
Abstract
Background
To assess satisfaction level of patients undergoing septorhinoplasty pre- and post-operatively using Rhinoplasty Outcome Evaluation (ROE) questionnaire.
Methods
The present prospective study, after approval by Institutional Ethics Committee, was conducted in the Department of ENT, SMGS Hospital, from March 2021 to November 2022 on 83 patients who underwent septorhinoplasty. Demographic and clinical characteristics (age, gender, education, technique of surgery) of all participants were recorded. All patients were asked to answer the Rhinoplasty Outcome Evaluation (ROE) questionnaire 1 day prior to surgery. Postoperative ROE questionnaire was asked at the 6th month in ENT OPD by the same researcher.
Results
In our study, the mean preoperative total ROE score was 32.17 ± 5.38, and the mean postoperative total ROE score was 87.11 ± 5.39, the difference being statistically significant (p = 0.0039). Higher post-operative satisfaction score (89.7 ± 5.64) was seen in patients aged more than 35 years, as compared to younger patients (78.4 ± 5.8). In our study, upon gender-wise comparison, there was more statistically significant satisfaction in male patients than female patients postoperatively (p = 0.0022). Better postoperative ROE score was seen in lower literacy group (88.9 ± 6.73) than higher literacy group (83.3 ± 5.63). However, both open and closed techniques showed statistically insignificant difference in postoperative ROE score (p = 0.388).
Conclusion
Based on the Rhinoplasty Outcome Evaluation (ROE) questionnaire, our study showed that septorhinoplasty significantly improved quality of life in majority of our study subjects in terms of both aesthetic as well as functional parameters.
Similar content being viewed by others

Background
Quality of life can be defined as the perception of one’s situation in life within the cultural and value system in which he lives, and in relation to one’s objectives, expectations, standards, and concerns. Thus, it is a concept of a holistic image of wholeness, which can be attained by various aesthetic interventions [1].
As cosmetic surgeries like septorhinoplasty are usually elective and patient satisfaction is of utmost importance, therefore, evaluation based on qualitative parameters is being increasingly recognised [2].
Questionnaires which assess quality of life and self-image have become gold standard for septorhinoplasty as it not only standardises the evaluation of surgical outcomes but also guides regarding comparison of various surgical techniques and identifying patients who may not benefit from surgery [3].
The nose has central location in the face, and any defect in its shape affects personality development and body image; as such, septorhinoplasty is one of the most performed plastic surgeries according to the American Society of Plastic Surgeons, being done most commonly in young males and females [4].
The primary aim of septorhinoplasty is to improve patient’s appearance; hence, patient selection is very important as difficulty in interpreting patient’s expectations could lead to a lower post-operative satisfaction.
Although surgical outcome of septorhinoplasty can be accurately evaluated by anthropometric measurements and anatomical markers of facial measurements, one of the most important determinants, i.e., patient satisfaction and expectation is not included in them. Measuring patient satisfaction and expectation is not an easy task as there are no real standards available [5, 6].
The Rhinoplasty Outcome Evaluation (ROE) questionnaire is a quick, easy to perform, and a validated tool developed by Alsarraf R et al. (2000) [7], which can objectively analyse various qualitative variables involved in septorhinoplasty, such as psychological, social, and emotional aspects.
As the expectation and opinion regarding surgical outcome might differ between surgeon and patient, especially in a procedure like septorhinoplasty which impacts directly on patient satisfaction with own image and eventually self-esteem, we in this study aim to assess satisfaction level of patients undergoing septorhinoplasty pre- and post-operatively using the Rhinoplasty Outcome Evaluation (ROE) questionnaire.
Methods
The present prospective study, after approval by the Institutional Ethics Committee, was conducted in the Department of ENT, SMGS Hospital, from March 2021 to November 2022 on 83 patients who underwent septorhinoplasty. Written informed consent was taken from all subjects.
Inclusion criteria:
-
- Age > 18 years and < 60 years
-
- Giving consent to participate in study
Exclusion criteria:
-
- Patients with congenital nasal deformities
-
- Those requiring revision rhinoplasty
-
- Those requiring concurrent functional endoscopic sinus surgery or other nasal airway procedures
-
- Age less than 18 years or more than 60 years
Demographic and clinical characteristics (age, gender, education, technique of surgery) of all participants were recorded. All patients planned for septorhinoplasty procedure underwent detailed general physical/systemic/local ENT examination. All routine investigations including blood/radiological tests, required for general anaesthesia, were done.
All patients were asked to answer the Rhinoplasty Outcome Evaluation (ROE) questionnaire 1 day prior to surgery. ROE consists of 6 questions (Table 1)—5 questions regarding aesthetic aspects of surgery and one question regarding functional outcome of surgery. Each question was answered on a scale of 0 to 4, with 0 indicating the most negative response and 4 indicating most positive response. The patient’s response to each question were summed up, divided by 24 and multiplied by 100, to get a ROE score varying between 0 and 100, with 0 representing minimum satisfaction and 100 implying most satisfaction.
Patients were followed up postoperatively at the 1st month, 3rd month, and 6th month. Postoperative ROE questionnaire was asked at the 6th month in ENT OPD by the same researcher.
All study data was entered in a Microsoft Excel Spread Sheet and analysed/compared using the Statistical Package for Social Sciences (SPSS) software (version 21 for windows). Appropriate statistical tests were used as advised by statistician (p value < 0.05 was accepted as the statistical significance limit).
Results
A total of 83 patients who underwent septorhinoplasty were included in our study. The mean age of presentation in our study was 32.13 ± 6.82 years. The age wise distribution is shown in Table 2.
Out of 83 patients, 44 were females (53.01%), and 39 (46.99%) were males. The mean age in males was 30.61 ± 3.99 years, and in females, it was 28.87 ± 4.15 years. The indication for surgery was aesthetic in 10 patients (12.04%), functional in 22 patients (26.5%), and combined (aesthetic + functional) in 51 patients (61.4%).
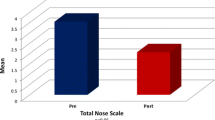
The mean preoperative total ROE score (Table 3) was 32.17 ± 5.38, and mean postoperative total ROE score was 87.11 ± 5.39, the difference being statistically significant (p = 0.0039). The mean preoperative ROE score for age groups less than 35 years (Table 4) was 33.1 ± 4.38, and it was 39.7 ± 5.11 in the age group more than or equal to 35 years (difference being statistically significant p = 0.047). Postoperatively, the mean ROE score for the age group less than 35 years was 78.4 ± 5.89, and it was 89.7 ± 5.64 for the age group more than or equal to 35 years, the difference being statistically significant (p = 0.0019).
Upon gender-wise comparison (Table 5), the mean preoperative ROE score for males was 29.1 ± 4.55, and it was 31.8 ± 5.31 for females, the difference being statistically insignificant (p = 0.261). Postoperatively, the mean ROE score was 92.4 ± 7.37 in males and 83.3 ± 6.92 for females, the difference being statistically significant (p = 0.0022).
Out of 83 patients, 56 patients (67.5%) underwent open technique, and 27 patients (32.5%) underwent closed technique of septorhinoplasty. Upon surgical technique-wise comparison (Table 6), the mean preoperative ROE score for open technique was 31.1 ± 5.75, and it was 30.4 ± 5.11 for closed technique, the difference being statistically insignificant (p = 0.973). Postoperatively, the mean ROE score was 88.2 ± 5.44 in open technique, and it was 86.7 ± 6.05 for closed technique, the difference being statistically insignificant (p = 0.388).
We in our study defined patients who were educated below 8th grade as the low literacy group and those who had college degree and/or above as the high literacy group. Out of 83 patients, 22 patients (26.5%) were in the low literacy group, and 18 patients (21.7%) were in the high literacy group, the rest of the patients being educated above 8th grade but less than college graduation. Upon literacy-wise comparison, the mean preoperative ROE score for the low literacy group was 33.5 ± 5.14, and it was 34.1 ± 5.45 for the high literacy group, the difference being statistically insignificant (p = 0.892). Postoperatively, the mean ROE score was 88.9 ± 6.73 for the low literacy group, and it was 83.3 ± 5.63 for the high literacy group, the difference being statistically significant (p = 0.034).
Discussion
Rhinoplasty is a complex procedure, and the operating surgeon must not only be well-versed with the underlying anatomy but also have the capability to perform a nasofacial analysis to formulate the operative plan and perform techniques that manipulate the bone, cartilage, and soft tissue [8].
Patient satisfaction is the most important indicator of success in cosmetic surgeries like septorhinoplasty, thus making the use of quantitative tools to assess the surgical outcome very crucial.
The Rhinoplasty Outcome Evaluation (ROE) questionnaire considers various factors which influence patient satisfaction, such as physical factors like nasal shape, emotional factors like degree of confidence, desire to change appearance, and social factors like family/social acceptance [9].
In our study, the mean preoperative total ROE score (Table 3) was 32.17 ± 5.38, and the mean postoperative total ROE score was 87.11 ± 5.39, the difference being statistically significant (p < 0.05). Thus, there was an improvement in ROE score by about 54.9 points, implying a high index of satisfaction in our patients. This is comparable to studies conducted by Arima et al. [10] and Cingi C and Eskiizmir G [11], who reported improvements in ROE score by 50.5 and 56.3 points respectively. However, studies done by Meninguad et al. (2008) [12] and Bulut OC et al. (2015) [13] showed improvements by 30.4 and 21.7 points only, respectively.
Out of 83 patients, 41 patients were below or equal to the age of 35 years, and 42 patients were above the age of 35 years. Between these two age groups (Table 4), there was statistically more significant satisfaction (p < 0.05) with surgical outcome in patients above 35 years than those patients who were less than or equal to 35 years. This finding was comparable to studies conducted by Litner JA et al. (2008) [14] and Gunel C et al. (2015 [15]. The reason for this difference could be due to the fact that as a person ages, person gets more accepting of how they look and adapt well to their new facial appearance, while younger patients have greater expectations due to greater need for social acceptance and being more negatively affected by the unrealistic demands to hide their facial imperfections before social media. Hence, we need to counsel and guide younger patients in a more detailed manner so as to get better postoperative surgical satisfaction.
In our study, upon gender-wise comparison (Table 5), there was more statistically significant satisfaction in male patients than female patients (p < 0.05). This finding was consistent with studies conducted by Bilgin E et al. (2020) [16]. However, Khansa I et al. (2015) [17] reported more satisfaction in females, while Sozen et al. (2017) [18] showed in their study that there was no difference between males and female patients in terms of surgical outcome satisfaction. The reason for this finding could be due to females being more concerned regarding their facial appearance, as compared to male patients.
In our study, there was no statistically significant difference (Table 6) in postoperative patient satisfaction on the basis of surgical technique used (p = 0.388). This was consistent with study conducted by Esteves SS et al. (2016) [2]. However, there was statistically more significant satisfaction (Table 7) in the lower literacy group of patients than the higher literacy group (p < 0.05). This finding was comparable to study conducted by Khan N et al. (2019) [19]. The reason for this finding could be due to the fact that patients with lower literacy had lower expectations regarding the extent their facial appearance should change after surgery, while higher literacy patients have less satisfaction as they keep on trying to gather more and more knowledge regarding how outcome of surgery should have been.
Conclusion
Based on the Rhinoplasty Outcome Evaluation (ROE) questionnaire, our study showed that septorhinoplasty significantly improved quality of life in the majority of our study subjects in terms of both aesthetic as well as functional parameters. Various factors like older age group, lower literacy, and male gender are more likely to have better satisfaction with postoperative surgical outcome, while the type of surgical technique used has no impact on patient’s quality of life. There are many other uncontrolled factors like demographic criteria/education of relatives and friends, which need to be studied as well; thus, further studies are required to find the effect of such factors on score values.
Availability of data and materials
Available with corresponding author upon reasonable request.
References
The Whoqol Group (1998) The World Health organization Quality of Life Assessment (WHO-QOL): development and general psychometric properties. Soc Sci Med 46(12):1569–82
Esteves SS, Ferreira MG, Almeida JC, et al. (2016) Evaluation of aesthetic and functional outcomes in rhinoplasty surgery: a prospective study. Braz J Otorhinolaryngol 83(5):552–7. https://doi.org/10.1016/j.bjorl.2016.06.010
Ching S, Thoma A, McCabe RE et al (2003) Measuring outcomes in aesthetic surgery: a comprehensive review of the literature. Plast Reconstr Surg 111:469–480
Picavet VA, Prokopakis EP, Gabriels L et al (2011) High prevalence of body dysmorphic disorder symptoms in patients seeking rhinoplasty. Plast Reconstr Surg 128:509–517
Okur E, Yildirim I, Ayodgan B et al (2004) Outcome of surgery for crooked nose: an objective method of evaluation. Aesthetic Plast Surg 28:203–207
Nouraei SA, Pulido MA, Saleh HA (2009) Impact of rhinoplasty on objective measurement and psychophysical appreciation of facial symmetry. Arch Facial Plast Surg 11:198–202
Alsarraf R (2000) Outcomes research in facial plastic surgery: a review and new directions. Aesthetic Plast Surg 24(3):192–197
Rohrich RJ, Ahmad J (2011) Rhinoplasty. Plast Reconstr Surg 128:49–73
Izu SC, Kosugi EM, Brandao KV et al (2012) Normal values for the Rhinoplasty Outcome Evaluation (ROE) questionnaire. Braz J Otorhinolaryngol 78(4):76–79
Arima LM, Velasco LC, Tiago RS (2012) Influence of age on rhinoplasty outcomes evaluation: a preliminary study. Aesth Plast Surg 36:248–253
Cingi C, Eskiizmir G (2013) Deviated nose attenuates the degree of patient satisfaction and quality of life in rhinoplasty: a prospective controlled study. Clin Otolaryngol 38:136–141
Meningaud JP, Lantieri L, Bertrand JC (2008) Rhinoplasty: an outcome research. Plast Reconstr Surg 121:251–257
Bulut OC, Wallner F, Plinkert PK et al (2015) Quality of life after septorhinoplasty measured with the Functional Rhinoplasty Outcome Inventory 17. Rhinology 53:54–58
Litner JA, Rotenberg BW, Dennis M et al (2008) Impact of cosmetic facial surgery on satisfaction with appearance and quality of life. Arch Facial Plast surg 10:79–83
Gubel C, Omurlu IK (2015) The effect of rhinoplasty on psychosocial distress level and quality of life. Eur Arch Oto Rhino Laryngol 272:1931–5
Bilgin E, Say M, Baklaci D (2020) Assessment of patient satisfaction with primary septorhinoplasty using the rhinoplasty Outcome Evaluation Questionnaire. Cureus 12(11):e11777
Khansa I, Khansa L, Pearson GD (2015) Patient satisfaction after rhinoplasty: a social media analysis. Aesth Surg J 10:1–5
Sozen T, Cabbarzade C, Tahir E et al (2017) Factors determining patient satisfaction in rhinoplasty: analysis of 506 cases with rhinoplasty outcome evaluation. Acta Medica 48:1–5
Khan N, Rashid M, Khan I et al (2017) Satisfaction in patients after rhinoplasty using the Rhinoplasty Outcome Evaluation Questionnaire. Cureus 11(7):e5283
Acknowledgements
None.
Funding
Nil.
Author information
Authors and Affiliations
Contributions
AS made contributions in the data collection and design of manuscript. NG made contributions in the interpretation of data. MM and PK made contributions in the data analysis. All authors read and gave approval to the final version of submitted manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted after approval by Institutional Ethics Committee of GMC Jammu. Written informed consent was taken from all subjects or their legal guardian in case of age of patient being less than 18 years. No animals were used in the study.
Consent for publication
Written informed consent to publish patient’s clinical details was obtained from all subjects or their legal guardian in case of subject under 18 years.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Saraf, A., Gupta, N., Manhas, M. et al. Evaluation of quality of life after septorhinoplasty using Rhinoplasty Outcome Evaluation questionnaire. Egypt J Otolaryngol 39, 82 (2023). https://doi.org/10.1186/s43163-023-00445-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-023-00445-9