
Abstract
Background
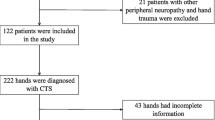
Electrodiagnostic tests (EDX) are the most frequent and applicable studies in early diagnosis of carpal tunnel syndrome (CTS), but the definitive sensitive and specific tests are still under study. We aimed to evaluate the role of the median versus ulnar palmar mixed nerve study (Mix M-U), and its sensitivity in comparison to other provocative comparison studies, in supporting the early diagnosis of CTS. This cross-sectional study included 142 idiopathic early CTS hands from 100 patients and 71 hands from 50 healthy subjects as a control group. We did routine median motor and sensory studies and 4 comparative tests namely median versus radial sensory study (MVR), Mix M-U, median versus ulnar sensory study (MVU), and median versus ulnar lumbrical-interossei motor study (LU-IN).
Results
The routine median motor and sensory latency and amplitude showed a statistically significant difference between CTS and control groups as (p< 0.05) and a highly statistically significant difference between the 2 groups as regards the 4 comparative tests as (p< 0.0001). The specificities of all the 4 comparative tests were higher than 90%. MVR test had the highest sensitivity (92.2%) and followed by Mix M-U study (82.2%) and MVU (78.7%), and the least sensitive test was the LM-IN (66.9%).
Conclusions
Although the patients’ results fall within the normal range according to the reference range in the literature, it showed a statistically significant difference when compared to controls. A high percentage of those symptomatic patients showed results of typical CTS when tested with the comparative studies so there is a need to use these sensitive tests to diagnose cases with early CTS. According to sensitivity studies, the selection of which tests to do in order is a challenging choice. For the diagnosis of cases with early CTS with a normal ordinary motor and sensory studies, MVR comparative technique appeared as the best sensitive and specific provocative electrophysiological test followed by the Mix M-U test. We recommend the use of a combination of both tests first in the diagnosis of early CTS and if one of them was negative we can use the other comparative studies MVU and then LM-IN studies.
Similar content being viewed by others


Background
Carpal tunnel syndrome (CTS) is a median nerve entrapment at the wrist. It is the most prevalent neuropathy in the body in which the median nerve is compressed under the transverse carpal ligament [1,2,3,4]. CTS is evaluated by the recognition of median nerve conduction studies affection over the carpal tunnel. These conduction studies are the key in the verification of the proof of uncertain cases of CTS and assess the physiological status of the median nerve across the carpal tunnel [5, 6]. The results of EDX studies give rise to interchange in the endorsed treatment of CTS [7].
There are a diversity of sensory and motor conduction studies that range in sensitivity and specificity. The changes in the sensory studies occur earlier than the motor studies and they are more sensitive. The motor studies are routinely documented in progressive CTS and in sufferers from peripheral polyneuropathy [2, 8]. The motor studies that evaluate the affection of the median nerve over the wrist are the median motor conduction study test (MMCS) with poor sensitivity for the diagnosis of CTS, LM-IN motor study that has a better sensitivity than the median conduction study test [3], and the median-ulnar medial thenar motor latency comparative study which is the most sensitive and specific motor study for the diagnosis of CTS than the previous two studies [2, 3, 9, 10]. The sensory conduction studies that evaluate the affection of the median nerve across the wrist are the routine median sensory nerve conduction test (MSCS), median versus ulnar sensory test (MVU) recorded from digit four, and median versus radial sensory test (MVR) recorded from the thumb and the median versus ulnar palmar mixed test (Mix M-U) [2, 3].
The differentiation of the several conduction studies identification sensitivity demonstrates that the sensory studies are preferred than motor studies and the comparative study techniques between median and ulnar or median and radial nerves are more sensitive than routine sensory study in the same hand [11].
This work aimed to evaluate the role of the median versus ulnar palmar mixed nerve study, and its sensitivity in comparison to other provocative comparison studies, in supporting the early diagnosis of CTS.
Methods
Study design, setting, and participants
Cross sectional comparative study included 100 patients of idiopathic early CTS. They were selected from the patients that attended the electrophysiology unit of Physical Medicine, Rheumatology and Rehabilitation department- Al-Mataria Teaching Hospital after explaining the procedure to them and taking from them a written consent. Fifty apparently healthy volunteers were included in the study as a control group. Diagnosis of CTS was in accordance with the criteria proposed by Keith et al. [12] as the presence of nocturnal or activity-related pain or dysthesia limited to the hand, sensory deficit in median nerve distribution, or positive Phalen’s or Tinel’s sign. Isolated atrophy of the abductor pollicis brevis (APB) muscle was excluded from the criteria. Inclusion criteria were adult patients fulfilling the clinical criteria of idiopathic CTS.
Exclusion criteria: Subjects with any neurological deficits including severe CTS, peripheral neuropathy, radiculopathy, diabetes mellitus, endocrine or metabolic disorders, and local steroid injection history or previous decompression surgery of the CTS were excluded from the study.
Methods
All participants in the study were subjected to:
- Full history taking including disease duration and symptoms of CTS, local clinical hand examination, and neurological examination.
- Electrophysiological studies were conducted using nerve conduction and EMG apparatus named Medtronic Dantek Keypoint 2 channels (DANTEK, Denmark). Skin temperature was maintained 32–34°C by using an infra-red lamp in cold hands and measured by a digital thermometer. Surface cup electrodes were applied for the recording of motor tests, the ring and the bar electrodes for the recording of sensory tests, and bipolar stimulator electrodes were used for stimulation. The ground electrode was placed between the stimulator and the recording electrodes. A measuring tape with a 1-mm measure was used to calculate the conduction distance. Supramaximal stimulation was applied.
- In motor conduction studies we used the belly-tendon montage method as the active recording electrode (G1) was placed on the muscle belly and the reference recording electrode (G2) on its tendon. The filter bandwidth was 10 Hz–10 kHz, sensitivity was 5 mV/ division, and sweep speed was 5 ms/division. The production current capacity of the stimulator was 100 mA with a pulse duration 0.2 ms. The measuring parameters was described in Table 1.
- In sensory conduction studies, the filter bandwidth was 20Hz–2kHz, the sensitivity was 20 μV/division, and the sweep speed was 2 ms/division. The production current capacity of the stimulator was 100 mA with a pulse duration of 0.2 ms. Averaging of signals was used. The measuring parameters of the sensory nerve action potential (SNAP) included peak latency (PL) in ms, amplitude in microvolts (μV ), and conduction velocity (CV) in m/s. Ring electrodes were placed on the studied digit as the active recording electrode (G1) was placed proximally and the reference recording electrode (G2) was placed 3–4cm distally. In studying the orthodromic Mix M-U test we used the bar electrode as a recording electrode and it was placed on the examined nerve.
Electrophysiological routine studies and provocative comparison techniques performed in the study were shown in Table 1.
-
1)
Median motor nerve conduction test (MMCS)
-
2)
Median sensory nerve conduction test (MSCS)
-
3)
Sensory median versus radial test (MVR)
-
4)
Sensory median versus ulnar test (MVU)
-
5)
Motor median versus ulnar lumbrical/interossei test (LM-IN)
-
6)
Sensory Median versus ulnar palmar mixed nerve test (Mix M-U)
Motor and sensory ulnar nerve conduction studies were done as a routine in all subjects to exclude neuropathy. The protocol of recording and stimulation of ulnar nerve conduction study was according to Preston and Shapiro [10].
The patients of early CTS according to bland scale [14] were defined as cases with a clinically established diagnosis of CTS with normal routine motor and sensory median studies with the presence of at least two abnormal sensitive comparative test (from no. 2 to 6).
To assess the percentage of affection of electrophysiological comparative tests in early CTS hands, we grouped the patients according to the median sensory latency cut-off: group 1 (<3.7ms), group 2 (<3.6 ms), group 3 (<3.5), group 4 (<3.4), group 5 (<3.3), group 6 (<3.2), and group 7 (<3.1) considering each cut off point as a reference to see the number of affected hands to get the most sensitive test.
Statistical analysis of data was calculated and tabulated by the application of the SPSS (V. 25) software (USA). The descriptive statistics are described as the minimum, maximum, mean, and SD, and the analysis of comparison parameters was done by using the independent Student t-test between the means. Statistical significance was measured to any P value less than or equal to 0.05. Sensitivity, specificity, and positive and negative predictive values were assigned and were extracted as percentages for easiness of elucidation. The sensitivity, specificity, and the area under the curve (AUC) were calculated using the receiver operating characteristic curves (ROC).
Results
One hundred and forty-two hands established clinically as CTS existed from 100 patients were included in the study. The mean age was 37.66±8.8 (18 to 60) years, 84% were females and 16% were males. Seventy one asymptomatic hands existed from 50 volunteers were included in the study as a control group. The mean age was 35.08±11.42 (18 to 61) years, 80% were females and 20% were males. There was no difference significantly between CTS hands and the control group concerning age (p=0.128) or gender (p=0.543).
A total of 42 (42%) patients had bilateral CTS and 58 (58%) patients had unilateral CTS. Clinical symptoms were presented in the right hands in 80 (56.3%) patients and the left hands in 62(43.6%). Ninety-seven hands (69%) of the 142 symptomatic hands that were exposed to EDX studies had nocturnal dysesthesia in the distribution of the median nerve, 45 (31.7%) hands had painful dysesthesia related to activity. Seventy-six (53.5%) hands had a sensory deficit in the distribution of the median nerve. Phalen’s test was positive in 92 (64.8%) hands and 54 (38.02%) hands had positive Tinel’s test. The clinical features of the CTS hands and control subjects were described in Table 2.
As regards the EDX study test, the distal motor latency of MN was delayed significantly in CTS hands compared to normal hands (p=0.022). The amplitude was reduced significantly in CTS hands compared to normal hands (p=0.0008), while there was no difference in motor conduction velocity between the 2 groups (p=0.896). The peak sensory latency of MN was delayed significantly in hands with CTS compared to normal hands (p<0.0001). The sensory amplitude was reduced significantly in CTS hands compared to normal hands (p=0.011), while there was no difference in sensory conduction velocity between the 2 groups (p=0.251).
All 4 provocative comparative tests, MVR, Mix M-U, MVU, and LM-IN, were significantly higher in CTS hands than in control hands (p<0.0001). There were no significant differences between patients and controls as regards ulnar motor and sensory studies (p> 0.05). A comparison of electrophysiological test variables between CTS hands and normal hands was shown in Table 3 and Fig. 1.

Control group at the left showed normal neurophysiological parameters of median, ulnar motor, and sensory studies; normal 4 comparative tests. CTS group at the right showed normal neurophysiological parameters of median, ulnar motor, and sensory studies; abnormal LM-IN (> 0.5); abnormal MVR (>0.4); abnormal Mix U-M (>0.4); and normal MVU (≤0.5). The traces from above downwards [median motor wrist, elbow, and palm (control only), LM-IN (2 traces), routine median sensory, MVR(2 traces), Mix M-U (2 traces), routine ulnar sensory, and MVU (last 2 traces)

Median versus ulnar mixed orthodromic sensory study technique. a MN recording electrodes at the wrist with G1 placed over the middle of the wrist between FCR and PL tendons and G2 placed 3–4 cm proximally. Stimulating electrode in the palm: 8 cm from the G1 on a line drawn from the median wrist to the web space between the index and middle fingers. b UN recording electrodes at the wrist with G1 placed over the medial wrist, adjacent to the FCU tendon, and G2 placed 3–4cm proximally. Stimulating electrode in the palm: 8cm from the active recording electrode on a line drawn from the ulnar wrist space between the ring and little fingers
Table 4 demonstrates the diagnostic value of provocative electrophysiological comparative tests used in the study for the diagnosis of early CTS. The tests of the highest sensitivity in confirming CTS were MVR, then Mix M-U and MVU studies (92%, 85.2%, and 78%, respectively). The lowest sensitive test in confirming early CTS was the LM-IN study (66.9%). All four comparative tests showed a specificity of more than 90%.
At the normal median sensory cut-off of less than 3.7, 131 (92.9%) hands had an abnormal MVR test, 111 (78.2%) hands had an abnormal MVU test, 95 (67.4%) had an abnormal LM-IN test, and 121 (85%) hands had an abnormal mix M-U test. We carried out the percentage of affection of the 4 comparative tests when median distal sensory latency (MDSL) was below 3.6ms (121 hands), below 3.5ms (102 hands), below 3.4ms (70 hands), below 3.3ms (52 hands), below 3.2ms (29 hands), and below 3.1ms (20 hands), as shown in Table 5. The percentage of affection of the MVR study showed the highest value in spite of that the 7 cut-off sensory latency values, ranging from 92.9 to 65%, followed by the Mix M-U study as it gained the second highest value ranging from 85.2 to 55%, then the MVU study reached the third highest value ranging from 78.2 to 45%. The LM-IN test reached the smallest value ranging from 67.4 to 15% as shown in Table 5. The percentage of affection of the 142 CTS hands when two to four comparative studies were found abnormal was shown in Table 6. When just 2 comparative tests were affected, the most frequent interrelation was MVR plus Mix M-U and MVR plus MVU studies.
Discussion
Our study was designed to evaluate the role of the median versus ulnar palmar mixed nerve study, and its sensitivity in comparison to other provocative comparison studies, in assisting the early diagnosis of CTS. Our results clearly demonstrated that the electrophysiological provocative comparison techniques MVR, MVU, LM-IN, and Mix M-U mainly the sensory tests are more sensitive and better than the routine motor and sensory median latency for early diagnosis of CTS, as reported by AAEM Quality Assurance Committee [11]. The sensitivity of sensory techniques namely MVR, Mix M-U, and MVU are exceeding 78.2% of abnormality when MDSL is still lower than the upper limit of normal (ULN), considered as 3.7 ms [15, 16]. When considering the upper limit of normal for MDSL as below 3.6 ms to below 3.1 ms, the percentage of affection of the MVR study was the most sensitive value ranging from 92.9 to 65% following by the Mix M-U study as the second high value ranging from 85.2 to 55%. MVU and LM-IN studies showed less sensitivity ranging from 78.2 to 45% and from 67.4 to 15%, respectively. We reported that when at least 2 comparative tests were affected, the most frequent linked affected tests were MVR plus Mix M-U and MVR plus MVU.
There were wide abnormal variation reports of the 4 provocative comparative tests. The abnormal percentage for MVR is described by Johnson et al. [17] (100%), Kouyoumdjian and Morita [18] (97.8%), Andary et al. [19] (90%), Cioni et al. [20] (89%), Pease et al. [21] (87.2%), Carrol [22] (59.6%), White et al. [23] (58%), and Jackson and Clifford [13] (44%). In our study, this technique was the most sensitive test in diagnosing early CTS and its sensitivity was (92.9%). The second sensitive test in our study was the Mix M-U study as its sensitivity was (85.2%). Reports of aberrancy percentage for Mix M-U are described by Kouyoumdjian & Morita [18] (89.4%), Andary et al. [19] (61%), Mills [24] (60%), and Jackson and Clifford [13] (30%). The third sensitive test in our study was the MVU study as its sensitivity was (78.2%). Reports of aberrancy percentage for MVU are described by Charles et al. [25] (100%), Cioni et al. [20] (99.2%), Monga et al. [26] (93%), Pease et al. [21] (88.6%), Lauritzen et al. [27] (87%), Kouyoumdjian and Morita [18] (85.2%), Uncini et al. [28] (78%), Jackson and Clifford [13] (44%), and Andary et al. [19] (42%). The least sensitive test in our study was the LM-IN study as its abnormal percentage was (67.4%). Reports of aberrancy percentage for LM-IN are described by Yilmaz et al. [29] (76%), Boonyapisit et al. [30] (92%), Kodama et al. [31] (92%), Preston and Logigian (88%) [32], and Ozben et al. [33] (89.4%). The wide range of abnormality differences in various reports was advocated because in a few electrophysiological labs, the upper limit of normal practice for MDSL could be contrasting. The changes in cut-off latencies in comparative tests for CTS diagnosis could change the sensitivity or specificity-induced false negative or positive results. The wide variation and cut-off latencies abnormality reported revealed that there was no concurrence suggesting only one test to be superior to others.
The precise procedure to diagnose CTS was to merge the clinical demonstrations with the consequences of electrodiagnostic studies [34]. For that reason, all the electrodiagnostic tests evaluating CTS were supportive to each other. There was no isolated test that could take the advantage over the others but the combination of the comparative tests can be used to complement one another in the diagnosis of patients with CTS who had normal routine sensory and motor studies [35]. The limitation of our study was the small number of patients of grade 1 CTS with normal motor and sensory routine studies and at the same time having only two abnormal comparative tests., this was perchance due to the medical attention of CTS patients about their disease with preliminary looking for medical guidance.
Conclusion
Although the patients’ results fall within the normal range according to the reference range in the literature, it showed a statistically significant difference when compared to controls. A high percentage of those symptomatic patients showed results of typical CTS when tested with the comparative studies so there is a need to use these sensitive tests to diagnose cases with early CTS. According to sensitivity studies, the selection of which tests to do in order is a challenging choice. For the diagnosis of cases with early CTS with a normal ordinary motor and sensory studies, MVR comparative technique appeared as the best sensitive and specific provocative electrophysiological test followed by the Mix M-U test. We recommend the use of a combination of both tests first in the diagnosis of early CTS, and if one of them was negative, we can use the other comparative studies MVU and then LM-IN studies.
Availability of data and materials
All data generalized and/or analyzed during the current study are available from the author upon reasonable request.
Abbreviations
- EDX:
-
Electrodiagnostic tests
- MVR:
-
Median versus radial sensory study
- MVU:
-
Median versus ulnar sensory study
- Mix M-U:
-
Median versus ulnar palmar mixed nerve study
- LM-IN:
-
Median versus ulnar lumbrical-interossei motor study
- PPV:
-
Positive predictive value
- NPV:
-
Negative predictive value
- AUC:
-
Area under curve
- MN:
-
Median nerve
- UN:
-
Ulnar nerve
- MMCS:
-
Median motor nerve conduction study
- MSCS:
-
Median sensory nerve conduction study
- MDSL:
-
Median distal sensory latency
- APB:
-
Abductor Pollicis Brevis muscle
- DL:
-
Distal latency
- PL:
-
Peak latency
- CV:
-
Conduction velocity
- MCP:
-
Metacarpo-phalangeal joint
- IPJ:
-
Interphalangeal Joint
- ULN:
-
Upper limit of normal
References
Kiernan MC, Mogyoros I, Burke D (1999) Conduction block in carpal tunnel syndrome. Brain 122:933–941
Werner RA, Andary M (2011) Electrodiagnostic evaluation of carpal tunnel syndrome. Muscle Nerve 44:597–607
Stevens JC (1997) AAEM minimonograph #26: the electrodiagnosis of carpal tunnel syndrome. American Association of Electrodiagnostic Medicine. Muscle Nerve 20(12):1477–1486
Uchiyama S, Itsubo T, Nakamura K, Kato H, Yasutomi T, Momose T (2010) Current concepts of carpal tunnel syndrome: pathophysiology, treatment, and evaluation. J Orthop Sci 15:1–13
Ibrahim I, Khan WS, Goddard N, Smitham P (2012) Carpal tunnel syndrome: a review of the recent literature. Open Orthop J 6(Suppl 1):69–76
Ntani G, Palmer KT, Linaker C, Harris EC, Van der Star R, Cooper C et al (2013) Symptoms, signs and nerve conduction velocities in patients with suspected carpal tunnel syndrome. BMC Musculoskelet Disord 14:242
Becker SJ, Makanji HS, Ring D (2014) Changes in treatment plan for carpal tunnel syndrome based on electrodiagnostic test results. J Hand Surg Eur 39:187–193
Löscher WN, Auer-Grumbach M, Trinka E, Ladurner G, Hartung HP (2000) Comparison of second lumbrical and interosseus latencies with standard measures of median nerve function across the carpal tunnel: a prospective study of 450 hands. J Neurol 247:530–534
Wilder Smith EP, Chan YH, Kannan TA (2007) Medial thenar recording in normal subjects and carpal tunnel syndrome. Clin Neurophysiol 118:57–61. https://doi.org/10.1016/j.clinph.2006.12.005
Preston D, Shapiro B. Electromyography and neuromuscular disorders: clinical-electrophysiologic- ultrasonographic correlations. Pennsylvania: Elsevier 4rd edition; 2021. https://www.elsevier.com/books/electromyography-and-neuromuscular-disorders/978-0-323-66180-5
Jablecki CK, Andary MT, So YT, Wilkins DE, Willians FH (1993) Literature review of the usefulness of nerve conduction studies and electromyography for the evaluation of patients with carpal tunnel syndrome. Muscle Nerve 16:1392–1414
Keith MW, Masear V, Chung K et al (2009) Diagnosis of carpal tunnel syndrome. J Am Acad Orthop Surg 17(6):389–396. https://doi.org/10.5435/00124635-200906000-00007
Jackson D, Clifford JC (1989) Electrodiagnosis of mild carpal tunnel syndrome. Arch Phys Med Rehabil 70:199–204
Bland JD (2000) A neurophysiological grading scale for carpal tunnel syndrome. Muscle Nerve 23:1280–1283
Johnson EW, Melvin JL (1967) Sensory conduction studies of median and ulnar nerves. Arch Phys Med Rehabil 48:25–30
Di Benedetto M, Mitz M, Klingbeil GE, Davidoff D (1986) New criteria for sensory nerve conduction especially useful in diagnosing carpal tunnel syndrome. Arch Phys Med Rehabil 67:586–589
Johnson EW, Sipski M, Lammertse T (1987) Median and radial sensory latencies to digit I: normal values and usefulness in carpal tunnel syndrome. Arch Phys Med Rehabil 68:140–141
Kouyoumdjian JA, Morita MD (1999) Comparison of nerve conduction techniques in 95 mild carpal tunnel syndrome hands. Arquivos de Neuro-Psiquiatria 57(2A):195–197
Andary MT, Fankhauser MJ, Ritson JL et al (1996) Comparison of sensory mid-palm studies to other techniques in carpal tunnel syndrome. Electromyogr Clin Neurophysiol 36:279–285
Cioni R, Passero S, Paradiso C, Giannini F, Battistini N, Rushworth G (1989) Diagnostic specificity of sensory and motor nerve conduction variables in early detection of carpal tunnel syndrome. J Neurol 236:208–213
Pease WS, Cannell CD, Johnson EW (1989) Median to radial latency difference test in mild carpal tunnel syndrome. Muscle Nerve 12:905–909
Carrol G (1987) Comparison of the median and radial sensory latencies in the electrophysiological diagnosis of carpal tunnel syndrome. Electroencephalogr Clin Neurophysiol 68:101–106
White JC, Hansen SR, Johnson RK (1988) A comparison of EMG procedures in the carpal tunnel syndrome with clinical-EMG correlations. Muscle Nerve 11:1177–1182
Mills KR (1985) Orthodromic sensory action potentials from palmar stimulation in the diagnosis of carpal tunnel syndrome. J Neurol Neurosurg Psychiatry 48:250–255
Charles N, Vial C, Chauplannaz G, Bady B (1990) Clinical validation of antidromic stimulation of the ring finger in early electrodiagnosis of mild carpal tunnel syndrome. Electroencephalogr Clin Neurophysiol 76:142–147
Monga TN, Laidlow DM (1982) Carpal tunnel syndrome measurement of sensory potentials using ring and index fingers. Am J Phys Med 61:123–129
Lauritzen M, Liguori R, Trojaborg W (1991) Orthodromic sensory conduction along the ring finger in normal subjects and in patients with a carpal tunnel syndrome. Electroencephalogr Clin Neurophysiol 81:18–23
Uncini A, Lange DJ, Solomon M, Soliven B, Meer J, Lovelace RE (1989) Ring finger testing in carpal tunnel syndrome: a comparative study of diagnostic utility. Muscle Nerve 12:735–741
Yılmaz F, Gündüz OH, Akyüz G (2017) Lumbrical-interosseous recording technique versus routine electrodiagnostic methods in the diagnosis of carpal tunnel syndrome. Turk J Phys Med Rehab 63(3):230–238. https://doi.org/10.5606/tftrd.2017.311
Boonyapisit K, Katirji B, Shapiro BE, Preston DC (2002) Lumbrical and interossei recording in severe carpal tunnel syndrome. Muscle Nerve 25:102–105
Kodama M, Tochikura M, Sasao Y, Kasahara T, Koyama Y, Aono K et al (2014) What is the most sensitive test for diagnosing carpal tunnel syndrome? Tokai J Exp Clin Med 39:172–177
Preston DC, Logigian EL (1992) Lumbrical and interossei recording in carpal tunnel syndrome. Muscle Nerve 15:1253–1257
Ozben S, Acar H, Gunaydin S, Genc F, Ozer F, Ozben H (2012) The second lumbrical-interosseous latency comparison in carpal tunnel syndrome. J Clin Neurophysiol 29:263–267
Rempel D, Evanoff B, Amadio PC, de Krom M, Franklin G, Franzblau A et al (1998) Consensus criteria for the classification of carpal tunnel syndrome in epidemiologic studies. Am J Publ health 88:1447–1451
Saba EK (2015) Median versus ulnar medial thenar motor recording in diagnosis of carpal tunnel syndrome. The Egyptian Rheumatologist 37:139–146. https://doi.org/10.1016/j.ejr.2014.11.001
Acknowledgements
Not applicable
Funding
The study had no funding from any resource.
Author information
Authors and Affiliations
Contributions
The main author designed the methodology, selection of patients, clinical examination, electrophysiological studies, interpretation and analysis of data, manuscript writing, and editing. The single author has read and approved the manuscript
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval for the study was obtained from the ethics committee of the General Organization for Teaching Hospitals and Institutes (GOTHI), with reference number HM000116 at the date 13 December 2019. All patients in this study gave written informed consent to participate in this research. A written informed consent was obtained from all participants to contribute in this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El-Hady, A.O. The sensitivity of median versus ulnar palmar mixed nerve study in the early diagnosis of carpal tunnel syndrome. Egypt Rheumatol Rehabil 50, 9 (2023). https://doi.org/10.1186/s43166-022-00163-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43166-022-00163-9