
Abstract
Background
Matrix metalloproteinase 9 (MMP-9) is an important inflammatory marker in diabetic nephropathy. Many studies assessed the association between MMP-9 gene polymorphism and different microvascular complications of type 2 diabetes mellitus, though the results were inconclusive and need further exploration. Our study aimed to assess the association between MMP-9 -1562C/T gene polymorphism and diabetic nephropathy in patients with type 2 diabetes mellitus.
Results
Taking CC genotype of rs3918242 (MMP-9-1562C/T SNP) as the reference genotype and C as the reference allele, TT genotype, T allele showed significantly lower frequency in diabetic nephropathy group than without nephropathy (2.9% versus 20%, 20% versus 35.7% respectively), with the possible significant protective effect against diabetic nephropathy development (OR = 0.269, 0.450 respectively); it was considered as an independent predictor for diabetic nephropathy occurrence.
Conclusions
This study suggested that T allele of MMP-9 -1562C/T single nucleotide polymorphism had a protective role against diabetic nephropathy development and also had a role for early prediction of patients susceptible to this complication, so it helps in prevention and management of those patients.
Similar content being viewed by others

Background
Diabetes is a leading cause of end-stage renal disease worldwide [1]. Diabetic nephropathy (DN) occurs in about 25% of patients with type 2 diabetes mellitus (DM) [2]. In Egypt, 42% of diabetic patients had nephropathy [3]. Series of pathophysiological events triggered by genetic and environmental factors are involved in the development of DN [4, 5]. These events are caused not only by hemodynamic (systemic and renal hypertension, mechanical strain, altered shear stress) and metabolic changes (formation of advanced glycation end products and hyperlipidemia), but also inflammation and inflammatory molecules play an important role. One of these events is extracellular matrix protein (EMP) over-accumulation in renal glomeruli due to overproduction by glomerular mesangial cells and decrease in its degradation [6].
Matrix metalloproteinase proteins (MMPs) are endoproteinases of non-specific affinity to compounds of extracellular matrix which are involved in degradation of extracellular matrix components (collagenous and non-collagenous). They are bound by specific inhibitors known as tissue inhibitors of metalloproteinase (TIMPs). Local imbalance between the activity of MMPs and TIMPs was involved in diabetic renal remodeling [7]. Matrix metalloproteinase 9 (MMP-9) is an important inflammatory marker in DN [8]. It is released in inflammatory response by neutrophils, monocytes, macrophages, and eosinophils and plays a role in degradation of type four collagen. Its increase precedes microalbuminuria in type 2 diabetes, but its exact role is not clearly known [9]. The MMP-9 gene is located on the chromosome 20q.13.12 in humans and contains four promoter regions. MMP-9 -1562C/T is located upstream of the promoter and contains binding sites for transcriptional repressors [10]. The association of MMP-9 gene promoter polymorphism and microvascular complications of diabetes have been assessed in many studies; however, the results are inconclusive [11]. Our study hypothesized presence of association between matrix metalloproteinase-9 (MMP-9) -1562C/T gene polymorphism and diabetic nephropathy in patients with type 2 DM.
Aim of the work
The aim of this study was to assess matrix metalloproteinase-9 (MMP-9) -1562C/T gene polymorphism and its correlation with diabetic nephropathy in patients with type 2 DM.
Methods
This is a case control study done from October 2017 to June 2019. The patients enrolled in this study were thirty-five diabetic patients with diabetic nephropathy (DN) and thirty-five diabetic patients without nephropathy (DWN), all with duration of diabetes more than 5 years. The diagnosis was based on the World Health Organization (WHO) diagnostic and classification criteria in 1999. Criteria for diagnosis of DN include serum creatinine (Cr) > 1.8 mg/dl, blood urea nitrogen (BUN) > 21.84 mg/dl, and urinary albumin excretion rate (UAER) > 30 mg/24 h confirmed in at least two independent consecutive examinations. Thirty non-diabetic persons were selected to be a control group. The control and diabetic groups were matched for age and sex.
Patients and controls were subjected to the following: full history taking, clinical examination with stress on blood pressure measurement, and examination of lower limb for edema. Type 2 DM patients, diagnosed depending on the WHO consulting criteria (i.e., [FBG] ≥ 7.0 mmol/L [126 mg/dL] and/or a 2-h post glucose value ≥ 11.1 mmol/L [200 mg/dL]) [12], with age ≥ 18 years were included in the study. Patients with other kidney disease (primary or secondary), taking nephrotoxic drugs, and pregnant females were excluded. An informed consent was taken from each participant. All data of patients were confidential with private code and used for the current medical research only.
Laboratory investigations were done for all patients and control groups as complete blood picture was done using Cell Dyn Emerald, Abbott, USA. Random blood sugar, serum creatinine, total cholesterol, and triglycerides were estimated by automated chemistry analyzer Cobas, C311 (Roche-Germany); hemoglobin (HA1c) was done using automated chemistry analyzer, Cobas Integra 400+ (Roche-Germany). Albumin and creatinine in urine were estimated for each subject by automated chemistry analyzer Cobas C311 (Roche Germany), and micro-albumin creatinine ratio (ACR) was calculated.
Polymerase chain reaction–restriction fragment length of polymorphism (PCR-RFLP)
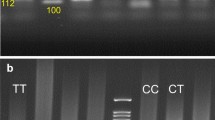
All patients and controls were subjected to molecular biology techniques for detection of SNPs of MMP-9 gene -1562C/T which include DNA extraction, polymerase chain reaction (PCR), and restriction fragment length polymorphism (RFLP) electrophoresis (Fig. 1).

PCR-RFLP with SphI restriction enzyme
DNA extraction
DNA was extracted from peripheral venous blood of all patients and control groups using the GeneJET Genomic DNA Purification Kit (Thermo Scientific) which is qualified by isolating genomic DNA from 200 μL of blood and 5 mg of mammalian tissue following described protocols. The DNA extract is stored in a refrigerator at − 20 until PCR amplification.
For amplification of the region containing the MMP-9 −1562C/T polymorphism, the following primers were used: sense primer 5-CTT CCT AGC CAG CCG GCA TC-3 and antisense 5-GCC TGG CCT ATA GTA GGC CC-3 [13]. PCR amplification was performed using DreamTaq PCR Green Master Mix (2X) (cat no k1081, Lithuania, EU). PCR was performed using the following thermal cycling conditions [13] by using thermal cycle (Bio-Rad PTC-100 Peltier, USA:
-
✓ 94 °C for 5 min
-
✓ 35 cycles of amplification at 94 °C for 35 s, 60 °C for 30 s, and 72 °C for 45 s
-
✓ 72 °C for 5 min
Digestion of PCR products with SphI restriction endonuclease Thermo Scientific FastDigest, cat no FD 0604, Lithuania, EU, to detect the MMP-9 −1562C/T SNP [13]. Separation of restriction products by electrophoresis in 2% agarose gels, after that visualization of the restriction products using an ultraviolet transilluminator.
Interpretation of MMP-9 −1562C/T allele SNPs
-
The CC genotype was not digested by the enzyme and represented by a single (435-bp) band.
-
The TT genotype was digested by SphI restriction enzyme into two bands (247 and 188 bp).
-
The CT genotype was represented by three bands (435, 247, and 188 bp).
Statistical analysis
The collected data were analyzed by using the Statistical Package for Social Sciences (SPSS/PC/VER 17).
Results
Analysis of the demographic data showed that 49 (49%) of the study population were males, divided as twenty have DN, sixteen diabetic without nephropathy (DWN), and thirteen controls, while 51 (51%) were females, divided as fifteen have DN, nineteen DWN, and seventeen controls, with mean ages of 58 ± 12.3, 58.9 ± 8.5, and 55.7 ± 15.2 years in DN, DWN, and control group, respectively. No significant differences were found in age and gender distribution among the studied groups (Table 1).
Systolic blood pressure (SBP) was significantly higher in DN group when compared to control or DWN groups, while diastolic blood pressure (DBP) was not significantly different among all groups. Number of patients with hypertension was significantly higher in the DN group than in control and in the DWN groups (Table 1).
Fasting blood glucose (FBG) and glycosylated hemoglobin (HbA1c) were significantly more elevated in the DN group than the control and DWN groups, and also significantly more raised in DWN than control group. Serum creatinine, total cholesterol (TC) and triglyceride (TG), and ACR levels were significantly higher in the DN group than the control and DWN groups (Table 1).
The rs3918242 (-1562C/T) SNP had C and T alleles. C is the reference allele. It is located on the long arm of chromosome 20 within matrix metallopeptidase 9 (MMP-9) gene (Table 2).
Applying Hardy-Weinberg equation revealed MMP-9 -1562C/T SNP (rs3918242) genotypes in all studied groups. There were CC genotypes in 11, CT in 11, and TT in 8 subjects of the control group, while CC genotypes were in 17, CT in 11, and TT in 7 patients of the DWN group, but in the DN group, we found CC genotype in 22 patients, CT in 12 patients, and TT in one patient in Hardy-Weinberg equilibrium (Table 3).
Taking rs3918242 (MMP-9 -1562C/T SNP) CC as the reference genotype and C as the reference allele in all studied groups (Fig. 2), no significant associations were found in genotypes and allele frequencies between the DWN cases and control group (Table 4), while DN group had significantly lower frequencies of TT, CT + TT genotypes, and T allele when compared to the control group (2.9% versus 26.7%, 37.1% versus 63.3%, and 20% versus 45% respectively), with significant protective effect of T allele against DN development (Table 5). Moreover, TT genotype and T allele showed significantly lower frequency in the DN group when compared to the DWN group (2.9% versus 20%, and 20% versus 35.7% respectively), with significant protective effect against DN development (Table 6).

MMP-9 rs3918242 genotypes in all studied groups
Logistic regression analysis was conducted for prediction of DN development using various risk factors including age, gender, hypertension, HBA1C, TC, TG, and MMP-9 -1562C/T SNP (rs3918242) genotypes. Hypertension, higher HBA1C, TC, and TG were associated with DN occurrence while TT genotype was protective against DN in univariable analysis. Considering significant covariates in univariable analysis, multivariable analysis revealed that hypertension, higher HBA1C, and TC, but not TG, were considered as risk predictors for DN development while TT genotype was significant predictor for protection against DN development (Table 7).
Discussion
Many factors contribute to the development of diabetic nephropathy, including metabolic, hemodynamics, and inflammatory changes. These factors help the development of DN through the accumulation of extracellular matrix protein (ECM), thickening of glomerular basement membrane (GBM), endothelial dysfunction, tubular fibrosis, and hyalinosis of renal arterioles [14, 15]. Matrix metalloproteinase 9 (MMP-9) belongs to gelatinases; it is known also as gelatinase B or type IV collagenase. It plays an important role in extracellular matrix degradation and remodeling [16]. Bai et al. suggested that exposure to hyperglycemia increases or decreases MMP-9 production; this may contribute to the abnormality of GBM produced by an imbalance in extracellular matrix synthesis and degradation, and may have a critical role in the pathogenesis of DN [17].
The association of MMP-9 gene promoter polymorphism and microvascular diabetic complications had been assessed in previous studies [18,19,20]. Nevertheless, the results are inconclusive [11], so the current study aimed to assess the association between (MMP-9) -1562C/T gene polymorphism and DN in type 2 DM. The patients enrolled in this study were thirty-five diabetic patients with DN, thirty-five diabetic patients without DN, and thirty non-diabetic personnel as a healthy control group.
In the current study, there was a non-significant difference between patients with DN and DWN as regard age and gender. This is in agreement with Palazhy and Viswanathan, who found that age and sex were comparable in patients with and without DN [21]. Also, another study found that the prevalence of diabetic kidney disease remained stable among the age group [22], as well as other researchers reported that diabetic nephropathy affects male and female sex equally [23]. However, other studies stated that male gender is a risk factor for diabetic nephropathy development and progression in type 2 diabetic patients [24, 25].
Additionally, Russo et al. reported that male sex, age, and DM duration were more prevalent in the albuminuria group of type 2 diabetic patients [26]; this discrepancy might be attributable to different characteristics of studied diabetic patients than our study as they studied elderly people, correspondingly the exposure to higher drugs, side effects of management of DN, including hypoglycemia, and frequent co-morbidities [27].
Hypertension is highly prevalent in type 2 diabetic patients with DN. Mechanisms of hypertension in DN include activation of renal renin-angiotensin-aldosterone system activation, increased sympathetic nervous system activity, endothelial cell dysfunction, reactive oxygen species upregulation, and nitric oxide downregulation. These mechanisms have the main role in the onset and deterioration of hypertension in these patients with DN [28]. This is in agreement with our results, which showed that hypertension was significantly higher in the DN group than in the control or the DWN groups. Moreover, the risk factor profile was worst in the DN group; previous study showed higher HBA1c, triglycerides ≥ 150 mg/dl, and BP ≥ 140/85 mmHg in the albuminuria positive group [26]. This is in partial harmony with our results, which showed that systolic BP, FBG, and HbA1C, TC, and TG levels were significantly higher in the group with DN than without. Though Palazhy and Viswanathan concluded that dyslipidemia (high TG, low HDL, and high LDL) was highly prevalent among diabetic patients with nephropathy, this is in agreement with our data, but on contrary, they found that hypertension and HBA1C were comparable in both groups (DN and DWN) [21].
Also, in the study done by Low et al., which included diabetic patients with CKD, defined by GFR < 60 mL/min per 1.73 m2 or ACR ≥ 30 mg/g in one spot urine analysis, they restated that the main traditional risk factors as smoking, hyperglycemia, dyslipidemia, and hypertension were associated with chronic kidney disease [29]. On the other hand, Okada et al. showed that systolic blood pressure visit-to-visit variability was a risk factor for the progression or development of albuminuria [30]. Also, annual FPG and HbA1c variations have a strong association with diabetic nephropathy in patients with type 2 diabetes [31].
In our study, the DWN group and control group showed non-significant difference as regard frequency of alleles and genotypes of MMP-9 (-1562C/T) gene polymorphism, and we found that TT genotype and T allele frequencies were significantly lower in DN when compared to the control and DWN groups, with the possibility of a protective effect of T allele against DN development. This is in harmony with Feng et al. [13]. This protective role of the T allele could be explained by transcriptional suppression that is decreased so the expression of MMP-9 is elevated, which leads to increase degradation of ECM, delayed interstitial fibrosis, and renal glomerular sclerosis with the subsequent delay in DN development and progression [13], while Feng et al. found that as regard T allele frequency, the DN group was different when compared with the DWN group, but did not reach statistically significant values. Conflicting to our results, Singh et al. revealed that the allele distribution differed significantly between diabetic patients without complications and the normal control group [20]. This difference between the two results might be attributable to dissimilar diabetic complications in these two works.
In the current study, logistic regression analysis showed that hypertension, TC, and TG were associated with DN occurrence while the TT genotype was protective against DN in univariable analysis.
However, the multivariate analysis revealed that hypertension, higher TC, HBA1c, and MMP-9 -1562C/T SNP (rs3918242) TT genotype were considered as risk predictors for DN development. This is in partial harmony with Feng et al., who reported that SBP, TG, and TC were independent risk factors for DN, and TT genotype of MMP-9 -1562C/T SNP (rs3918242) was a protective factor against DN [13]. Additionally, in the meta-analysis which was retrieved from PubMed, Medline, Embase, China National Knowledge Infrastructure, Web of Science, and Cochrane databases, there was a significant association between the MMP-9-1562 C/T genotype and the risk of DN in Asians, and the MMP-9-1562 T gene mutation might reduce the risk of DN [11].
The current study acknowledges some limitations including a small sample size; we advise further study with a large number of populations to ascertain the role of MMP-9 gene polymorphisms in DN prediction.
Conclusions
This study suggested the protective role of the T allele of MMP-9 SNP (-1562C/T) gene polymorphism and lower HbA1c against diabetic nephropathy development. This may be useful in the early prediction of patients susceptible to diabetic nephropathy and for further early prevention and management.
Availability of data and materials
The data that support the findings of this study are available from Rania Bahriz (corresponding author). Study was done in Diabetes and Endocrinology unit and outpatient diabetic clinics of Specialized Medical Hospital at Mansoura University, Egypt.
Abbreviations
- <:
-
Less than
- >:
-
More than
- ACR:
-
Albumin creatinine ratio
- BUN:
-
Blood urea nitrogen
- DM:
-
Diabetes mellitus
- DN:
-
Diabetic nephropathy
- DWN:
-
Diabetic without nephropathy
- EMP:
-
Extracellular matrix proteins
- FBG:
-
Fasting blood glucose
- GBM:
-
Glomerular basement membrane
- GFR:
-
Glomerular filtration rate
- HbA1c:
-
Hemoglobin A1c
- MMPs:
-
Matrix metalloproteinase proteins
- MMP-9:
-
Matrix metalloproteinase 9
- PCR:
-
Polymerase chain reaction
- RFLP:
-
Restriction fragment length polymorphism
- SBP:
-
Systolic blood pressure
- SPSS:
-
Statistical Package for Social Sciences
- Cr:
-
Serum creatinine
- TIMPs:
-
Tissue inhibitors of metalloproteinase
- TC:
-
Total cholesterol
- TG:
-
Triglyceride
- UAER:
-
Urinary albumin excretion rate
- WHO:
-
World Health Organization
References
Ritz E, Rychlík I, Locatelli F, Halimi S (1999) End-stage renal failure in type 2 diabetes: a medical catastrophe of worldwide dimensions. Am J Kidney Dis 34(5):795–808
Tuttle KR, Bakris GL, Bilous RW, Chiang JL, De Boer IH, Goldstein-Fuchs J, Neumiller JJ (2014) Diabetic kidney disease: a report from an ADA Consensus Conference. Am J Kidney Dis 64(4):510–533
Gheith O, Othman N, Maher A, Rida S, Halim MA, Abduo H, Al-Otaibi T (2018) Prevalence of diabetic kidney disease before and after renal transplantation in Arab countries. J Egypt Soc Nephrol Transplant 18(3):59
Wolf G (2004) New insights into the pathophysiology of diabetic nephropathy: from haemodynamics to molecular pathology. Eur J Clin Invest 34(12):785–796
Martini S, Eichinger F, Nair V, Kretzler M (2008) Defining human diabetic nephropathy on the molecular level: integration of transcriptomic profiles with biological knowledge. Rev Endocr Metab Disord 9(4):267–274
Cooper ME (2001) Interaction of metabolic and haemodynamic factors in mediating experimental diabetic nephropathy. Diabetologia 44(11):1957–1972
Zaoui P, Cantin JF, Alimardani-Bessette M, Monier F, Halimi S, Morei F, Cordonnier D (2000) Role of metalloproteases and inhibitors in the occurrence and progression of diabetic renal lesions. Diabete Metab 26:25–29
van der Zijl NJ, Hanemaaijer R, Tushuizen ME, Schindhelm RK, Boerop J, Rustemeijer C, Diamant M (2010) Urinary matrix metalloproteinase-8 and-9 activities in type 2 diabetic subjects: a marker of incipient diabetic nephropathy? Clin Biochem 43(7-8):635–639
Ebihara I, Nakamura T, Shimada N, Koide H (1998) Increased plasma metalloproteinase-9 concentrations precede development of microalbuminuria in non-insulin-dependent diabetes mellitus. Am J Kidney Dis 32(4):544–550
Clark IM, Swingler TE, Sampieri CL, Edwards DR (2008) The regulation of matrix metalloproteinases and their inhibitors. Int J Biochem Cell Biol 40(6-7):1362–1378
Zhang Z, Wu X, Cai T, Gao W, Zhou X, Zhao J, Liao L (2015) Matrix metalloproteinase 9 gene promoter (rs 3918242) mutation reduces the risk of diabetic microvascular complications. Int J Environ Res Public Health 12(7):8023–8033
Kruger DF, Boucher JL, Banerji MA (2011) Utilizing current diagnostic criteria and treatment algorithms for managing type 2 diabetes mellitus. Postgrad Med 123(4):54–62
Feng S, Ye G, Bai S, Wei H, Liao X, Li L (2016) Matrix metalloproteinase-9− 1562C/T gene polymorphism is associated with diabetic nephropathy. Biomed Res Int 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5007315/
Satirapoj B, Adler SG (2014) Comprehensive approach to diabetic nephropathy. Kidney Res Clin Pract 33(3):121–131
Umanath K, Lewis JB (2018) Update on diabetic nephropathy: core curriculum 2018. Am J Kidney Dis 71(6):884–895
Ho HY, Lin CW, Chien MH, Reiter RJ, Su SC, Hsieh YH, Yang SF (2016) Melatonin suppresses TPA-induced metastasis by downregulating matrix metalloproteinase-9 expression through JNK/SP-1 signaling in nasopharyngeal carcinoma. J Pineal Res 61(4):479–492
Bai Y, Wang L, Li Y, Liu S, Li J, Wang H, Huang H (2006) High ambient glucose levels modulates the production of MMP-9 and a5 (IV) collagen by cultured podocytes. Cell Physiol Biochem 17(1-2):57–68
Beránek M, Kolar P, Tschoplova S, Kankova K, Vasku A (2008) Genetic variations and plasma levels of gelatinase A (matrix metalloproteinase-2) and gelatinase B (matrix metalloproteinase-9) in proliferative diabetic retinopathy. Mol Vis 14:1114
Ahluwalia TS, Khullar M, Ahuja M, Kohli HS, Bhansali A, Mohan V, Venkatesan R, Rai TS, Sud K, Singal PK (2009) Common variants of inflammatory cytokine genes are associated with risk of nephropathy in type 2 diabetes among Asian Indians. PLoS One 4(4):e5168
Singh K, Agrawal NK, Gupta SK, Singh K (2013) A functional single nucleotide polymorphism-1562C > T in the matrix metalloproteinase-9 promoter is associated with type 2 diabetes and diabetic foot ulcers. Int J Low Extrem Wounds 12(3):199–204
Palazhy S, Viswanathan V (2017) Lipid abnormalities in type 2 diabetes mellitus patients with overt nephropathy. Diabetes Metab J 41(2):128–134
De Boer IH, Rue TC, Hall YN, Heagerty PJ, Weiss NS, Himmelfarb J (2011) Temporal trends in the prevalence of diabetic kidney disease in the United States. JAMA 305:2532–2539
Pavkov ME, Bennett PH, Knowler WC, Krakoff J, Sievers ML, Nelson RG (2006) Effect of youth-onset type 2 diabetes mellitus on incidence of end-stage renal disease and mortality in young and middle-aged Pima Indians. JAMA 296:421–426
Neugarten J, Golestaneh L (2013) Gender and the prevalence and progression of renal disease. Adv Chronic Kidney Dis 20(5):390–395
Gheith O, Othman N, Nampoory N, Halimb MA, Al-Otaibi T (2016) Diabetic kidney disease: difference in the prevalence and risk factors worldwide. J Egypt Soc Nephrol Transplant 16(3):65
Russo GT, De Cosmo S, Viazzi F, Mirijello A, Ceriello A, Guida P, Giorda C, Cucinotta D, Pontremoli R, Fioretto P (2018) AMD-Annals Study Group. Diabetic kidney disease in the elderly: prevalence and clinical correlates. BMC Geriatr 18(1):38
Huang ES (2016) Management of diabetes mellitus in older people with comorbidities. BMJ 353:i2200
Van Buren PN, Toto R (2011) Hypertension in diabetic nephropathy: epidemiology, mechanisms, and management. Adv Chronic Kidney Dis 18(1):28–41
Low SK, Sum CF, Yeoh LY, Tavintharan S, Ng XW, Lee SB, Lim SC (2015) Prevalence of chronic kidney disease in adults with type 2 diabetes mellitus. Ann Acad Med Singapore 44(5):164–171
Okada H, Fukui M, Tanaka M, Matsumoto S, Mineoka Y, Nakanishi N, Nakamura N (2013) Visit-to-visit blood pressure variability is a novel risk factor for the development and progression of diabetic nephropathy in patients with type 2 diabetes. Diabetes Care 36(7):1908–1912
Lin CC, Chen CC, Chen FN, Li CI, Liu CS, Lin WY, Li TC (2013) Risks of diabetic nephropathy with variation in hemoglobin A1c and fasting plasma glucose. Am J Med 126(11):1017–10e1
Acknowledgements
To all mentioned authors only.
Not applicable for any other researchers.
Funding
This research is not funded.
Author information
Authors and Affiliations
Contributions
Author 1: KS: (1st author): gave the idea of the research and shared in clinical part, writing of the research, statistical analysis, and data reviewing and interpretation. Author 2: RB (corresponding author): shared in clinical part of the research, writing, statistical analysis, and data reviewing and interpretation. Author 3: NM: shared in the laboratory part of the research, shared in writing, statistical analysis, and data reviewing. Author 4: ME: responsible for the laboratory part of the research, shared in writing, statistical analysis, and data reviewing. Author 5: GE: shared in clinical part of the research, shared in writing, statistical analysis, and data reviewing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the ethics committee of Mansoura University on 15 September 2017 with approval number [Ms.17.08.60]. The patients provided written consent.
Consent for publication
Consent for publication was taken from all participants in the study.
Competing interests
The authors declare that they have no competing interests in this section.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shalaby, K., Bahriz, R., Mahsoub, N. et al. Matrix metalloproteinase-9 gene polymorphism (-1562 C/T) and its correlation with diabetic nephropathy. Egypt J Intern Med 33, 7 (2021). https://doi.org/10.1186/s43162-021-00035-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43162-021-00035-2