
Abstract
Background
Joubert syndrome (JS) is a rare autosomal recessive genetic heterogeneously inherited disorder characterized by neurological features that include hypotonia, ataxia, developmental delay, intellectual disability, abnormal eye movements, and neonatal breathing dysregulation.
Case presentation
The main purposes of the case report are to highlight the benefit of multidisciplinary rehabilitation team approach and describe the clinical features associated with Joubert syndrome. In this case report, we have discussed a 9-month-old girl who presented with developmental delay, impaired vision, and a history of recurrent respiratory infection with respiratory distress. On examination, she had facial dysmorphism, myopia, and hypotonia. Brain magnetic resonance imaging showed a thick, elongated, and abnormally oriented superior cerebellar peduncle showing molar tooth appearance with elongated bat-wing shaped 4th ventricle and hypoplasia of the vermis suggestive of JS. The patient has been treated at Garden Reach Institute for the Rehabilitation and Research (GRIRR), Kolkata, India, by a multidisciplinary team of physiotherapist, speech therapist, special educator, orthotist, medical officer, and social worker that shown excellent improvement in her condition, and she has achieved good sitting balance, able to sit without support, stand with wall support, and able to walk using bilateral AFO and reverse walker.
Conclusion
Knowledge of characteristic clinical and radiological findings in JS will help in early diagnosis and successful rehabilitation.
Similar content being viewed by others


Background
Joubert syndrome (JS) is a rare autosomal recessive genetic heterogeneously inherited disorder characterized by neurological features that include hypotonia, ataxia, developmental delay, intellectual disability, abnormal eye movements, and neonatal breathing dysregulation [1]. It can be diagnosed on the basis of clinical presentation and the presence of the molar tooth sign (MTS) on brain axial magnetic resonance imaging (MRI) [1, 2].
The reported prevalence of JS, commonly ranges from 1:80,000 to 100,000 live births, is probably underestimated due to the lower number of case reports of MTS in the literature [2, 3]. This signifies the case reporting of JS as epidemiological data such as population-based prevalence rates are almost completely lacking. As it represents like a delayed developmental milestone, most of the cases may not be diagnosed in the early phase of childhood; however, the presence of respiratory distress along with delayed developmental milestones may raise the suspicion and diagnosis of JS [4]. Maria et al. reported 33 months as an average age for its diagnosis [5]. Most children with this syndrome survive infancy to reach adulthood [6]. Early detection of this condition is essential so that multidisciplinary intervention, i.e., medical management along with rehabilitation, can be started as early as possible.
Case presentation
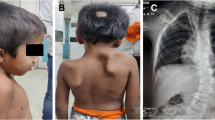
A 9-month-old baby girl presented to the Department of Paediatrics, IPGMER Hospital, Kolkata, India, with a history of fever for 2 days and respiratory distress, where she was diagnosed with Joubert syndrome with associated respiratory tract infection and recurrent seizure disorders. It was a known follow-up case of hypoxic ischemic encephalopathy (HIE) stage II with laryngomalacia and was on medication for the convulsions. The diagnosis of JS was made on the basis of a brain MRI, which showed thick, elongated, and abnormally oriented superior cerebellar peduncle showing molar tooth appearance with elongated bat-wing shaped 4th ventricle and hypoplasia of the vermis. JS can be classified into 6 subtypes: pure JS, JS with ocular defect (JS-O), JS with renal defect (JS-R), JS with oculo-renal defects (JS-OR), JS with hepatic defect (JS-H), and JS with oro-facio-digital defects. In our case, on clinical examination, there was a presence of myopia and facial dysmorphism with specific facial features such as low-set ears and frontal blossing; however, polydactyly was absent. On neurological and physical examination, there was a presence of hypersensitivity, thumb sucking, poor muscle tone, and poor motor development which denotes pathological presence of moro reflex, rooting reflex, asymmetric tonic neck reflex, tonic labyrinthine reflex, and landau reflex. There is no report of retinopathy and associated eye disorders. Moreover, the child has no pathological features of suspected renal disorders and neurocutaneous markers. There is a lack of evidence to confirm or exclude hepatic defect as the child was not referred to a specialist for it. This might be due to a potential lack of clinical awareness or due to the illiteracy of her parents.
Laboratory investigations, including complete blood count, blood sugar, electrolytes, C-reactive protein, liver enzymes, urea and creatinine, TSH, and free T4 and T3, were all normal. She was a full-term baby, delivered normally with no history of perinatal complications or positive consanguinity. She was about 2.5 kg at birth and had a delayed birth cry. There was no history of consanguineous marriage. There was a history of recurrent respiratory infection at the age of 3 years.
At the age of 3 years, she was brought to Garden Reach Institute for the Rehabilitation and Research (GRIRR), Kolkata, a non-governmental organization working for the underprivileged and disabled children. GRIRR has a multidisciplinary team of physiotherapist, speech therapist, special educator, orthotist, medical officer, and social worker. The initial physical assessment and evaluation were made by the team that found facial dysmorphism with specific facial features such as low-set ears, frontal blossing, lack of neck and head control, unable to sit (supported or unsupported), unable to stand (supported or unsupported), hypotonic upper and lower extremities, unable to make a sound even for cry, no vocal response to stimulus, and drowsy eyes with no eye movement. No polydactyly has been noted. The initial goals and interventions were decided with the multidisciplinary team, and rehabilitation was initiated in a full-fledged manner.
The child has received a 90-min treatment session, 6 days/week that includes physiotherapy and in-between speech therapy. The physiotherapy intervention included positioning, sensory integration therapy, and functional activities to facilitate the required developmental milestones. Other exercises include weight-bearing and joint compression techniques, stretching, motor control activities using gym ball, instrument-assisted ADL activities, hand function activities, and use of assistive and orthotic devices such as special chair, bilateral ankle foot orthoses (AFO), standing frame, and balance board.
She has continued her treatment sessions at GRIRR from the age of 3 years to date (age 6 years) with the multidisciplinary team. She has shown excellent improvement in her condition, and she has achieved good sitting balance, able to sit without support, stand with wall support, and able to walk using bilateral AFO and reverse walker. She also responds to her name and other conversations and also makes a sound like papa and cha. No adverse reaction was noted in the last 3 years. She continues the medication for seizures with regular follow-up with the clinician.
Conclusion
Hypotonia during infancy and developmental delay with or without mental retardation, associated with abnormal breathing patterns and abnormal eye movements (nystagmus), are the most important clinical signs and symptoms to suspect the case of JS [7]. However, the radiological presence of “molar tooth sign” on the brain MRI is an essential component to confirm the diagnosis. The present case had all the clinical symptoms with the exception of nystagmus and mental retardation which may have been overlooked.
The main findings from cranial MRI studies are (1) cerebellar vermis hypoplasia, (2) deepened interpeduncular fossa, and (3) thick and horizontal enlarged superior cerebellar peduncles [4]. The present case had all the findings radiologically. However, cerebellar vermis hypoplasia had been reported as a component of other disorders like trisomy 21, occipital encephalocele, and dandy walker malformation [1, 8, 9]. Besides, hypotonia is associated with other features to be considered as an essential clinical feature [10].
Genetic counseling has been recommended as one of the important measures to prevent JS. Prenatal diagnosis of JS is feasible through chorionic villus sampling at about 11 weeks of gestation [1, 10]. Fetal ultrasound may be useful to diagnose high-risk pregnancies as it showed increased nuchal translucency. The prognosis of JS cases may be good, if diagnosed in early childhood and managed early through a multidisciplinary intervention program including physical therapy, special education, occupational, and speech therapy. The early intervention has shown significant benefits in the advancement of developmental milestones for several patients with JS [11]. Unfortunately, she has received a late multidisciplinary intervention at the age of 3 years, though she showed a remarkable improvement in her condition and the parents were happy. Renal and retinal dysfunction can be progressive. In patients with retinal anomalies, the renal function should be monitored regularly, and ultrasonography should be done to detect cystic renal disease. The diagnosis is important for future procedures that require anesthesia because these patients are sensitive to respiratory depressant effects of anesthetic agents like opiates and nitrous oxide. Hence, the use of these anesthetic agents should be avoided in these patients [12].
We have discussed it to highlight the benefit of multidisciplinary rehabilitation team approach for better outcomes and to summarize the main clinical and radiological milestones for JS diagnosis. Through this scientific article, we also emphasize to promote awareness regarding disabilities of the child and in the improvement of developmental milestones, balance, and walking with a multidisciplinary team approach.
Availability of data and materials
All the data related to the diagnostic imaging, doctor’s prescription confirming the diagnosis, physical therapy, and rehabilitation-related documents are available.
Abbreviations
- JS:
-
Joubert syndrome
- GRIRR:
-
Garden Reach Institute for the Rehabilitation and Research
- MTS:
-
Molar tooth sign
- MRI:
-
Magnetic resonance imaging
- HIE:
-
Hypoxic ischemic encephalopathy
- ADL:
-
Activities of daily living
- AFO:
-
Ankle-foot orthoses
- JS-O:
-
Joubert syndrome with ocular defect
- JS-R:
-
Joubert syndrome with renal defect
- JS-OR:
-
Joubert syndrome with oculo-renal defects
- JS-H:
-
Joubert syndrome with hepatic defect
References
Brancati F, Dallapiccola B, Valente EM. Joubert syndrome and related disorders. Orphanet J Rare Dis. 2010;5(1):20. https://doi.org/10.1186/1750-1172-5-20.
Nuovo S, Bacigalupo I, Ginevrino M, et al. Age and sex prevalence estimate of Joubert syndrome in Italy. Neurology. 2020;94:797–801.
Boltshauser E, Isler W. Joubert syndrome: episodic hyperpnea, abnormal eye movements, retardation and ataxia, associated with dysplasia of the cerebellar vermis. Neuropadiatrie. 1977;8(1):57–66. https://doi.org/10.1055/s-0028-1091505.
Akcakus M, Gunes T, Kumandas S, Kurtoglu S, Coskun A. Joubert syndrome: report of a neonatal case. Paediatr Child Health. 2003;8(8):499–502. https://doi.org/10.1093/pch/8.8.499.
Maria BL, Quisling RG, Rosainz LC, Yachnis AT, Gitten J, Dede D, et al. Molar tooth sign in Joubert syndrome: clinical, radiologic, and pathologic significance. J Child Neurol. 1999;14(6):368–76. https://doi.org/10.1177/088307389901400605.
Alharabi KM. Joubert syndrome: a rare case report from Saudi Arabia. J Med Cases. 2017;8(6):180–2. https://doi.org/10.14740/jmc2832w.
Parisi MA, Doherty D, Chance PF, Glass IA. Joubert syndrome (and related disorders) (OMIM 213300). Eur J Human Genet Vol. 2007;15:511–21.
Satran D, Pierpont ME, Dobyns WB. Cerebello-oculorenal syndromes including Arima, Senior-Loken and COACH syndromes: more than just variants of Joubert syndrome. Am J Med Genet. 1999;86(5):459–69. https://doi.org/10.1002/(SICI)1096-8628(19991029)86:5<459::AID-AJMG12>3.0.CO;2-C.
Aslan H, Ulker V, Gulcan EM, Numanoglu C, Gul A, Agar M, et al. Prenatal diagnosis of Joubert syndrome: a case report. Prenat Diagn. 2002;22(1):13–6. https://doi.org/10.1002/pd.220.
Saraiva JM, Baraitser M. Joubert syndrome: a review. Am J Med Genet. 1992;43(4):726–31. https://doi.org/10.1002/ajmg.1320430415.
Parisi MA. Clinical and molecular features of Joubert syndrome and related disorders. Am J Med Genet C. 2009;151C(4):326–40. https://doi.org/10.1002/ajmg.c.30229.
Singh P, Goraya JS, Saggar K, Ahluwalia A. A report of Joubert syndrome in an infant, with literature review. J Pediatr Neurosci. 2011;6(1):44–7.
Acknowledgements
We acknowledge the parents of the child who has supported throughout.
Funding
No grants and funding have been received for the case report.
Author information
Authors and Affiliations
Contributions
S.A. and F.K have contributed to the formation, data collection, manuscript preparation, and manuscript finalization. N.K has contributed to the manuscript preparation and maintaining the patient’s record. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The guardian of the child (as the patient is a minor) has given consent to participate.
Consent for publication
The guardian of the child (as the patient is a minor) has given consent to publish the data. Written informed consent to publish this information was obtained from the parents and/or legal guardian of the study participant.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alam, S., Khatoon, F. & Khan, N. Joubert syndrome: a case report. Bull Fac Phys Ther 26, 18 (2021). https://doi.org/10.1186/s43161-021-00039-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43161-021-00039-7