
Abstract
Background
Drug metabolism is crucial to attaining the therapeutic index of any drug. The metabolism and elimination of the drugs are governed mainly by P-glycoprotein (P-gp) and Cytochrome P450 (CYP). Paracetamol is mostly used as analgesic and antipyretic agent. The metabolism of paracetamol is primarily via Glucuronidation and sulphation at therapeutic doses. About 5–10% of paracetamol is metabolized via CYP mediated pathway. Cytochrome P450 2E1 (CYP2E1) is primarily responsible for forming a toxic metabolite of paracetamol called N-acetyl-p-benzoquinoneimine (NAPQI). Even at therapeutic doses, long-term usage of paracetamol leads to the hepatic and nephrotoxicity because of NAPQI. Several in-vitro and in-vivo studies conducted by different research groups and reported that chlorzoxazone is a substrate and inhibitor of CYP2E1. However, the effect of chlorzoxazone on the paracetamol (CYP2E1 substrate) metabolism via the CYP2E1 has not yet been reported. This study investigated the effect of chlorzoxazone on the CYP2E1-mediated metabolism of Paracetamol and NAPQI formation in Wistar rats.
Results
For 15 days, animals were orally administered with Paracetamol (300 mg/kg) with and without Silymarin (100 mg/kg) (standard CYP2E1 inhibitor) and Chlorzoxazone (50 and 100 mg/kg). Analysis was performed using RP-HPLC on the 15th day to determine paracetamol and NAPQI concentration in the plasma. Paracetamol combination with chlorzoxazone (50 and 100 mg/kg) showed a dose-dependent increase in the AUC0–∞ and the peak plasma concentration (Cmax) of Paracetamol and a dose-dependent decrease of AUC0–∞ and Cmax of NAPQI compared to paracetamol control (p < 0.001). Chlorzoxazone significantly decreased the elevated liver and renal markers compared to paracetamol control. Simultaneously, Hepatic and nephrotic tissue studies showed that compared to the paracetamol control group, the combination of chlorzoxazone significantly ameliorated paracetamol-induced hepatotoxicity and nephrotoxicity.
Conclusion
Finally, this study revealed that paracetamol in combination with chlorzoxazone led to a significant decrease in the plasma levels of NAPQI and enhanced absorption of paracetamol in rats via the inhibition of CYP2E1- mediated metabolism. In addition, chlorzoxazone significantly ameliorated paracetamol-induced hepatotoxicity and nephrotoxicity.
Similar content being viewed by others

Introduction
Hepatic enzymes play a crucial role in drug metabolism and subsequent elimination from the body. Cytochrome P450 (CYP) are the isozymes in the liver responsible for drug metabolism. CYP2E1 is one among this enzymatic family involved in the oxidation of ethanol and a diverse group of suspected carcinogens [1, 2]. Paracetamol is the most prescribed analgesic and antipyretic drug worldwide. However, several drugs have previously investigated paracetamol to study the interactions with acetaminophen. Glucuronidation and sulphation are the primary ways paracetamol is metabolized at the therapeutic dose, as shown in Fig. 1. Glucuronide and sulfate conjugates are other ways paracetamol is excreted in the urine, contributing approximately 40–60 and 20–30% of paracetamol, respectively. CYP2E1 is responsible for the metabolism of 5–10% of the paracetamol, resulting in the formation of reactive electrophilic metabolite N-acetyl-p-benzoquinoneimine (NAPQI). In addition, previous studies reported that NAPQI results in paracetamol poisoning via hepatic and nephrotic damage. [3, 4]

Metabolism of paracetamol and chlorzoxazone by CYP2E1. NAPQI, N-acetyl-p-benzoquinoneimine; CYP2E1, Cytochrome P450-2E1
Previous studies revealed that several compounds and naturally occurring flavonoids, when administered along with paracetamol, have been shown to protect against paracetamol toxicity caused by the excessive and long-term administration of paracetamol, even at therapeutic doses. The protective nature of these compounds was due to the inhibition of the CYP2E1 hepatic enzyme responsible for the metabolism of paracetamol and the formation of NAPQI [5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21]. To further understand the role of CYPE1 inhibition on the formation of NAPQI, we have selected Chlorzoxazone (CLZ), which is known to be a standard inhibitor and used in the phenotyping of CYP2E1. Chlorzoxazone is well known to be a centrally acting muscle relaxant and is mainly metabolized to 6-hydroxychlorzoxazone by this pathway [22, 23]. However, the role of CLZ in paracetamol metabolism via CYP2E1 is not yet known. Therefore, this study investigated the effect of Chlorzoxazone on the CYP2E1-mediated paracetamol metabolism by estimating NAPQI concentrations in Wistar rats.
Materials and methods
Drugs and chemicals
Paracetamol and Chlorzoxazone were gifted by Lancer Pharmaceuticals Pvt. Ltd, Baddi, India. Sigma Chemical Co. (St. Louis, MO) was approached to purchase Silymarin and N-acetyl-p-benzoquinoneimine (NAPQI). Finar Chemicals Ltd, Ahmadabad, India, was closed to buy Methanol, Triethylamine, Orthophosphoric acid, and water for HPLC analysis. Transasia Bio-Medicals Limited, Solan, Himachal Pradesh, India, was approached to purchase standard kits to perform the biochemical analysis (to estimate liver and kidney function). An analytical grade of chemicals and reagents were used in this study.
Animal experiments
Animal studies were conducted with the approval and support of the KVSR Siddhartha School of Pharmaceutical Sciences (SCOPS) Vijayawada Andhra Pradesh, India (Protocol No: KVSRSCOPS/11-03-14-007). The Govt. of India approved the college for animal studies (993/PO/E/S/06/CPCSEA). Mahaveer Enterprises, Hyderabad, and Telangana State, India, was approached to purchase Male Wistar rats (180–220 g). Animal food was purchased from (Hindustan Switch, Mumbai, India). Rats were held under the standard research condition of light–dark cycles, temperature, and humidity for at least seven days before the trials.
In-vivo studies
Paracetamol, Silymarin, and Chlorzoxazone were suspended individually in 0.5% sodium carboxymethyl cellulose (SCMC) for oral administration. Five groups of male Wistar rats, with six rats in each group, were divided and treated according to the plan consecutively once daily for 15 days as described in our earlier studies by [24,25,26,27,28,29,30]. Earlier studies were used to calculate and select the doses of paracetamol [28], Chlorzoxazone [31, 32], and Silymarin [24, 33,34,35] with the following
-
Group I: Treated with 0.5% SCMC (0.5 mL/200 g body weight)
-
Group II: Treated with paracetamol (300 mg/kg)
-
Group III: Treated with silymarin (100 mg/kg) followed by paracetamol (300 mg/kg)
-
Group IV: Treated with chlorzoxazone (50 mg/kg) followed by paracetamol (300 mg/kg)
-
Group V: Treated with chlorzoxazone (100 mg/kg) followed by paracetamol (300 mg/kg).
About 200 μL of the blood samples were collected from each rat via tail vein at the end of the treatment for 15 days. Simultaneously an equal volume (100 μL of heparinized 0.9% NaCl (20 IU/mL) was administered to the animals following the blood collection after each time point. Blood samples were collected in heparinized Eppendorf tubes at 0.25, 0.5, 1.0, 1.5, 2.0, 4.0, 6.0, 8.0, and 12 h and maintained on the ice. The plasma separation was performed by centrifugation (Remi, R4C Compact model, Mumbai, India) at 5000 rpm for 6 min and was stored at − 20 °C until analysis.
Paracetamol and NAPQI extraction from plasma
Paracetamol and NAPQI were extracted from the rat plasma using a single-step liquid–liquid extraction method [36]. Briefly, 100 µL plasma and 100 µL of 0.3 M phosphate buffer of pH 5.0 was added and gently mixed, followed by a mixture of 5 mL of Isopropyl alcohol and chloroform (5:95 v/v). The entire mixture of solutions was vortexed and centrifuged at 3000 rpm for 5 min using a Remi vortex mixer. The resulting supernatant of 1.4 µL was removed, dried, and the dry residue was regenerated in the mobile phase of 100 µL and vortexed to facilitate mixing. The HPLC analysis was performed using 20 µL of the obtained sample.
Determination of paracetamol and NAPQI in rat plasma by RP-HPLC
The quantification of Paracetamol and NAPQI plasma concentration from rat plasma was performed as described by [36, 37], along with some improvements using a reversed phase-high pressure liquid chromatography (RP-HPLC). A Shimazdu HPLC system with Thermo Electron Corp, Beverly, MA) and a dual-wavelength PDA detector (SPD-10A VP), LC-20AT VP pump, C18 column (ODS Thermo Hypersil, 250 mm × 4.6 mm, 5.0 μm was used. Data collection and processing were performed using LC solution software. A 20:40:40 ratio of Methanol, Water, and Buffer was used as the mobile phase. A 0.45 μm nylon Millipore membrane (Millipore, Billerica, MA) was used to vacuum-filter the mobile phase. Ultrasonication (Remi, Mumbai, India) for 20 min was performed to degas the mobile phase before being used. About 20 µL was injected in to HPLC and effluent were monitored at 205 nm with a PDA detector at a 1 mL/min flow rate. The NAPQI and paracetamol retention times were obtained at about 3.919 and 6.938 min (Fig. 2).

Representative chromatograms of standard NAPQI (3.919) and paracetamol (6.938)
Method development and validation
The paracetamol and NAPQI linear range was 0.5–10 μg/mL. Five calibration samples (720, 1440, 2160, 2880, and 3600 ng/mL) were prepared from the appropriate working solutions. Graphs were plotted between concertation and peak area to obtain the calibration curves.
Calculation of pharmacokinetic parameters
Thermo Kinetica (Version 5.1, Thermo Electron Corporation, Beverly, MA) was used to perform non-compartmental PK analysis with paracetamol and NAPQI plasma concentrations. Pharmacokinetic parameters like concentration of maximum plasma (Cmax), time to reach the maximum plasma concentrations (Tmax), area under the concentration–time curve of plasma (AUC), AUC from zero to the last sampling time (AUC 0–t), AUC from time zero to infinite (AUC0–α), apparent terminal half-life (t1/2), clearance (CL/F), apparent volume of distribution (Vz/F), apparentvolume of distribution at steady state (Vss) and mean residence time (MRT) were obtained from the plasma concentrations vs time data from each rat.
Effect of chlorzoxazone and silymarin on the liver and kidney in vivo
On the 15th day of treatment, 1000 μL blood samples were collected from the retro-orbital plexus. Serum Glutamic Pyruvic Transaminase (SGPT) and Serum Glutamic-oxaloacetic Transaminase (SGOT) [38], Alkaline phosphatase (ALP) [39], total proteins [40], total bilirubin, uric acid, urea [41], blood urea nitrogen (BUN) and creatinine were estimated.
Histopathological studies
Samples for the histopathological examinations were prepared as described by [42]. Before processing the tissue samples in paraffin-embedded blocks, the liver and kidney samples of the animals used in the study were fixed in 10% neutral buffered formalin. Followed by the blinded histological examination Hematoxylin–eosin (HE) was used to cut and stain the sections (5 µm thick). Electronic light microscopy (Olympus BX-50 Olympus Corporation, Tokyo, Japan) was used to examine the Glass slides. Vascular congestion, Tissue degeneration, steatosis, and sinusoidal dilation were considered to evaluate the histopathology of the liver. Similarly, A photomicroscope was used to observe the sections of the kidneys. To consider the kidneys, normal cytoarchitecture, the presence of glomeruli, convoluted tubules, interstitium, and capillaries were observed. In contrast, kidney damage was considered to observe hemorrhage cellular necrosis, glomerular hypercellularity, tubular degeneration, and capillary congestion.
Statistical analysis
Statistical analysis was performed with Graph Pad Prism 5.0 software (San Diego, CA). One-way ANOVA followed by Dunnett’s test compared the paracetamol and NAPQI. PK parameters and plasma concentrations. A two-way ANOVA followed by the Bonferroni test was used to perfume multiple comparisons. In addition, a statistical comparison of the data obtained to evaluate the functioning of the liver and kidneys was performed in one-way ANOVA followed by Tukey’s post hoc test. The test was considered statistical significance with a p-value of less than 0.05.
Results
Effect of chlorzoxazone on the pharmacokinetics of paracetamol
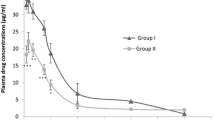
The pharmacokinetic parameters of paracetamol alone and paracetamol with silymarin (100 mg/kg) and chlorzoxazone (50 and 100 mg/kg) are shown in Table 1 and Fig. 3. The time profiles comparing paracetamol alone and in combination with Silymarin and Chlorzoxazone shows that co-administration of Silymarin and Chlorzoxazone substantially improved the plasma concertation of paracetamol. Table 1 shows the mean pharmacokinetic parameters and it is evident that silymarin and Chlorzoxazone increased the Cmax and AUC0–α of paracetamol significantly from 8.078 ± 1.344 to 10.749 ± 1.779 with silymarin (100 mg/kg), 13.590 ± 1.345 with chlorzoxazone (50 mg/kg) and 15.823 ± 1.827 μg/mL with chlorzoxazone (100 mg/kg). Similarly, the AUC0–α of paracetamol increased from 62.058 ± 16.801 to 94.118 ± 29.068 with silymarin (100 mg/kg), 89.145 ± 19.831 and 89.287 ± 13.219 μg/mL × h at the dose of 50 and 100 mg/kg, respectively.

Time profiles of Mean plasma concentration–time of Paracetamol; following an oral administration of Paracetamol to rats with or without diosmin (n = 6). (Circles) Control (paracetamol); (squares) with 100 mg/kg Silymarin and paracetamol (300 mg/kg); (traingles) with 50 mg/kg chlorzoxazone and paracetamol (300 mg/kg); (inverted traingles) paracetamol with chlorzoxazone (100 mg/kg). All values are mean ± SD. Bars represent the standard deviation. *P < 0.01, compared to the paracetamol control group (Two-way ANOVA followed by Bonferroni post-tests to compare each column to column). PCM, Paracetamol
The AUC 0–12 of Paracetamol increased significantly from 44.419 ± 8.798 to 61.816 ± 12.896 with silymarin 100 mg/kg, 68.361 ± 8.609 with chlorzoxazone (50 mg/kg) and 71.936 ± 5.500 μg/mL × h with chlorzoxazone (100 mg/kg). The t1/2 increased from 5.469 ± 2.128 to 6.916 ± 2.708 with Silymarin 100 mg/kg and 5.707 ± 3.820 h with Chlorzoxazone (50 mg/kg). It can be observed that the t½ of paracetamol increased in combination with Silymarin and Chlorzoxazone, and the tmax of the paracetamol was also increased slightly, but the t ½ and tmax change compared to control were not statistically significant. The MRT of Paracetamol was higher when Paracetamol was co-administered with Silymarin (100 mg/kg) from 9.166 ± 3.059 to 10.765 ± 3.841 and when co-administered with Chlorzoxazone 100 mg/kg the increased is to 11.008 ± 1.656 h. The CL/F of paracetamol was decreased from 0.281 ± 0.109 to 0.182 ± 0.046 with silymarin 100 mg/kg and to 0.187 ± 0.042 mL/h, 0.183 ± 0.030 with chlorzoxazone (50 and 100 mg/kg). The Vss/F of paracetamol decreased from 2.336 ± 0.528 to 1.440 ± 0.424 (chlorzoxazone 50 mg/kg) and 1.245 ± 0.129 mL/kg (chlorzoxazone 100 mg/kg). The V z/F of paracetamol decreased from 1.987 ± 0.563 to 1.398 ± 0.599 and 1.176 ± 0.248 mL/kg with chlorzoxazone 50 and 100 mg/kg, respectively.
Effect of chlorzoxazone on the pharmacokinetics of NAPQI
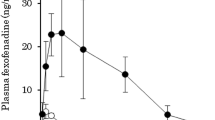
Table 2 and Fig. 4 shows the NAPQI Pharmacokinetic parameters following paracetamol oral administration to rats with or without Silymarin (100 mg/kg) and Chlorzoxazone (50 and 100 mg/kg). Pharmacokinetic parameters of NAPQI such as C max, AUC 0–12, AUC 0–∞, and t 1/2, were significantly decreased in the combination of Silymarin (100 mg/kg) and Chlorzoxazone (50 and 100 mg/kg) compared to the paracetamol control group. The C max of NAPQI was significantly decreased from 0.579 ± 0.134 to 0.514 ± 0.056 with silymarin (100 mg/kg) and to 0.434 ± 0.071 with chlorzoxazone (50 mg/kg) and to 0.300 ± 0.122 μg/mL with chlorzoxazone (100 mg/kg). The AUC 0–12 of NAPQI decreased significantly from 4.089 ± 0.521 to 2.949 ± 0.386 μg/mL × h at the dose of Chlorzoxazone (100 mg/kg). Silymarin (100 mg/kg) and chlorzoxazone (50 and 100 mg/Kg) treatment significantly decreased the AUC0–α of NAPQI from 7.892 ± 4.262 to 5.770 ± 0.886 with Silymarin 100 mg/kg and 5.123 ± 1.305 with Chlorzoxazone 50 mg/kg and to 5.730 ± 4.549 μg/mL × h with Chlorzoxazone at the dose 100 mg/kg. The tmax of NAPQI was slightly increased with 100 mg/kg of Silymarin and slightly decreased with chlorzoxazone 100 mg/kg, but statistically not significant. The t1/2 of NAPQI decreased from 9.927 ± 8.190 to 5.351 ± 1.957 with Silymarin 100 mg/kg and to 5.656 ± 11.250 h with Chlorzoxazone (100 mg/kg).

Time profiles of Mean plasma concentration–time of NAPQI following an oral administration of paracetamol to rats with or without Silymarin and Chlorzoxazone (n = 6). (Circles) Control (paracetamol); (squares) paracetamol with silymarin (100 mg/kg); (traingles) paracetamol with chlorzoxazone (50 mg/kg); (inverted traingles) paracetamol with chlorzoxazone (100 mg/kg). All values are Mean ± SD. Bars represent the standard deviation. *p < 0.01 compared to the paracetamol control group (Two-way ANOVA followed by Bonferroni post-tests to compare each column to column). PCM, Paracetamol; NAPQI, N-acetyl-p-benzoquinoneimine
Effect of chlorzoxazone on the liver function tests and histology
The effect of Chlorzoxazone on the hepatotoxicity induced by the NAPQI was analyzed by the liver functioning tests and the comparison of histological parameters of the control group (Fig. 5A) treated with paracetamol (300 mg/kg), and the combination of paracetamol with Silymarin (100 mg/kg), chlorzoxazone (50 mg/kg and 100 mg/kg). The results are presented in Table 3. Compared to the control, the group treated with oral administration of paracetamol at 300 mg/kg showed a significant increase in the Serum SGPT, SGPT, ALP, TP, and TB levels by 181.455%, 145.98%, 168.881, 116.204%, and 396.104% respectively. These changes agreed with the severe damage to the sections of rats’ livers, as shown in Fig. 5A, B. The morphological characteristics like vascular congestion, steatosis, sinusoidal dilation, and ballooning degeneration can be seen in the histological section of the rats treated with paracetamol (300 mg/kg) alone, presented in Fig. 5B. However, the administration of Silymarin (100 mg/kg) and Chlorzoxazone (50 and 100 mg/kg) in combination with paracetamol resulted in the reduction of serum SGPT, SGPT, ALP, TP, and TB levels by 142.383%, 91.1073%, 144.208%, 74.927% and 197.442 respectively resulting in attaining the typical morphology of the liver section of the rats. This protective effect of Chlorzoxazone on the hepatic cells may be due to the reduction in the formation of NAPQI by inhibiting the CYP2E1. These results of the hepatic cells can be further supported by the images shown in Fig. 5C–E, which depict only the scattered cytoplasmic vascularization. In summary, the albumin levels, which were increased with the treatment of the paracetamol alone, were back to normal as that of the control group in the presence of Chlorzoxazone.

Histopathological examination of hepatoprotective activity of Chlorzoxazone and Silymarin when administered along with Paracetamol (300 mg/kg). A (Control). B Represents the Liver Histology section of rats treated with Paracetamol; ballooning degeneration, vascular congestion, sinusoidal dilatation, Central vein (CV), and steatosis;(clear vacuoles contained lipid in life) were seen in Paracetamol treated group C, D Represents the Liver Histology section of rats treated with paracetamol and Chlorzoxazone 50 mg/kg & 100 mg/kg; E Represents the Liver Histology section of rats treated with paracetamol and silymarin 100 mg/kg. The images from C–E show a significant improvement in the hepatic markers with scattered cytoplasmic vacuolization indicating the hepatic protective property of Chlorzoxazone and Silymarin
Effect of chlorzoxazone on kidney function tests and histology
Nephrotoxicity has been identified by observing increased creatinine levels, blood urea nitrogen, and uric acid levels in the paracetamol-treated group compared to the control group (Fig. 6A and Table 4). The comparison of the histological parameters of the rat kidney sections treated with paracetamol (300 mg/kg) and the combination of paracetamol with Silymarin (100 mg/kg), chlorzoxazone (50 mg/kg, and 100 mg/kg). The results are presented in Table 4. Compared to the control group treated with oral administration of paracetamol, 300 mg/kg showed a significant increase in the Serum urea, BUN, uric acid, and uric acid levels by 134.114%, 188.435%, 62.811%, 116.204%, and 998.925% respectively. These changes agreed with the severe damage to the sections of rats' kidneys treated with paracetamol (300 mg/kg) alone, as shown in Fig. 6B resulting in morphological characteristics like numerous tubular casts, glomerular atrophy, leukocyte infiltration, and degenerated globular structure. However, the administration of Silymarin (100 mg/kg) and chlorzoxazone (50 and 100 mg/kg) resulted in the reduction of Serum urea, BUN, uric acid, and uric acid levels resulting in remarkable recovery of the renal lesions and attaining the typical morphology of the liver section of the rats. This effect of Chlorzoxazone can be termed as the protective effect on the hepatic cells may be due to the reduction in the formation of NAPQI by inhibiting the CYP2E1. These results of the hepatic cells can be further supported by the images shown in Fig. 6C–E. In summary, the serum levels which were increased with the treatment of the paracetamol alone were back to normal as that of the control group in the presence of Chlorzoxazone.

Histopathologically examined the nephroprotective activity of Silymarin and Chlorzoxazone when administered along with Paracetamol (300 mg/kg). A (Control). B Represents the Kidney Histology section of rats treated with Paracetamol; pathological changes, including glomerular atrophy, degenerated tubular structure, leukocyte infiltration, and numerous tubular casts, can be seen. C, D Represents the Kidney Histology section of rats treated with paracetamol and chlorzoxazone 50 and 100 mg/kg; E Represents the Liver Histology section of rats treated with paracetamol and silymarin 100 mg/kg. The images from C–E show a significant improvement in the kidney functioning markers (C–E) with renal lesions, which were remarkably ameliorated by treatment with Chlorzoxazone and Silymarin
Discussion
Paracetamol is one of the most used and prescribed antipyretic and analgesic drugs. It has been reported that long-term usage and paracetamol intake at unusual dosages leads to the accumulation of the toxic metabolite of paracetamol called NAPQI. NAPQI leads to liver and kidney toxicity. Paracetamol is primarily metabolized by glucuronidation and sulfate conjugation. Metabolism of the paracetamol by the CYP450 system is mainly by CYP2E1, CYP1A2, and CYP3A4, leading to NAPQI formation. Chlorzoxazone (CLZ) is a skeletal muscle relaxant and is reported to be a probe to measure CYP2E1 activity. In addition, CLZ was reported to be a CYP isoenzyme modulator. The role of Chlorzoxazone in inhibiting the formation of NAPQI via the metabolism of paracetamol is not yet explored. The current study focused on investigating the effect of Chlorzoxazone on the pharmacokinetics of paracetamol and its toxic metabolite NAPQI.
The result of this study shows that Chlorzoxazone increased the paracetamol Cmax by 1.25-fold when pretreated with Silymarin (100 mg/kg), 1.6-fold when pretreated with CLZ (50 mg/kg), and ~ 2-fold increased with 100 mg/kg of CLZ. Similarly, AUC0–∞ of paracetamol has increased 1.5 and 1.4-fold when pre-treated with Silymarin (100 mg/kg) and CLZ (50 mg/kg and 100 mg/kg). This change in the bioavailability might be due to the inhibition of CYP2E1 and CYP3A4 enzymes. In addition, chlorzoxazone decreased the Cmax of NAPQI by 0.8-fold when pretreated with Silymarin (100 mg/kg), 0.6-fold when pretreated with CLZ (50 mg/kg and 100 mg/kg). Similarly, AUC0–∞ of NAPQI decreased 0.75-fold when pretreated with CLZ (100 mg/kg). This decrease in the pharmacokinetic parameters of NAPQI might be due to the inhibition of CYP2E1 and CYP3A4 enzymes. Also, the histopathological evaluation of liver and kidney sections of the paracetamol-treated rats with and without CLZ and Silymarin shows that the combination treatment ameliorated the severe damage caused by NAPQI. These findings of this study are consistent with the previous findings.
Acarbose is a complex oligosaccharide that inhibits pancreatic alpha-amylase and is used in the treatment of type 2 diabetes mellitus. It was reported that acarbose, combined with paracetamol, leads to the formation of a toxic metabolite of paracetamol in vitro and in vivo. The toxicity is attributed to acarbose's ability to induce the hepatic isoenzyme CYP2E1, which is responsible for forming paracetamol reactive, toxic metabolite. Based on these findings, patients were recommended to avoid the combination of acarbose, acetaminophen, and Ethanol until further investigation of the clinical significance of the potential interactions [43]. This report indicates that CYP2E1 plays a role in the paracetamol metabolism in forming a toxic metabolite.
A similar study on the metabolism of paracetamol in combination with barbiturates including Amobarbital, Secobarbital, Ergotamine Methohexital, Primidone, Mephobarbital, Thiopental could result in the decrease in the effectiveness of acetaminophen by increasing the metabolism of paracetamol. In contrast, barbiturates overdosing in combination with paracetamol enhances toxicity due to the formation of acetaminophen metabolites [44, 45]. In addition, CYP3A4 metabolizes 10–15% of acetaminophen. To further emphasize this, paracetamol studies conducted in the presence of Aprepitant, a partial CYP3A4 inhibitor and inducer, increase the plasma concentrations of acetaminophen. The study also reported that a 5-day Aprepitant regimen resulted in the AUC increase of midazolam, a CYP3A4 substrate, by 2.3-fold on the day and 3.3-fold on day 5. In addition to this, followed by a 3-day oral regimen of Aprepitant, the AUC of midazolam administered on days 1,4,8 and 15 improved by 25% on day 4 and lowered by 19% and 4%, respectively on days 8 and 15 [4]. This finding shows that the CYP3A4 inhibitors lead to changes in the bioavailability of acetaminophen, which was observed in the current study.
A series of studies conducted on paracetamol in combination with antivirals demonstrated a better understanding of acetaminophen metabolism by CYP3A4 isoenzyme, a partial metabolizer of acetaminophen. The presence of boceprevir and paracetamol co-administration resulted in the elevated acetaminophen plasma concentration via the inhibition of CYP3A4 by boceprevir [4]. Similarly, the combination prescription for the treatment of hepatitis (Dasabuvir; Ombitasvir; Paritaprevir; Ritonavir) along with the concurrent administration of paracetamol resulted in the elevation of plasma concentration of acetaminophen and subsequent increase in the adverse effects caused by the acetaminophen toxic metabolite. It may be due to the inhibition of the CYP3A4 isoenzyme by ritonavir which is reported to be an inhibitor of CYP3A4 (Tolman et al. 1998; [4].
It is noteworthy that the administration of paracetamol in combination with saquinavir, a CYP3A4 inhibitor [30], could increase the plasma concentration of acetaminophen like ritonavir, as reported above. It is interesting to test the outcome of food-drug interactions of acetaminophen with pomegranate juice since pomegranate juice is reported to be an inhibitor of CYP3A4 in single-dose studies and an inducer in multiple-dose studies [30]. To add to this Carbamazepine, Oxcarbazepine which is prescribed to treat epilepsy, pain, and bipolar disorders, is reported to induce the hepatic metabolism of acetaminophen resulting in the hepatotoxicity of acetaminophen due to the formation of the toxic metabolite NAPQI. Similarly higher metabolism of acetaminophen could alter its effect of acetaminophen [44, 46].
Similarly, the role of CYP3A4 in acetaminophen metabolism was further emphasized by co-administration of acetaminophen with Posaconazole, a potent CYP3A4 inhibitor. The study revealed that the presence of Posaconazole resulted in increased acetaminophen concentration and increased risk of adverse effects related to the acetaminophen toxic metabolite [47]. Further reports of Isavuconazonium administered with paracetamol revealed an increased serum concentration of paracetamol due to the inhibition of CYP3A4 by the isavuconazole, the active moiety of isavuconazonium [4]. Finally, Mitotane, an inducer of CYP3A4, when administered with acetaminophen, resulted in the decrease of plasma concentration of acetaminophen [4, 48] The above reports show that co-administration of paracetamol with various drugs that are substrates of CYP3A4 resulted in either inhibition of CYP3A4 or increasing the plasma concentration of acetaminophen leading to the adverse effects caused by the toxic metabolite NAPQI. Similarly, inducing the CYP3A4 decreased the acetaminophen plasma concentration, leading to a decrease in the impact of paracetamol. In this study, we have observed an increase in the plasma concentration of paracetamol which supports that this change might be due to the inhibition of CYP3A4 by Chlorzoxazone.
CYP2E1 is reported to be an enzyme responsible for the metabolism of 5–10% of acetaminophen, which also results in the formation of NAPQI. The subsequent studies reported earlier have demonstrated the role of various drug molecules that are substrates of CYP2E1 and how they affect the metabolism of acetaminophen and the formation of NAPQI. The following molecules, Efavirenz, Emtricitabine, and Tenofovir, induce the hepatic isoenzymes CYP2E1 and CYP1A2. The study conducted in the presence of efavirenz increased NAPQI, a hepatotoxic metabolite, due to inducing CYP2E1 by Efavirenz and resulted in the decrease of analgesic activity of acetaminophen [44]. Another study reported that acute or chronic consumption of Ethanol leads to an increased risk of hepatotoxic metabolite formation due to inducing CYP2E1 by Ethanol. It is noteworthy to consider that chronic alcohol consumption depletes the glutathione stores in the liver, and administration of acetaminophen could potentially increase the risk of liver damage due to NAPQI formation. Limited use of acetaminophen should be considered in patients who consume alcohol [49,50,51,52].
Similarly, anticonvulsants, including Hydantoin, were reported to be effective inducers of hepatic microsomal enzymes that increase the metabolism of several drugs. This leads to the reduced efficacy of the drugs with an increased risk of toxic metabolite formation in the case of medications like acetaminophen. Previous clinical trials on acetaminophen (1300 mg and 6200 mg daily) along with phenytoin led to acetaminophen-related hepatotoxicity, and interestingly, cessation of acetaminophen for 2 weeks led to normal levels of serum transaminase. So, adhering to the dosing limitation of acetaminophen and phenytoin was recommended since the risk of hepatotoxicity from acetaminophen may be increased [53]. Another paracetamol combination study with Isoniazid, Pyrazinamide, PZA; Rifampin, and Rifabutin which are CYP2E1 inducers, led to an increased risk of acetaminophen-induced hepatotoxicity due to increased metabolism showing a more significant percentage of acetaminophen hepatotoxic metabolites. To further support this, a patient's observation of severe hepatotoxicity was administered with a combination of isoniazid, INH, and acetaminophen. A similar observation was also noted in animal studies in a combination of isoniazid, INH, and acetaminophen; [54]. Rifampin, in combination with acetaminophen, was reported to increase acetaminophen's hepatotoxic metabolites significantly due to the CYP2E1-induced activity of Rifampin [55].
Glucuronidation and sulfate conjugation also plays a primary role in acetaminophen metabolism and, minorly, by CYP1A2. A study reported that Osimertinib in combination with acetaminophen could lead to decreased efficacy of acetaminophen due to CYP1A2-induced higher metabolism [4]. Another CYP1A2 inducer might also theoretically induce the acetaminophen metabolism resulting in the increased risk of acetaminophen-induced hepatotoxicity via the formation of NAPQI [56]. Another report with Sulfinpyrazone is responsible for inducing hepatic oxidative microsomal enzymes. Sulfinpyrazone was also reported to increase acetaminophen clearance by roughly 23%. These properties of Sulfinpyrazone may increase the risk of hepatotoxicity due to the formation of toxic metabolites via the rapid metabolism of acetaminophen by Sulfinpyrazone, which is not yet confirmed [44].
Acetaminophen metabolizing was reported to be altered in the case of smoking. It was reported that smoking induces the CYP1A2 enzymes supporting the fact that smoking could potentially increase the risk of hepatotoxicity by acetaminophen toxic metabolite NAPQI due to overdosing. One study reported that tobacco smoking was persistent in patients with acetaminophen poisoning. Smoking is also an independent risk factor for hepatotoxicity resulting in liver failure and death in some cases due to overdosing on acetaminophen [57]. Finally, Vemurafenib is reported to be an inhibitor of CYP1A2 and CYP2A6 and an inducer of CYP3A4. It was reported that the combination of acetaminophen with Vemurafenib alters the pharmacokinetics of acetaminophen [4].
The above reports show that co-administration of paracetamol with various drugs that are substrates of CYP2E1 resulted in inducing CYP2E1, increasing the plasma concentration of acetaminophen leading to the adverse effects caused by the toxic metabolite NAPQI. Similarly, inducing the CYP2E1 lead to a decrease in the plasma concentration of the acetaminophen leading to a decrease in the effect of paracetamol. In this study, we have observed the reduction in the plasma concentration of NAPQI, which supports that this change might be due to the inhibition of CYP2E1 by Chlorzoxazone.
Conclusion
The result of this study clearly showed that chlorzoxazone enhanced paracetamol absorption significantly with a simultaneous decrease in the formation of NAPQI might be due to the inhibition of the CYP2E1 by chlorzoxazone. Interestingly the toxicity induced by the NAPQI has been ameliorated and reversed to the normal condition when pretreated with chlorzoxazone. The combination could be an alternative approach to reduce the paracetamol dosage and still achieve the therapeutic index.
Availability of data and materials
Data and material can be provided upon request.
Abbreviations
- P-gp:
-
P-glycoprotein
- CYP:
-
Cytochrome P450
- NAPQI:
-
N-Acetyl-p-benzoquinoneimine
- CYP2E1:
-
Cytochrome P450 2E1
- RP-HPLC:
-
Reverse Phase-High Performance Liquid Chromatography
- CLZ:
-
Chlorzoxazone
- SCMC:
-
Sodium Carboxymethyl Cellulose
- Cmax :
-
Concentration of maximum plasma
- Tmax :
-
Time to reach the maximum plasma concentrations
- AUC:
-
Area Under the concentration–time curve of plasma
- AUC0–t :
-
AUC from zero to the last sampling time
- AUC0–α :
-
AUC from time zero to infinite
- t1/2:
-
Terminal half-life
- CL/F:
-
Clearance
- Vz/F:
-
Apparent volume of distribution
- Vss:
-
Apparent volume of distribution at steady state
- MRT:
-
Mean residence time
- SGPT:
-
Serum Glutamic Pyruvic Transaminase
- SGOT:
-
Serum Glutamic-oxaloacetic Transaminase
- ALP:
-
Alkaline phosphatase
- BUN:
-
Blood urea nitrogen
References
Jóźwiak-Bebenista M, Nowak JZ (2014) Paracetamol: mechanism of action, applications and safety concern. Acta Pol Pharm 71:11–23
Graham GG, Davies MJ, Day RO, Mohamudally A, Scott KF (2013) The modern pharmacology of paracetamol: therapeutic actions, mechanism of action, metabolism, toxicity and recent pharmacological findings. Inflammopharmacology 21:201–232
Heubi JE, Barbacci MB, Zimmerman HJ (1998) Therapeutic misadventures with acetaminophen: hepatoxicity after multiple doses in children. J Pediatr 132:22–27
Manyike PT, Kharasch ED, Kalhorn TF, Slattery JT (2000) Contribution of CYP2E1 and CYP3A to acetaminophen reactive metabolite formation. Clin Pharmacol Ther 67:275–282
Jing Y, Wu K, Liu J, Ai Q, Ge P, Dai J, Jiang R, Zhou D, Che Q, Wan J (2015) Aminotriazole alleviates acetaminophen poisoning via downregulating P450 2E1 and suppressing inflammation. PLoS ONE 10:e0122781
Tomishima Y, Ishitsuka Y, Matsunaga N, Nagatome M, Furusho H, Irikura M, Ohdo S, Irie T (2013) Ozagrel hydrochloride, a selective thromboxane A2 synthase inhibitor, alleviates liver injury induced by acetaminophen overdose in mice. BMC Gastroenterol 13:1–10
Ying W, Yan-Ling W, Li-Hua L, Ji-Xing N (2012) Protective effect of Ornithogalum saundersiae Ait (Liliaceae) against acetaminophen-induced acute liver injury via CYP2E1 and HIF-1α. Chin J Nat Med 10:177–184
Zhao X, Cong X, Zheng L, Xu L, Yin L, Peng J (2012) Dioscin, a natural steroid saponin, shows remarkable protective effect against acetaminophen-induced liver damage in vitro and in vivo. Toxicol Lett 214:69–80
Kumari A, Kakkar P (2012) Lupeol prevents acetaminophen-induced in vivo hepatotoxicity by altering the Bax/Bcl-2 and oxidative stress-mediated mitochondrial signaling cascade. Life Sci 90:561–570
Kwak MK, Kim SG, Kwak JY, Novak RF, Kim ND (1994) Inhibition of cytochrome P4502E1 expression by organosulfur compounds allylsulfide, allylmercaptan and allylmethylsulfide in rats. Biochem Pharmacol 47:531–539
Oliveira FA, Chaves MH, Almeida FR, Lima RC Jr, Silva RM, Maia JL, Brito GAA, Santos FA, Rao VS (2005) Protective effect of α-and β-amyrin, a triterpene mixture from Protium heptaphyllum (Aubl.) March. trunk wood resin, against acetaminophen-induced liver injury in mice. J Ethnopharmacol 98:103–108
Su GL, Gong KQ, Fan MH, Kelley WM, Hsieh J, Sun JM, Hemmila MR, Arbabi S, Remick DG, Wang SC (2005) Lipopolysaccharide-binding protein modulates acetaminophen-induced liver injury in mice. Hepatology 41:187–195
Bayan MF, Jaradat A, Alyami MH, Naser AY (2023) Smart Pellets for Controlled Delivery of 5-Fluorouracil. Molecules 28:306
Jang S, Kim H, Hwang K, Jekal S, Pae H, Choi B, Yun Y, Kwon T, Chung H, Kim Y (2003) Hepatoprotective effect of baicalin, a major flavone from Scutellaria radix, on acetaminophen-induced liver injury in mice. Immunopharmacol Immunotoxicol 25:585–594
Bayan MF, Marji SM, Salem MS, Begum MY, Chidambaram K, Chandrasekaran B (2022) Development of polymeric-based formulation as potential smart colonic drug delivery system. Polymers 14:3697
Janbaz K, Gilani A (2000) Studies on preventive and curative effects of berberine on chemical-induced hepatotoxicity in rodents. Fitoterapia 71:25–33
Thomsen MS, Loft S, Roberts DW, Poulsen HE (1995) Cytochrome P4502E1 inhibition by propylene glycol prevents acetaminophen (paracetamol) hepatotoxicity in mice without cytochrome P4501A2 inhibition. Pharmacol Toxicol 76:395–399
Qiu-Ju L, Bessems JG, Commandeur JN, Adams B, Vermeulen NP (1994) Mechanism of protection of ebselen against paracetamol-induced toxicity in rat hepatocytes. Biochem Pharmacol 48:1631–1640
Lin MC, Wang EJ, Patten C, Lee MJ, Xiao F, Reuhl KR, Yang CS (1996) Protective effect of diallyl sulfone against acetaminophen-induced hepatotoxicity in mice. J Biochem Toxicol 11:11–20
Hong SW, Lee HS, Jung KH, Lee H, Hong SS (2012) Protective effect of fucoidan against acetaminophen-induced liver injury. Arch Pharmacal Res 35:1099–1105
Fan YJ, Rong Y, Li PF, Dong WI, Zhang DY, Zhang L, Cui MJ (2013) Genistein protection against acetaminophen-induced liver injury via its potential impact on the activation of UDP-glucuronosyltransferase and antioxidant enzymes. Food Chem Toxicol 55:172–181
Khemawoot P, Nishino K, Ishizaki J, Yokogawa K, Miyamoto KI (2007) Circadian rhythm of cytochrome P4502E1 and its effect on disposition kinetics of chlorzoxazone in rats. Eur J Pharmacol 574:71–76
Lucas D, Ferrara R, Gonzalez E, Bodenez P, Albores A, Manno M, Berthou F (1999) Chlorzoxazone, a selective probe for phenotyping CYP2E1 in humans. Pharmacogenetics 9:377–388
Pingili R, Vemulapalli S, Mullapudi SS, Nuthakki S, Pendyala S, Kilaru N (2016) Pharmacokinetic interaction study between flavanones (hesperetin, naringenin) and rasagiline mesylate in wistar rats. Drug Dev Ind Pharm 42:1110–1117
Sridhar V, Surya SM, Ravindra BP, Naveen BK (2014) Evaluation of first-pass cytochrome P4503A (CYP3A) and P-glycoprotein activities using felodipine and hesperetin in combination in Wistar rats and everted rat gut sacs in vitro. Phytother Res 28:699–705
Surya SM, Sridhar V, Puneeth Y, Ravindra BP, Naveen BK (2014) Enhanced oral bioavailability of felodipine by naringenin in Wistar rats and inhibition of P-glycoprotein in everted rat gut sacs in vitro. Drug Dev Ind Pharm 40:1371–1377
Challa VR, Ravindra BP, Challa SR, Johnson B, Maheswari C (2013) Pharmacokinetic interaction study between quercetin and valsartan in rats and in vitro models. Drug Dev Ind Pharm 39:865–872
Pingili RB, Pawar AK, Challa SR (2015) Systemic exposure of Paracetamol (acetaminophen) was enhanced by quercetin and chrysin co-administration in Wistar rats and in vitro model: risk of liver toxicity. Drug Dev Ind Pharm 41:1793–1800
Pingili RB, Vemulapalli S, Dirisala VR, Mullapudi SS, Gullapalli Y, Kilaru NB (2021) Effect of naringenin on the pharmacokinetics of metoprolol succinate in rats. Xenobiotica 51:926–932
Vemulapalli S (2016) Influence of pomegranate juice on the CYP3A4-mediated metabolism and p-glycoprotein mediated transport of saquinavir in vivo and ex vivo models. Indones J Pharm 27:152
Ahn CY, Bae SK, Jung YS, Lee I, Kim YC, Lee MG, Shin WG (2008) Pharmacokinetic parameters of chlorzoxazone and its main metabolite, 6-hydroxychlorzoxazone, after intravenous and oral administration of chlorzoxazone to liver cirrhotic rats with diabetes mellitus. Drug Metab Dispos 36:1233–1241
Wan J, Shoaf SE, Ernstgard E, Song BJ (2006) Chlorzoxazone metabolism is increased in fasted Sprague-Dawley rats. J Pharm Pharmacol 58:51–61
Mahli A, Koch A, Czech B, Peterburs P, Lechner A, Haunschild J, Müller M, Hellerbrand C (2015) Hepatoprotective effect of oral application of a silymarin extract in carbon tetrachloride-induced hepatotoxicity in rats. Clin Phytosci 1:1–8
Zhang W, Hong R, Tian T (2013) Silymarin’s protective effects and possible mechanisms on alcoholic fatty liver for rats. Biomol Ther 21:264
Bui K, She F, Zhou D, Butler K, Al-Huniti N, Sostek M (2016) The effect of quinidine, a strong P-glycoprotein inhibitor, on the pharmacokinetics and central nervous system distribution of naloxegol. J Clin Pharmacol 56:497–505
Flores-Pérez C, Chávez-Pacheco JL, Ramírez-Mendiola B, Alemón-Medina R, García-Álvarez R, Juárez-Olguín H, Flores-Pérez J (2011) A reliable method of liquid chromatography for the quantification of acetaminophen and identification of its toxic metabolite N-acetyl-p-benzoquinoneimine for application in pediatric studies. Biomed Chromatogr 25:760–766
Powis G, Svingen BA, Dahlin DC, Nelson SD (1984) Enzymatic and non-enzymatic reduction of N-acetyl-p-benzoquinone imine and some properties of the N-acetyl-p-benzosemiquinone imine radical. Biochem Pharmacol 33:2367–2370
Schumann G, Bonora R, Ceriotti F, Clerc-Renaud P, Ferrero CA, Férard G, Franck PF, Gella FJ, Hoelzel W, Jørgensen PJ, Kanno T, Kessne A, Klauker R, Kristiansen N, Lessinger JM, Linsinger TP, Misaki H, Panteghini M, Pauwels J, Schimmel HG, Vialle A, Weidemann G, Siekmann L (2002) IFCC primary reference procedures for the measurement of catalytic activity concentrations of enzymes at 37 degrees C. Part 2. Reference procedure for the measurement of catalytic concentration of creatine kinase. Clin Chem Lab Med 40:635–642
Young DS, Pestaner L, Gibberman V (1975) Effects of drugs on clinical laboratory tests. Clin Chem 21:1D-432D
Gornall AG, Bardawill CJ, David MM (1949) Determination of serum proteins by means of the biuret reaction. J Biol Chem 177:751–766
Bablok W, Passing H, Bender R, Schneider B (1988) A general regression procedure for method transformation. Application of linear regression procedures for method comparison studies in clinical chemistry, part III. J Clin Chem Clin Biochem 26:783–790
Sobeh M, Esmat A, Petruk G, Abdelfattah MAO, Dmirieh M, Monti DM, Abdel-Naim AB, Wink M (2018) Phenolic compounds from Syzygium jambos (Myrtaceae) exhibit distinct antioxidant and hepatoprotective activities in vivo. J Funct Foods 41:223–231
Wang PY, Kaneko T, Wang Y, Sato A (1999) Acarbose alone or in combination with ethanol potentiates the hepatotoxicity of carbon tetrachloride and acetaminophen in rats. Hepatology 29:161–165
Bailey DN (1997) Relative binding of acetaminophen, lidocaine, phenobarbital, phenytoin, quinidine, and theophylline to human tissues in vitro. J Anal Toxicol 21:1–4
Pond SM, Tong TG, Kaysen GA, Menke DJ, Galinsky RE, Roberts SM, Levy G (1982) Massive intoxication with acetaminophen and propoxyphene: unexpected survival and unusual pharmacokinetics of acetaminophen. J Toxicol Clin Toxicol 19:1–16
Smith JA, Hine ID, Beck P, Routledge PA (1986) Paracetamol toxicity: is enzyme induction important? Hum Toxicol 5:383–385
Sansone-Parsons A, Krishna G, Simon J, Soni P, Kantesaria B, Herron J, Stoltz R (2007) Effects of age, gender, and race/ethnicity on the pharmacokinetics of posaconazole in healthy volunteers. Antimicrob Agents Chemother 51:495–502
Guengerich FP (2021) A history of the roles of cytochrome P450 enzymes in the toxicity of drugs. Toxicol Res 37:1–23
Florén CH, Thesleff P, Nilsson A (1987) Severe liver damage caused by therapeutic doses of acetaminophen. Acta Med Scand 222:285–288
Thummel KE, Slattery JT, Nelson SD, Lee CA, Pearson PG (1989) Effect of ethanol on hepatotoxicity of acetaminophen in mice and on reactive metabolite formation by mouse and human liver microsomes. Toxicol Appl Pharmacol 100:391–397
Whitcomb DC, Block GD (1994) Association of acetaminophen hepatotoxicity with fasting and ethanol use. JAMA 272:1845–1850
Zimmerman HJ, Maddrey WC (1995) Acetaminophen (paracetamol) hepatotoxicity with regular intake of alcohol: analysis of instances of therapeutic misadventure. Hepatology 22:767–773
Brackett CC, Bloch JD (2000) Phenytoin as a possible cause of acetaminophen hepatotoxicity: case report and review of the literature. Pharmacotherapy 20:229–233
O’Shea D, Kim RB, Wilkinson GR (1997) Modulation of CYP2EI activity by isoniazid in rapid and slow N-acetylators. Br J Clin Pharmacol 43:99–103
Paracetamol interaction, reactions weekly, 2001;853:10.
Henderson NC, Pollock KJ, Frew J, Mackinnon AC, Flavell RA, Davis RJ, Sethi T, Simpson KJ (2007) Critical role of c-jun (NH2) terminal kinase in paracetamol-induced acute liver failure. Gut 56:982–990
Schmidt LE, Dalhoff K (2003) The impact of current tobacco use on the outcome of paracetamol poisoning. Aliment Pharmacol Ther 18:979–985
Acknowledgements
We are very grateful to the management of SVKM’s NMIMS Deemed to be University and KVSR Siddhartha College of Pharmaceutical Sciences, Vijayawada, for providing the necessary facilities and their encouragement in completing this work.
Funding
Not received any funding for this work.
Author information
Authors and Affiliations
Contributions
Dr. NBK and Dr. RBP designed the work and guided the students. Mr. SV, Mr. MVG, Miss. DP, Mr. RK and Miss. VR were involved in animal studies and drafted the rough manuscript. Dr. NBK and Dr. RBP analyzed the data and finalized the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The protocol was approved by the IAEC at KVSR Siddhartha College of Pharmaceutical Sciences (Regd. No: 993/PO/Re/S/06/CPCSEA). The protocol number was KVSRSCOPS/11-03-14-006.
Consent for publication
All authors provided their consent for publication in FJPS.
Competing interests
The authors declare that there is no conflict of interest with anyone or any institute.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pingili, R.B., Vemulapalli, S., Gadamsetty, M.V.V.N. et al. Chlorzoxazone reduced the paracetamol-induced toxicity via competitive inhibition of CYP2E1-mediated metabolism. Futur J Pharm Sci 9, 34 (2023). https://doi.org/10.1186/s43094-023-00484-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43094-023-00484-2