
Abstract
Background
Lingual edema is usually the result of infectious etiology, angioedema, and less commonly of traumatic etiology.
As for the therapeutic approach, the first priority excluding airway compromise or ensuring airway safety. Antibiotic treatment should be administered for tongue swelling of inflammatory etiology while standard therapy with epinephrine, steroids, and antihistamines is recommended for cases of anaphylaxis. In addition, in case of injury causing lingual edema, one of the treatment options is surgical intervention.
Aim of work
The aim of our work is to present a rare and simultaneously instructive case of traumatic hemorrhagic edema of the tongue, leading to airway obstruction.
Case presentation
We report a case of hemorrhagic traumatic lingual edema, initially without symptoms of upper airway obstruction on admission. However, immediate intervention and airway securing was necessary due to rapid growth of the edema.
Then, as long as patient was hemodynamically stable and airway patency was ensured, the diagnosis of iatrogenic tongue hematoma was confirmed. The challenge was to decide the appropriate treatment for the patient. Following, she was taken for 24 h to the ICU due to lactic acidosis while the bleeding was treated conservatively.
Afterward, she was transferred to the clinic, hemodynamically stable, and was discharged uneventfully.
Conclusions
Hemorrhagic edema of the tongue may become a life-threatening condition. Its rapid growth can lead to obstruction of the upper respiratory way; therefore, special wariness in its management is required. Treatment can be conservative or surgical, depending on the size and tendency of hematoma to increase.
Similar content being viewed by others


Background
The tongue is a richly vascular structure, mainly supplied by branches of the lingual artery. Lingual edema is usually the result of infectious etiology, angioedema and less commonly of traumatic etiology or a complication in patients receiving anticoagulant/antiplatelet therapy [1, 2]. Tongue edema is a clinical diagnosis. In order to identify the cause of the swelling of the tongue, a detailed medical history including the medication that the patients receive is necessary.
Laboratory investigations include leukocyte counts and CRP assessment to differentiate for infection as well as specialized laboratory tests, including tryptase, C4, and C1 for excluding angioedema [3]. As for the therapeutic approach, the first priority excluding airway compromise or ensuring airway safety. Antibiotic treatment should be administered for tongue swelling of inflammatory etiology while standard therapy with epinephrine, steroids and antihistamines is recommended for cases of anaphylaxis [3]. In addition, in case of injury causing lingual hemorrhagic edema, one of the treatment options is surgical intervention [4, 5]. Hemorrhagic edema of the tongue may become a life-threatening condition. Its rapid growth can lead to obstruction of the upper respiratory way; therefore, special wariness in its management is required.
Case presentation
Our case concerns a 60-year-old woman with history of chronic end-stage kidney disease, undergoing regular hemodialysis. In her scheduled appointment for hemodialysis, the placement of a central venous catheter in the right internal jugular vein was deemed necessary. This attempt was unsuccessful causing injury to the neck and resulted in hemorrhagic swelling of the tongue. The patient was referred to the emergency department for treatment.
Her medical history included diabetes mellitus and hypertension. She was treated with acetylsalicylic acid daily and bemiparin injections on non-hemodialysis days.
Clinical findings
On physical examination, a massive dark-red colored swelling of the tongue was noticed in the anterior two thirds of the tongue extending in the floor of the mouth. The tongue was enlarged in such extend that was protruding out of her mouth (Figs. 1 and 2).

Massive swelling of the tongue with dark red coloration on admission

Lingual hematoma extending in the floor of the mouth
At the same time, ecchymosis and edema coexisted in the corresponding lateral cervical region, after the attempt to place a central venous catheter in the right internal jugular vein (Fig. 3). Upon arrival, the patient was hemodynamically stable with no symptoms of upper airway obstruction.

Ecchymosis in the right lateral cervical region
Investigations
The diagnostic approach on admission included laboratory examination, who revealed a hemoglobin of 9.3 g/100 ml with a hematocrit of 29.2% and WBC 11.1/cu mm. Platelet count was 159,000/cu mm and INR was 2.72.
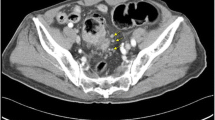
Additionally, a computed tomography angiography of the head and neck showed diffuse enlargement of the tongue, active contrast extravasation from the right lingual artery, and enlargement of the right sternocleidomastoid muscle (Fig. 4).

CT angiography: diffuse enlargement of the tongue, active contrast extravasation from the right lingual artery and enlargement of the right sternocleidomastoid muscle
Treatment
Οn presentation to the emergency department, the patient received a dose of methylprednisolone 250 mg intravenous.
A few hours after her admission, the patient showed signs of progressive airway obstruction; therefore, the airway saw secured by performing a surgical tracheostomy under general anesthesia with nasotracheal intubation.
Subsequently, the patient was treated for 24 h to the ICU due to lactic acidosis, while hemorrhagic edema of the tongue was treated conservatively. The conservative treatment included methylprednisolone (40 mg daily, intravenous antibiotics (sultamicillin tosylate and clindamycin phosphate) and hemodialysis sessions to regulate the coagulation mechanism.
Following, she was transferred to the Nephrology Clinic, hemodynamically stable. Feeding was performed by a nasogastric tube.
Outcome and follow-up
The patient showed daily improvement of the tongue swelling and airway patency, so on the 8th postoperative day the tracheostomy was safe to remove.
Follow-up showed complete resolution of the lingual hematoma with normal tongue mobility (Fig. 5). Blood tests were normal at discharge and INR was 1.01.

Follow-up after 1 month: complete resolution of the lingual hematoma and traumatic ulcer
Discussion
Traumatic swelling of the tongue is a rare but life-threating complication, and it is imperative to secure the upper airway.
Renehan and Morton suggested a classification of acute enlargement of the tongue based on the various etiologies. This classification system includes 4 categories: bleeding of traumatic etiology, vascular abnormality or disorder of coagulation, oedema, infarction, and infection [2].
Our case concerns a traumatic lingual hematoma, in addition to the contributing factor of receiving anticoagulants. The recognition of the etiological causes is fundamental for the choice of the right treatment and consequently a good outcome. An important parameter is timely intervention because lingual hematomas often comprise a rapidly deteriorating situation.
Airway management is of major importance in cases of acute, massive lingual enlargement.
Symptoms such as dyspnea, dysphonia, and stridor, combined with progressive swelling of the tongue and sublingual gland should alert the physician of pending upper airway obstruction. In such case, the airway should be secured with surgical tracheostomy, if possible by oral, or nasotracheal intubation [6, 7].
Chase et al. encountered an airway obstruction due to swelling of a lacerated tongue treated by an emergency tracheostomy under local anesthesia and subsequence suture of the lacerated tongue [7].
Reija et al. managed a lingual hematoma secondary to traumatic tongue biting after tonic-clonic seizures and thrombocytopenia conservatively. After establishing a secure airway by orotracheal intubation, they figured out that there was no active hemorrhage and no further therapeutic interventions were needed [8]. In such cases, treatment is usually conservative with monitoring of the patient and correction of coagulation factors [8, 9].
Furthermore, in a similar case with lingual hematoma after tonic-clonic seizures, Lo et. Al had to intubate nasotracheally the patient and the swelling resolved with steroids conservatively [9].
Less often active bleeding coexisting with hematoma and tongue edema may be surgically controlled by ligation of the feeding vessel, or by endovascular embolism. This approach depends on the size and the tendency of hematoma to increase over time.
Dhaliwal et al. were requested to treat a patient with active bleeding due to deep lacerations and tongue hematoma. After failing to identify the source of the extravasation, they proceeded to wound exploration, hematoma evacuation, and extraoral ligation of the lingual artery [6].
Tongue hematoma excision and draining is not usually suggested because bleeding takes place into the lingual muscles rather than into the fascial spaces.
Interestingly, Carden et al. reports the effectiveness of leeches at reducing the size of a tongue hematoma [10].
Conclusions
Hemorrhagic edema of the tongue may become a life-threatening condition. Its rapid growth can lead to obstruction of the upper respiratory way, therefore special wariness in its management is required. This includes primarily securing the airway, identifying the cause, and establishing hemostasis.
Treatment can be conservative or surgical, depending on the size and tendency of hematoma to increase.
Learning points
-
Traumatic tongue hematoma is a rare, but life-threatening condition and should be recognized promptly.
-
Even simple medical procedures need attention, to avoid life-threatening complications for the patient.
-
Airway management is of major importance in cases of acute, massive lingual enlargement and if required a surgical tracheostomy must be done.
-
Treatment can be conservative or surgical, depending on the size and tendency of hematoma to increase.
Availability of data and materials
Not applicable.
References
Dass C, Mahaffa M, Dang E, Campbell R, Ballas Z, Lee S (2021) Evaluation of staging criteria for disposition and airway intervention in emergency department angioedema patients. Acute Med Surg. 8(1):e704. https://doi.org/10.1002/ams2.704 PMID: 34729186; PMCID: PMC8548721
Renehan A, Morton M (1993) Acute enlargement of the tongue. Bri J Oral Maxillofacial Surg 31(5):321–324. https://doi.org/10.1016/0266-4356(93)90071-4
Long BJ, Koyfman A, Gottlieb M (2019) Evaluation and management of angioedema in the emergency department. West J Emerg Med 20(4):587–600. https://doi.org/10.5811/westjem.2019.5.42650 Epub 2019 Jul 2. PMID: 31316698; PMCID: PMC6625683
Kaynar AM, Bhavani-Shankar K, Mushlin P (1999) Lingual hematoma as a potential of upper airway obstruction. Anesth Analg 89:1573
Song Z, Laggan B, Parulis A (2008) Lingual hematoma treatment rationales: a case report. J Oral Maxillofac Surg. 66(3):535–539. https://doi.org/10.1016/j.joms.2006.09.023 PMID: 18280389
Dhaliwal HS, Dhaliwal SS, Heckel RD, Quereshy FA, Baur DA (2011) Diagnosis and management of upper airway obstruction due to lingual hematoma: report of a case. J Oral Maxillofac Surg. 69(2):558–563. https://doi.org/10.1016/j.joms.2009.11.007 Epub 2010 Feb 13. PMID: 20156666
Chase CR, Hebert JC, Farnham JE (1987) Post-traumatic upper airway obstruction secondary to a lingual artery hematoma. J Trauma. 27(8):953–954. https://doi.org/10.1097/00005373-198708000-00018 PMID: 3612876
Reija MG, Fernández-Barriales M, Terán TG, Santolino SS (2019) Traumatic lingual haematoma: Another unusual cause of upper airway obstruction in systemic lupus erythematosus. Trauma Case Rep. (23):100226. https://doi.org/10.1016/j.tcr.2019.100226 PMID: 31372486; PMCID: PMC6660455
Lo BM, Campbell BH (2010) A traumatic swollen tongue. Resuscitation. 81(3):267. https://doi.org/10.1016/j.resuscitation.2009.12.013 Epub 2010 Jan 13. PMID: 20071066
BET (2013) 2: leeches (hirudotherapy) or steroids for traumatic obstructive tongue swelling? Emerg Med J. 30(12):1062–1063. https://doi.org/10.1136/emermed-2013-203256.2 PMID: 24232008
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
Supervised by HJ. Patient was under the care of HJ and FS. Report was written by KV and HJ. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent to publish this information was obtained from the study participant.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kyriaki, V., Fani, S. & Jiannis, H. Iatrogenic massive hemorrhagic edema of the tongue: a case report. Egypt J Otolaryngol 38, 128 (2022). https://doi.org/10.1186/s43163-022-00317-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-022-00317-8