link between OSA and glycemic measurements in those with type 2 diabetes. However, confounding factors as age, sex, obesity, DM duration, and early OSA diagnosis all influence this connection.
The impact of CPAP usage on glycemic control was studied in a few research. After two months of CPAP therapy, one study found that insulin sensitivity had improved [71]. The effect of 24 weeks of CPAP on glycemic control in patients with poorly controlled type 2 diabetes and OSA was studied in a randomized controlled trial, discovered that CPAP prescription results in improving glycemic control and/or insulin resistance significantly when compared to standard care [72]. In a meta-analysis study, researchers looked at RCTs that examined the impact of CPAP on glycemic management and insulin resistance in those with type 2 DM and OSA. Based on these findings, it was shown that CPAP treatment considerably improved glycemic management and insulin resistance, as seen by lower HbA1c, fasting glucose, and HOMA-IR values, as well as significantly lower blood pressure levels [73].
Regarding advantages of our study, we screened for the presence of sleep apnea in patients with type 2 DM using a simple affordable device (overnight pulse oximetry). we also used a previously proven effective questionnaire (STOP-BANG) to add more to our results. On the other hand, there were some limitations, such as small number of our study sample. A full PSG would have been more accurate to confirm the diagnosis of OSA.
-
❖
In conclusion, patients with type 2 diabetes showed a significant high prevalence of OSA (77.9%). There was statistical significant higher prevelance of OSA among patients with uncontrolled DM when compared to patients with controlled DM so there was an association between glycemic control and the risk of OSA. Despite increased prevelance of OSA among uncontrolled diabetic patients there was no correlation between HbA1c and severity of OSA. STOP-BANG questionnaire was the only factor that was correlated with the severity of OSA (ODI) among type 2 diabetic patients in our study. Using multiple regression analysis, we found that variables were significantly related to presence of OSA, which were comorbidities, ESS, Mallampati score, STOP-BANG, and symptoms of sleep (nocturia and snoring). On the other hand there was no variable taking the upper hand and affecting the other variables. Overnight pulse oximetry is an easy and affordable method for screening type 2 DM for presence of OSA. We recommend performing similar studies on larger scale of patients using full polysomnography if possible.
-
➢
Increase awareness as well as patients education of the harmful effect of undiagnosed and untreated OSA in diabetic patients and its effect on diabetic control.
-
➢
All diabetic patients (type 2) should undergo screening for OSA (using STOP-BANG questionnaire and overnight pulse oximetry).
Availability of data and materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SDB:
-
Sleep disordered breathing
- OSA:
-
Obstructive sleep apnea
- PSG:
-
Polysomnography
- RDI:
-
Respiratory disturbance index
- AASM:
-
American Academy of Sleep Medicine
- PAP:
-
Positive airway pressure
- EDS:
-
Excessive daytime sleepiness
- BMI:
-
Body mass index
- REM:
-
Rapid eye movement
- CIH:
-
Chronic intermittent hypoxia
- AHI:
-
Apnea hypopnea index
- ESS:
-
Epworth Sleepiness Scale
- WHR:
-
Waist hip ratio
- T2DM:
-
Type two diabetes mellitus
- HbA1c :
-
Glycated hemoglobin
- CPAP:
-
Continuous positive airway pressure
- WHO:
-
World health organization
- DKA:
-
Diabetes ketoacidosis
- FBG:
-
Fasting plasma glucose
- OPO:
-
Overnight pulse oximetry
- ODI:
-
Oxygen desaturation index
- HTN:
-
Hypertension
- IHD:
-
Ischemic heart diseases
- AF:
-
Atrial fibrillation
- CKD:
-
Chronic kidney diseases
- FBS:
-
Fasting blood sugar
References
Fleetham J, Ayas N, Bradley D, Ferguson K, Fitzpatrick M, George C et al (2006) Canadian Thoracic Society guidelines: diagnosis and treatment of sleep disordered breathing in adults. Can Respir J 13(7):387–392
Kapur VK, Auckley DH, Chowdhuri S, Kuhlmann DC, Mehra R, Ramar K et al (2017) Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med 13(3):479–504
Mandereau-Bruno L, Léger D, Delmas MC (2021) Obstructive sleep apnea: a sharp increase in the prevalence of patients treated with nasal CPAP over the last decade in France. PLoS ONE 16(1):e0245392
Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC et al (2017) Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev 34:70–81
Tufik S, Santos-Silva R, Taddei JA, Bittencourt LR (2010) Obstructive sleep apnea syndrome in the Sao Paulo Epidemiologic Sleep Study. Sleep Med 11(5):441–446
Reddy EV, Kadhiravan T, Mishra HK, Sreenivas V, Handa KK, Sinha S et al (2009) Prevalence and risk factors of obstructive sleep apnea among middle-aged urban Indians: a community-based study. Sleep Med 10(8):913–918
Jun J, Savransky V, Nanayakkara A, Bevans S, Li J, Smith PL et al (2008) Intermittent hypoxia has organ-specific effects on oxidative stress. Am J Physiol Regul Integr Comp Physiol 295(4):R1274–R1281
O’Halloran KD (2016) Chronic intermittent hypoxia creates the perfect storm with calamitous consequences for respiratory control. Respir Physiol Neurobiol 226:63–67
Schwartz AR, Patil SP, Laffan AM, Polotsky V, Schneider H, Smith PL (2008) Obesity and obstructive sleep apnea: pathogenic mechanisms and therapeutic approaches. Proc Am Thorac Soc 5(2):185–192
Ness-Abramof R, Apovian CM (2005) Drug-induced weight gain. Drugs Today (Barc) 41(8):547–555
Gagliardi L, Wittert G (2007) Management of obesity in patients with type 2 diabetes mellitus. Curr Diabetes Rev 3(2):95–101
Leslie WS, Hankey CR, Lean ME (2007) Weight gain as an adverse effect of some commonly prescribed drugs: a systematic review. QJM 100(7):395–404
Gozal D, Ham SA, Mokhlesi B (2016) Sleep apnea and cancer: analysis of a nationwide population sample. Sleep 39(8):1493–1500
Ryan S (2017) Adipose tissue inflammation by intermittent hypoxia: mechanistic link between obstructive sleep apnoea and metabolic dysfunction. J Physiol 595(8):2423–2430
Tahrani AA (2015) International Textbook of Diabetes Mellitus, 4th edn. John Wiley & Sons, USA
Guo LX, Zhao X, Pan Q, Sun X, Li H, Wang XX et al (2015) Effect of continuous positive airway pressure therapy on glycemic excursions and insulin sensitivity in patients with obstructive sleep apnea-hypopnea syndrome and type 2 diabetes. Chin Med J (Engl) 128(17):2301–2306
Reichmuth KJ, Austin D, Skatrud JB, Young T (2005) Association of sleep apnea and type II diabetes: a population-based study. Am J Respir Crit Care Med 172(12):1590–1595
Pamidi S, Tasali E (2012) Obstructive sleep apnea and type 2 diabetes: is there a link? Front Neurol 3:126
Foster GD, Sanders MH, Millman R, Zammit G, Borradaile KE, Newman AB et al (2009) Obstructive sleep apnea among obese patients with type 2 diabetes. Diabetes Care 32(6):1017–1019
American Diabetes Association (2015) Initial evaluation and diabetes management planning. Diabetes Care 38(Suppl):S17–S19
American Academy of Sleep Medicine (AASM) (2013) Patients with Type 2 Diabetes or Hypertension Must Be Evaluated for Sleep Apnea. AASM, Darien, IL
Chiquete E, Ruiz-Sandoval JL, Ochoa-Guzmán A, Sánchez-Orozco LV, Lara-Zaragoza EB, Basaldúa N et al (2014) The Quételet index revisited in children and adults. Endocrinol Nutr 61(2):87–92
Cakirer B, Hans MG, Graham G, Aylor J, Tishler PV, Redline S (2001) The relationship between craniofacial morphology and obstructive sleep apnea in whites and in African-Americans. Am J Respir Crit Care Med 163(4):947–950
Nishida C, Ko GT, Kumanyika S (2010) Body fat distribution and noncommunicable diseases in populations: overview of the 2008 WHO Expert Consultation on Waist Circumference and Waist-Hip Ratio. Eur J Clin Nutr 64(1):2–5
Nuckton TJ, Glidden DV, Browner WS, Claman DM (2006) Physical examination: Mallampati score as an independent predictor of obstructive sleep apnea. Sleep 29(7):903–908
Johns MW (1991) A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 14(6):540–545
Chung F, Yegneswaran B, Liao P, Chung SA, Vairavanathan S, Islam S et al (2008) STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology 108(5):812–821
Festic N, Zuberi M, Bansal V, Fredrickson P, Festic E (2019) Correlation between oxygen saturation and pulse tracing patterns on overnight oximetry with normal desaturation index is an independent predictor of obstructive sleep apnea. J Clin Sleep Med 15(2):195–200
Sacks DB (1994) Carbohydrates. In: Burtis CA, Ashwood ER (eds) Tietz textbook of clinical chemistry, 2nd edn. WB sanders, Philadelphia, pp 935–949
The University of Oxford. HOMA Calculator 2016. Available from: https://www.dtu.ox.ac.uk/homacalculator/. Accessed in: Sep, 2021.
American Diabetes Association (2013) Standards of medical care in diabetes–2013. Diabetes Care 36(Suppl 1):S11-66
Burtis CA, Ashwood ER (1994) Tietz textbook of clinical chemistry, 2nd edn. WB Saunders, Philadelphia, pp 1017–1089
Kirkpatrick L, Feeney B (2013) A simple guide to IBM SPSS statistics for version 20.0. Student ed. Wadsworth Cengage Learning, Belmont, Calif
Jehan S, Myers AK, Zizi F, Pandi-Perumal SR, Jean-Louis G, McFarlane SI (2018) Obesity, obstructive sleep apnea and type 2 diabetes mellitus: epidemiology and pathophysiologic insights. Sleep Med Disord 2(3):52–58
Megahed FI, Farg HK (2020) Most effiecnt factors affecting glycemic control of type ii diabetic patients attending Suez Canal University hospitals in Egypt applying stepwise regression. LOJ Med Sci 4(5):442–450
Dussa KN (2017) Impact of pharmaceutical care on economic Clinical and humanistic outcomes in patients With diabetes mellitus Type II. JCHPS 1:29–38
Mufunda E, Ernersson Å, Hjelm K (2018) Limited knowledge of diabetes in patients attending an outpatient diabetes clinic at a referral hospital in Zimbabwe: a cross-sectional study. Pan Afr Med J 29:144
Juel K, Christensen K (2008) Are men seeking medical advice too late? Contacts to general practitioners and hospital admissions in Denmark 2005. J Public Health (Oxf) 30(1):111–113
Souliotis K, Koutsovasilis A, Vatheia G, Golna C, Nikolaidi S, Hatziagelaki E et al (2020) Profile and factors associated with glycaemic control of patients with type 2 diabetes in Greece: results from the diabetes registry. BMC Endocr Disord 20(1):16
Arnold SV, Goyal A, Inzucchi SE, McGuire DK, Tang F, Mehta SN et al (2017) Quality of care of the initial patient cohort of the diabetes collaborative registry ®. J Am Heart Assoc 6(8):e005999
Ji LN, Lu JM, Guo XH, Yang WY, Weng JP, Jia WP et al (2013) Glycemic control among patients in China with type 2 diabetes mellitus receiving oral drugs or injectables. BMC Public Health 13:602
Borgharkar SS, Das SS (2019) Real-world evidence of glycemic control among patients with type 2 diabetes mellitus in India: the TIGHT study. BMJ Open Diabetes Res Care 7(1):e000654
Ufuoma C, Godwin YD, Kester AD, Ngozi JC (2016) Determinants of glycemic control among persons with type 2 diabetes mellitus in Niger Delta. Sahel Med J 19(4):190–195
Monti A, Doulazmi M, Nguyen-Michel VH, Pautas E, Mariani J, Kinugawa K (2021) Clinical characteristics of sleep apnea in middle-old and oldest-old inpatients: symptoms and comorbidities. Sleep Med 82:179–185
Yousif M, El-Helbawy R (2013) A six-year sleep lab experience in an Egyptian University Hospital. Egypt J Chest Dis Tuberc 62(4):717–722
Lloyd LJ, Langley-Evans SC, McMullen S (2012) Childhood obesity and risk of the adult metabolic syndrome: a systematic review. Int J Obes (Lond) 36(1):1–11
Nsr-Allah AEM, El-Osh S, Ahmed AM, Hazem S (2019) Salivary α2-macroglobulin as a marker for glycemic control in patients with type 2 diabetes mellitus. Egypt J Intern Med 31(2):155–163
Piniés JA, González-Carril F, Arteagoitia JM, Irigoien I, Altzibar JM, Rodriguez-Murua JL et al (2014) Development of a prediction model for fatal and non-fatal coronary heart disease and cardiovascular disease in patients with newly diagnosed type 2 diabetes mellitus: the Basque Country Prospective Complications and Mortality Study risk engine (BASCORE). Diabetologia 57(11):2324–2333
Dong Z, Xu X, Wang C, Cartledge S, Maddison R, Islam SMS (2020) Association of overweight and obesity with obstructive sleep apnoea: a systematic review and meta-analysis. Obes Med 17:100185
Vgontzas AN, Papanicolaou DA, Bixler EO, Hopper K, Lotsikas A, Lin HM et al (2000) Sleep apnea and daytime sleepiness and fatigue: relation to visceral obesity, insulin resistance, and hypercytokinemia. J Clin Endocrinol Metab 85(3):1151–1158
Lim YH, Choi J, Kim KR, Shin J, Hwang KG, Ryu S et al (2014) Sex-specific characteristics of anthropometry in patients with obstructive sleep apnea: neck circumference and waist-hip ratio. Ann Otol Rhinol Laryngol 123(7):517–523
Chung F, Abdullah HR, Liao P (2016) STOP-Bang questionnaire: a practical approach to screen for obstructive sleep apnea. Chest 149(3):631–638
Rodrigues MM, Dibbern RS, Goulart CW (2010) Nasal obstruction and high Mallampati score as risk factors for Obstructive Sleep Apnea. Braz J Otorhinolaryngol 76(5):596–599
Eldaboosy S, Eldosky I, Nour S (2021) Modified Mallampati score as a predictor for the presence and the severity of obstructive sleep apnea in snoring patients. Prensa Med Argent 107:3
Buyukaydin B, Akkoyunlu ME, Kazancioglu R, Karakose F, Ozcelik HK, Erkoc R et al (2012) The effect of sleep apnea syndrome on the development of diabetic nephropathy in patients with type 2 diabetes. Diabetes Res Clin Pract 98(1):140–143
Nimitphong H, Siwasaranond N, Sritara C, Saetung S, Chailurkit LO, Chirakalwasan N et al (2019) The differences in the relationship between obstructive sleep apnea severity and trabecular bone score in men and women with type 2 diabetes. J Clin Transl Endocrinol 16:100193
Kashine S, Kishida K, Funahashi T, Nakagawa Y, Otuki M, Okita K et al (2010) Characteristics of sleep-disordered breathing in Japanese patients with type 2 diabetes mellitus. Metabolism 59(5):690–696
Chen L, Ma W, Covassin N, Chen D, Zha P, Wang C et al (2021) Association of sleep-disordered breathing and wound healing in patients with diabetic foot ulcers. J Clin Sleep Med 17(5):909–916
Shoukri AM (2021) Correlation between nocturnal oxygen desaturation and glycemic control in diabetic patients with obstructive sleep apnea. Egypt J Bronchol 15(1):1–6
Elmasry A, Lindberg E, Berne C, Janson C, Gislason T, Awad Tageldin M et al (2001) Sleep-disordered breathing and glucose metabolism in hypertensive men: a population-based study. J Intern Med 249(2):153–161
Einhorn D, Stewart DA, Erman MK, Gordon N, Philis-Tsimikas A, Casal E (2007) Prevalence of sleep apnea in a population of adults with type 2 diabetes mellitus. Endocr Pract 13(4):355–362
Fredheim JM, Rollheim J, Omland T, Hofsø D, Røislien J, Vegsgaard K et al (2011) Type 2 diabetes and pre-diabetes are associated with obstructive sleep apnea in extremely obese subjects: a cross-sectional study. Cardiovasc Diabetol 10:84
Sweed RA, Hassan S, ElWahab NHA, Aref SR, Mahmoud MI (2019) Comorbidities associated with obstructive sleep apnea: a retrospective Egyptian study on 244 patients. Sleep Breath 23(4):1079–1085
Wang X, Bi Y, Zhang Q, Pan F (2013) Obstructive sleep apnoea and the risk of type 2 diabetes: a meta-analysis of prospective cohort studies. Respirology 18(1):140–146
Seicean S, Kirchner HL, Gottlieb DJ, Punjabi NM, Resnick H, Sanders M et al (2008) Sleep-disordered breathing and impaired glucose metabolism in normal-weight and overweight/obese individuals: the Sleep Heart Health Study. Diabetes Care 31(5):1001–1006
Li X, Sotres-Alvarez D, Gallo LC, Ramos AR, Aviles-Santa L, Perreira KM et al (2021) Associations of sleep-disordered breathing and insomnia with incident hypertension and diabetes. The Hispanic community health study/study of Latinos. Am J Respir Crit Care Med 203(3):356–65
Aronsohn RS, Whitmore H, Van Cauter E, Tasali E (2010) Impact of untreated obstructive sleep apnea on glucose control in type 2 diabetes. Am J Respir Crit Care Med 181(5):507–513
Drager LF, Queiroz EL, Lopes HF, Genta PR, Krieger EM, Lorenzi-Filho G (2009) Obstructive sleep apnea is highly prevalent and correlates with impaired glycemic control in consecutive patients with the metabolic syndrome. J Cardiometab Syndr 4(2):89–95
Kosseifi S, Bailey B, Price R, Roy TM, Byrd RP, Peiris AN (2010) The association between obstructive sleep apnea syndrome and microvascular complications in well-controlled diabetic patients. Mil Med 175(11):913–916
Agha MA, Shehab-Eldin W, Helwa MA (2019) Obstructive sleep apnea in patients with type 2 diabetes mellitus. Egypt J Chest Dis Tuberc 68(4):560–566
Weinstock TG, Wang X, Rueschman M, Ismail-Beigi F, Aylor J, Babineau DC et al (2012) A controlled trial of CPAP therapy on metabolic control in individuals with impaired glucose tolerance and sleep apnea. Sleep 35(5):617–625
Martínez-Ceron E, Fernández-Navarro I, Garcia-Rio F (2016) Effects of continuous positive airway pressure treatment on glucose metabolism in patients with obstructive sleep apnea. Sleep Med Rev 25:121–130
Shang W, Zhang Y, Wang G, Han D (2021) Benefits of continuous positive airway pressure on glycaemic control and insulin resistance in patients with type 2 diabetes and obstructive sleep apnoea: a meta-analysis. Diabetes Obes Metab 23(2):540–548
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Contributions
Rania Ahmed Sweed directed the practical part of the research, presented the results, and wrote the manuscript. Nashwa Hassan Abd El Wahab decided the main idea of the research and the methodology, and revised the whole manuscript. Dina Mohsen Shetta performed the practical part, statistics, and data collection. Mona Saeed El Hooshy guided the practical part and revised the manuscript. Eman Youssef Morsy guided the practical part and revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was in accordance with the ethical standards of the institutional research committee (Alexandria Faculty of Medicine) and with the 1964 Helsinki declaration.
Consent for publication
Informed consent was obtained from all individual participants included in the study.
Competing interests
All authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sweed, R.A., Wahab, N.H.A.E., El Hooshy, M.S. et al. Obstructive sleep apnea in patients with type 2 diabetes mellitus in Egyptian population. Egypt J Bronchol 17, 55 (2023). https://doi.org/10.1186/s43168-023-00224-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43168-023-00224-3