
Abstract
Background
Elective neck dissection with salvage laryngectomy was associated with decreased quality of life, increased operative time, and increased incidence of complications; some surgeons prefer wait-and-see observation policy. However, lymph nodes recurrence after salvage total laryngectomy during follow-up period carry very poor quality of life and very poor survival rate.
The aim of this study is to investigate the risk of nodal metastases in patients undergoing salvage laryngectomy and to search for predictors of occult metastases in this group of patients. Our study included 30 patients presented with recurrent laryngeal cancer after failure of organ preservation protocol. All selected patients were without detected lymph nodes both clinically and radiologically, classified as N0 according to The TNM classification.
All patients were candidate for salvage total laryngectomy and had elective neck dissection performed during surgery to detect the possible occult cervical lymph node metastasis.
Results
The positive nodal metastasis incidence was 14% in glottic, 29% in supraglottic, and 57% in trans-glottic tumors of all positive patients. The previously indicated results showed statistically significantly increased incidence of positive LN in the supraglottic tumor site and increased incidence of negative LN in the glottic site.
Regarding the recurrence T stage in our study, lymph nodes were negative for metastasis in one patient with rT1 representing 4%, 6 patients with rT2 representing 26%, and for rT3 and rT4 were 65% and 4%, respectively. The nodal metastasis was positive in 3 patients with rT3 representing 43% and 4 patients with rT4 representing 57%. No patients with rT1 or rT2 showed nodal metastasis.
Conclusions
Our findings demonstrated that patients with advanced local disease at recurrence undergoing salvage total laryngectomy may benefit from an elective neck dissection.
Similar content being viewed by others


Background
Treatment strategies of laryngeal cancer has changed dramatically, due to the development of organ preservation protocols; as a result, total laryngectomy is commonly reserved as salvage treatment for recurrent tumors [1].
Incidence of occult nodal metastases in primary nonirradiated laryngeal cancer cases is high; in these cases, elective neck dissection is mandatory; however, incidence decreases after failure of primary radiation therapy making the role of elective neck dissection controversial [1].
Lymphatic tissues change after irradiations includes decrease caliber of lymphatic vessels and hyalinized and fibrosed lymph nodes which serve as a barrier for lymphatic dissemination of locally recurrent tumors after previous irradiation [2].
As elective neck dissection with salvage laryngectomy was associated with decreased quality of life, increased operative time, and increased incidence of complications, some surgeons prefer wait-and-see observation policy [2].
However, lymph nodes recurrence after salvage total laryngectomy during follow-up period carry very poor quality of life and very poor survival rate [3].
The aim of this study is to investigate the risk of nodal metastases in patients undergoing salvage laryngectomy and to search for predictors of occult metastases in this group of patients, thus trying to verify the need of elective neck dissection in salvage laryngectomy inspite of the higher rate of complications that may occur.
Methods
Our study included 30 patients attending otolaryngology outpatient clinic, presented with recurrent laryngeal cancer after failure of organ preservation protocol during the period from October 2014 to February 2017.
All selected patients were without detected lymph nodes both clinically and radiologically, classified as N0 according to the TNM classification.
All patients were candidate for salvage total laryngectomy and had elective neck dissection performed during surgery to detect the possible occult cervical lymph node metastasis. The study is approved by ethical committee of our institution.
All patients were subjected to the following preoperative protocol:
-
Full history taking including history of previous treatment regimen for laryngeal carcinoma
-
Full otorhinolaryngological examination was done for each patient that is included.
-
In full head and neck examination, endoscopic assessment through flexible laryngoscopy or rigid endoscopy was done.
CT neck was done for each patient including axial and coronal cuts with sagittal reconstruction for assessment of the lesion, the neck nodes, and for confirmation of the radiologically N0 nodal stage.
Direct laryngoscopy under general anesthesia and biopsy was done to prove the presence of recurrent carcinoma. Biopsy sites included the obvious lesion of interest and any suspicious lesions for assessment of the site, the extent of the tumor, and proper TNM classification and compare it with the previous initial histopathology and TNM classification workout to exclude distant metastasis.
All patients were diagnosed with recurrent cancer larynx after failure of radiotherapy or chemoradiotherapy and were listed for salvage laryngectomy.
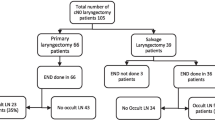
The surgeries performed included 30 salvage total laryngectomies. All patients were N0 with no detected metastatic cervical lymph nodes clinically and radiologically; elective lateral neck dissections (level II, III, IV) were performed unilaterally in 23 patients and bilaterally in 7 patients.
Unilateral elective lateral neck dissections were performed in unilateral tumors, while bilateral elective lateral neck dissections were done for midline tumors, those crossing the midline and supraglottic tumors.
A total of 37 elective neck dissections were performed with salvage total laryngectomy for the 30 patients. After surgery, each lymph node level was dissected separately and was sent for histopathological examination. Data were analyzed by the Statistical Package for Social Science (IBM SPSS) version 20.
The comparison between two groups was done by using chi-square test, and/or Fisher exact test was used instead of chi-square test when the expected count in any cell was found less than 5.
The p-value was considered significant as the following:
-
P > 0.05: nonsignificant
-
P < 0.05: significant
-
P < 0.01: highly significant
Results
Our study included 30 patients (27 males and 3 females). The age ranged from 42 to 82 with a mean age of 60.4. Regarding the histopathological type, it was squamous cell carcinoma in all patients.
The initial tumor subsite was glottic in 10 (33%) of patients, supraglottic in 2 (7%), and transglottic in 17 (57%), while in one (3%) patient, the tumor was subglottic.
Regarding the initial TNM staging, the tumor was T2 in 8 patients representing 27%, T3 in 18 patients representing 60%, and T4 in 4 patients representing 13% of all. No patient was T1 in initial staging. Meanwhile, all of them were initially N0.
All patients were initially treated with radiotherapy as the primary treatment modality, and 25 of them received full course representing 83%. Chemotherapy was given to 22 patients representing 73%.
Regarding recurrence, the TNM staging was rT1 in one patient (3%), rT2 in 6 patients representing 20%, r T3 in 18 patients (60%), and rT4 in 5 patients (17%). All patients were N0. Elective neck dissections were performed in all patients with salvage total laryngectomy, of which 23 were unilateral and 7 were bilateral.
Regarding operative complications, our results indicated that no complications were recorded in 19 patients (63.3%), delayed wound healing occurred in 2 patients (6.7%), pharyngocautaneous fistula occurred in 7 patients representing 23%, chylous fistula occurred in one patient representing 3%, and postoperative bleeding occurred in one patient.
Regarding lymph nodes analysis in the operative specimen, lymph nodes metastasis was negative in 23 patients representing 77% and positive in 7 patients representing 23% of our patients.
On routine histopathological examination with H&E staining, 23 of lymph nodes were negative for metastasis representing 77% of all with single node metastasis in three patients, 2 lymph nodes metastasis in two patients, while 3 lymph nodes metastasis was detected in one patient and 4 lymph nodes metastasis in one patient.
Regarding negative lymph nodes analysis according to the initial tumor sites, lymph nodes were negative in 9 patients with glottic tumors representing 39%, 13 patients with trans-glottic tumor representing 57%, and one patient with subglottic tumor representing 4% of all negative patients.
Regarding the positive nodal metastasis incidence, it was 14% in glottic, 29% in supraglottic, and 57% in transglottic tumors in all positive patients.
This showed statistically significant increased incidence of positive LN in the supraglottic tumor site and increased incidence of negative LN in the glottic site (p-value = 0.049).
Regarding the analysis according to the initial T staging, the nodal metastasis was positive in 0% of T1 tumors, 14% of T2 tumors, and 29% and 57% of T3 and T4 tumors, respectively, of all positive patients.
The nodal metastasis was negative in 0% of initial T1 tumors, 30% of initial T2, and 70% and 0% of initial T3 and T4 tumors, respectively, that showed statistical significance increased incidence of positive LN in initial T4 stage (p-value = 0.001).
After full radiotherapy course, LNs were positive in 3 patients representing 42.86% of all positive patients and negative in 22 patients representing 95.65% of all negative patients (Table 1).
After interrupted radiotherapy course, positive LNs were in 4 patients representing 57.14% of all positive patients, and negative LNs were in one patient representing 4.35% of all negative patients. Showing statistical significance increased incidence of positive LN in patients with interrupted course of radiotherapy (p-value = 0.001).
Regarding chemotherapy, in patients treated with chemotherapy, LNs were positive in 3 patients representing 42.86% of all positive patients and negative in 19 patients representing 82.61% of all negative patients.
In patients not treated with chemotherapy, positive LNs metastasis was in 4 patients representing 57.14% of all positive patients, and negative LNs metastasis was in 4 patients representing 17.39% of all negative patients showing statistical significance increased incidence of positive LN in patients not taking chemotherapy (p-value = 0.037).
Regarding lymph nodes analysis according to the recurrent T stage, the nodal metastasis was positive in three patients with rT3 representing 43% and 4 patients with rT4 representing 57%, with no patients with neither rT1 nor rT2 showing nodal metastasis that showed a high statistical significance (p-value=0.009).
Lymph nodes were negative in one patient with rT1 representing 4%, 6 patients with rT2 representing 26%, and for rT3 and rT4 were 65% and 4%, respectively (Table 2).
Regarding laterality of neck dissection, 18 patients with unilateral neck dissection representing 78% found to be negative for LN, while 5 patients representing 71% found to be negative, and for bilateral neck dissection, 5 patients representing 22% found to be negative, and two patients representing 29% found to be positive showing no statistical significance.
Discussion
Laryngeal carcinomas carry a high risk of occult nodal metastasis. Positive nodes are associated with a poor locoregional disease control and poor survival outcome. A single ipsilateral lymph node metastasis decreases survival by about 50% [4].
Revolution in treatment of laryngeal carcinoma started with endoscopic surgery and the development of organ preservation protocols. As a result, total laryngectomy is reserved mainly as salvage treatment for recurrent laryngeal cancer [1].
In salvage surgery for recurrent laryngeal carcinoma, positive cervical lymph nodes should be treated with primary laryngeal tumors; the debate still presents with negative cervical lymph nodes whether to be treated electively or to choose to wait and see observation policy [5].
Neck dissection with salvage total laryngectomy after radiotherapy or chemoradiotherapy carries high rate of complications and morbidities, benefits of elective neck dissection in negative nodes in these patients, and the overall survival results still controversial [6].
In our study, we included 30 patients with undetected lymph nodes both clinically and radiologically classified as N0 according to the TNM classification had elective neck dissection performed during salvage total laryngectomy to detect the possible occult cervical lymph node. The initial tumor subsite was glottic in 10 (33%) of patients, supraglottic in 2 (7%), and transglottic in 17 (57%), while in one (3%) patient, the tumor was subglottic. The tumor was T2 in 8 patients representing 27%, T3 in 18 patients representing 60%, and T4 in 4 patients representing 13% of all. No patient was T1 in initial staging. Meanwhile, all of them were initially N0.
Regarding the initial tumor sites in our study, lymph nodes were negative in 9 patients with glottic tumors representing 39%,13 patients with transglottic tumor representing 57%, and one patient with subglottic tumor representing 4%. No patients with initial supraglottic tumor had negative lymph node metastasis of all negative patients. The positive nodal metastasis incidence was 14% in glottic, 29% in supraglottic, and 57% in transglottic tumors of all positive patients. The previously indicated results showed statistically significantly increased incidence of positive LN in the supraglottic tumor site and increased incidence of negative LN in the glottic site, so we suggest that elective neck dissection can be considered in supraglottic tumors. For other sites, it is difficult to offer a recommendation, but clinical judgment can guide the treatment policy.
Regarding the initial T staging in our study, we found that the nodal metastasis was positive in 0% of T1 tumors, 14% of T2 tumors, and 29% and 57% of T3 and T4 tumors, respectively, and was negative for nodal metastasis in 0% of initial T1 tumors, 30% of initial T2, and 70% and 0% of initial T3 and T4, respectively, tumors of all positive patients that showed statistically significant increased incidence of positive LN in initial T4 stage, and so we suggest that observation policy for the neck could be considered in patients with tumors classified originally as early tumors (T1-2) and elective neck dissection in more advanced tumor (T3-T4).
Regarding the recurrence T stage in our study, lymph nodes were negative for metastasis in one patient with rT1 representing 4%, 6 patients with rT2 representing 26%, and for rT3 and rT4 were 65% and 4%, respectively. The nodal metastasis was positive in 3 patients with rT3 representing 43% and 4 patients with rT4 representing 57%. No patients with rT1 or rT2 showed nodal metastasis, and so we suggest that observation policy for the neck could be considered in less advanced recurrence (rT1-2) and elective neck dissection in more advanced recurrences (rT3-4).
Amit et al. study in 2012 underwent a salvage laryngectomy with elective neck dissection (42 unilateral and 9 bilateral). Originally, 85% of patients were staged N0, 57% were T1-T2, and 62% of patients had glottic tumors. Occult nodal metastases were found in 19% of patients with no contralateral lymph node metastases. The frequency of occult metastases in patients with T1-2 N0 tumors was 14% and 22% in T3-4 or N+ patients. The frequency in glottic tumors was 15, while it was 25% in supraglottic tumors [1].
Yao et al. study in 2005 was not able to find a statistically significant difference in 5-year overall survival between those who underwent neck dissection and those who did not, while survival was higher for patients with supraglottic tumors who underwent neck dissection; however, the difference was nonstatistically significant.
They found that survival was higher for patients with supraglottic tumors who underwent neck dissection; thus, it is possible that elective neck dissection may offer a survival advantage for patients with more advanced recurrent tumors [7].
Hilly et al. study in 2013 suggested that the patients with advanced local disease at recurrence undergoing salvage total laryngectomy may benefit from an elective neck dissection [8].
Sanabria et al. study in 2014 suggests observation policy for the neck could be used for patients with glottic tumors classified originally as early tumors (T1-2) and who recurred with less advanced tumors (rT1-2). For more advanced tumor recurrences (rT3-4), elective neck dissection could be considered with bilateral neck dissections for supraglottic tumors [3].
Dagan et al. (2010) were against elective neck dissection with salvage total laryngectomy and reported that there were no statistically significant differences in overall survival between observation or performing elective neck dissection and recommended an expectant policy for the N0 neck patients to reduce complications [2].
Also, Bohannon et al. (2010) were against elective neck dissection with salvage total laryngectomy and reported that there was no survival advantage gained by performing neck dissection in the clinically negative neck [9].
Regarding operative complications, no complications reported in 19 patients (63.3%), pharyngocautaneous fistula occurred in 7 patients (23%), delayed wound healing occurred in 2 patients (6.7%), chylous fistula occurred in one patient (3%), and postoperative bleeding occurred in one patient (3%).
A study carried by Freiser et al. in 2016 showed that elective neck dissection with salvage total laryngectomy did not carry any significant risk nor increased incidence of complications; Basheeth et al. in 2013 also showed no increased risk of complications with unilateral elective neck dissection with salvage total laryngectomy but showed increased complications in bilateral elective neck dissection [6, 10].
Amit et al. (2012) and Basheeth et al. (2013) did not recommend bilateral neck dissection as an elective procedure, as it increases the risk of complication, and the contralateral nodes carry low incidence of metastasis [1, 6].
So, we recommended that the need for performing elective neck dissection should be balanced against the risk of developing future neck metastases and against the risk of complications of neck dissection especially delayed wound healing and fistula formation particularly after previous radiotherapy.
We suggest observation policy for the neck could be used for patients with glottic tumors classified originally as early tumors (T1-T2) and who recurred with less advanced tumors (rT1-rT2). For more advanced tumors recurrences (rT3-rT4), the suggestion is that elective neck dissection could be considered, with bilateral neck dissections for supraglottic tumor.
Conclusions
Our findings demonstrated that patients with advanced local disease at recurrence undergoing salvage total laryngectomy may benefit from an elective neck dissection; observation policy for the neck could be considered in less advanced recurrence (rT1-2) and elective neck dissection in more advanced recurrences (rT3-4), and that elective neck dissection could be considered in supraglottic tumors.
Availability of data and materials
Data are available from the authors upon reasonable request with permission from Cairo University.
References
Amit M, Hilly O, Leider-Trejo L, Popovtzer A, Gutfeld O, Shvero J, Fliss DM, Cohen JT, Bachar G, Gil Z (2013) The role of elective neck dissection in patients undergoing salvage laryngectomy. Head Neck 35(10):1392–1396. https://doi.org/10.1002/hed.23145 Epub 2012 Sep 28. PMID: 23019150
Dagan R, Morris CG, Kirwan JM, Werning JW, Vaysberg M, Amdur RJ, Mendenhall WM (2010) Elective neck dissection during salvage surgery for locally recurrent head and neck squamous cell carcinoma after radiotherapy with elective nodal irradiation. Laryngoscope. 120(5):945–952. https://doi.org/10.1002/lary.20854 PMID: 20422688
Sanabria A, Silver CE, Olsen KD, Medina JE, Hamoir M, Paleri V, Mondin V, Rinaldo A, Rodrigo JP, Suárez C, Boedeker CC, Hinni ML, Kowalski LP, Teymoortash A, Werner JA, Takes RP, Ferlito A (2014) Is elective neck dissection indicated during salvage surgery for head and neck squamous cell carcinoma? Eur Arch Otorhinolaryngol 271(12):3111–3119. https://doi.org/10.1007/s00405-014-2893-x Epub 2014 Feb 11. PMID: 24515917
Enepekides DJ, Sultanem K, Nguyen C, Shenouda G, Black MJ, Rochon L (1999) Occult cervical metastases: immunoperoxidase analysis of the pathologically negative neck. Otolaryngol Head Neck Surg 120(5):713–717. https://doi.org/10.1053/hn.1999.v120.a91761 PMID: 10229598
Deganello A, Gitti G, Meccariello G, Parrinello G, Mannelli G, Gallo O (2011) Effectiveness and pitfalls of elective neck dissection in N0 laryngeal cancer. Acta Otorhinolaryngol Ital 31(4):216–221 PMID: 22058599; PMCID: PMC3203726
Basheeth N, O'Leary G, Sheahan P (2013) Elective neck dissection for no neck during salvage total laryngectomy: findings, complications, and oncological outcome. JAMA Otolaryngol Head Neck Surg 139(8):790–796. https://doi.org/10.1001/jamaoto.2013.3995 PMID: 23949354
Yao M, Roebuck JC, Holsinger FC, Myers JN (2005) Elective neck dissection during salvage laryngectomy. Am J Otolaryngol 26(6):388–392. https://doi.org/10.1016/j.amjoto.2005.05.002 PMID: 16275407
Hilly O, Stern S, Horowitz E, Leshno M, Feinmesser R (2013) Is there a role for elective neck dissection with salvage laryngectomy? A decision-analysis model. Laryngoscope. 123(11):2706–2711. https://doi.org/10.1002/lary.24138 Epub 2013 May 17. PMID: 23686615
Bohannon IA, Desmond RA, Clemons L, Magnuson JS, Carroll WR, Rosenthal EL (2010) Management of the N0 neck in recurrent laryngeal squamous cell carcinoma. Laryngoscope. 120(1):58–61. https://doi.org/10.1002/lary.20675 PMID: 19877259
Freiser ME, Ojo RB, Lo K, Saint-Victor S, Bollig C, Nayak CS, Sargi ZB (2016) Complications and oncologic outcomes following elective neck dissection with salvage laryngectomy for the N0 neck. Am J Otolaryngol 37(3):186–194. https://doi.org/10.1016/j.amjoto.2016.01.004 Epub 2016 Jan 22. PMID: 27178505
Acknowledgements
Not applicable
Funding
None
Author information
Authors and Affiliations
Contributions
All authors have read and approved the manuscript. MA, revision and adjustment of research; HD, data collection and writing of the article; AH, revise pathology and revision of data; NE, revision and adjustment of research; AN writing the article and did surgeries.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in Cairo University Hospital after receiving the approval from the Research Ethics Committee, reference number: 18 804R. Written informed consents were obtained from all participants.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visithttp://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Anwar, M., Dewidar, H., Hareedy, A. et al. Role of elective neck dissection with salvage laryngectomy. Egypt J Otolaryngol 38, 55 (2022). https://doi.org/10.1186/s43163-022-00249-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-022-00249-3