
Abstract
Background
A plethora of chemicals exists in human body which can alter physiology in one way or other. Scientists have always been astounded by such abilities of chemicals but as the technology advances, even the chemical which was once expected to be well known changes its status to not really well known. Adenosine is one of the chemicals which is in consonance with the aforementioned statements, although previous articles have covered vast information on role of adenosine in cardiovascular physiology, bacterial pathophysiology and inflammatory diseases. In this review we have discussed adenosine and its congeners as potential promising agents in the treatment of Huntington’s disease, post-traumatic stress disorder, erectile dysfunction, viral infections (SARS-CoV) and anxiety.
Main text
Adenosine is a unique metabolite of ATP; which serves in signalling as well. It is made up of adenine (a nitrogenous base) and ribo-furanose (pentose) sugar linked by β-N9-glycosidic bond. Adenosine on two successive phosphorylation forms ATP (Adenosine Triphosphate) which is involved in several active processes of cell. It is also one of the building blocks (nucleotides) involved in DNA (Deoxy-ribonucleic Acid) and RNA (Ribonucleic Acid) synthesis. It is also a component of an enzyme called S-adenosyl-L-methionine (SAM) and cyano-cobalamin (vitamin B-12). Adenosine acts by binding to G protein-coupled receptor (GPCR: A1, A2A, A2B and A3) carries out various responses some of which are anti-platelet function, hyperaemic response, bone remodelling, involvement in penile erection and suppression of inflammation. On the other hand, certain microorganisms belonging to genus Candida, Staphylococcus and Bacillus utilize adenosine in order to escape host immune response (phagocytic clearance). These microbes evade host immune response by synthesizing and releasing adenosine (with the help of an enzyme: adenosine synthase-A), at the site of infection.
Conclusion
With the recent advancement in attribution of adenosine in physiology and pathological states, adenosine and its congeners are being looked forward to bringing a revolution in treatment of inflammation, viral infections, psychiatric and neurodegenerative disorders.
Similar content being viewed by others


Background
A plethora of chemical exists which can modify human physiology in multiple ways. Scientists have always been astounded by the way in which the biochemicals modify these physiology. However, with the advent of new technologies, as more and more knowledge, even the chemical which was expected to be well known often changed its status to not really well known.
This paper is about one such biochemical: adenosine. Adenosine is a metabolite, a neurotransmitter, a signalling agent which was once known to modify only cardiovascular physiology but today, it has been found to be multifaceted chemical which can alter physiology in innumerable ways. Adenosine and its congers today have served as a prototype which on more studies are expected to turn out as promising agent in treatment of several ailments and diseases.
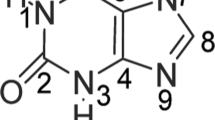
Adenosine is one of the life sustaining chemical moieties present in cell [1]. Adenosine has nitrogenous base: Adenine, which is linked to ribose sugar (ribo-furanose, a five carbon containing sugar) via β-N9-glycosidic linkage. Adenosine is one of the essential nucleotides required in biosynthesis and duplication/replication of DNA and RNA [2,3,4,5,6]. ATP, the energy currency of cell, is formed from adenosine after series of steps. Hence, a majority of active process in cell will retard in the absence of adenosine making it an indispensable chemical moiety in cell [7, 8].
Apart from all these functions, adenosine is also a component of an enzyme called S-adenosyl-L-methionine (SAM) and cyano-cobalamin (vitamin B-12) (Fig. 1).

Structure of adenosine
Main text
Metabolism of adenosine
External or extracellular metabolism
-
Adenosine deaminase enzyme is responsible for biotransformation of adenosine to inosine.
-
Extracellular activity of adenosine is also brought to an end by ENT (Equilibrative Nucleoside Transporters). ENTs are responsible for intracellular influx/transport of adenosine
Internal or intracellular/cytosolic metabolism
-
Adenosine deaminase: converts adenosine to inosine.
-
S-adenosyl-homocysteine hydrolase (SAHH): converts adenosine to adenosyl homocysteine
-
Adenosine kinase: converts adenosine to adenosine monophosphate by phosphorylation. This phosphorylation maintains cytosolic concentration of adenine nucleosides/nucleotides.
During cellular injury or hypoxia/ischemia, ATP is broken down to ADP by CD-39 [9]. ADP is further broken down into adenosine using CD-73. Adenosine binds to its GPCR and performs physiological–pathological actions. Adenosine is carried inside cell using transmembrane protein called equilibrative nucleoside transporters (ENTs). Adenosine is biotransformed either into inosine or S-(5′-Adenosyl)-L-homocysteine (AdoHcy) using adenosine deaminase (ADA) and S-adenosyl-L-homocysteine hydrolase (SAHH), respectively. ATP formed inside cell can migrate out of cell using connexin [10,11,12,13,14,15,16,17,18].
How adenosine acts? (receptors and traducer pathways)
Adenosine acts by binding to metabotropic G protein-coupled receptors (GPCR). It activates both Gs and Gi subtypes of GPCR. A detailed explanation is given in Table 1.
ATP or adenosine triphosphate is stored inside the vesicle in presynaptic neuron. During action potential, vesicle gets fuse with presynaptic membrane of presynaptic neuron and glutamate and ATP are released. ATP is converted to adenosine by ectonucleotidase (EctoN). The released adenosine can bind to presynaptic A2A and A1 inhibitory receptor or may bind to excitatory A2A post-synaptic receptor. Adenosine is taken up by equilibrative nucleoside transporters (ENT) inside cell where it is phosphorylated by kinases to ADP and ATP. A2A adenosine receptors on blood vessels exert vasodilatory effect [19,20,21,22,23,24,25,26,27].
Pharmacological and pathological roles of adenosine
Adenosine in hyperaemic response
Myocardium of human heart is supplied oxygen by coronary micro-circulation. In response to hypoxia/ischemia, coronary perfusion multiplies (almost 5 times the base value): a phenomenon known as hyperaemic response. Adenosine is also one of the factors which are involved in hyperaemic response because of its ability to cause vasodilation in coronary microvasculature. Cytosolic level of adenosine increases at the time of ischemia since there is a misalliance between its use and ATP synthesis (in the absence of oxygen; synthesis of ATP is retarded) [28, 29].
Adenosine in bone remodelling
Adenosine plays a significant role in bone reabsorption and remodelling. By activating A1 receptor, development of osteoclast from monocytic precursor is augmented. Activation of A2 receptor on the contrary inhibits differentiation of osteoclast in bones [30,31,32,33,34,35].
Adenosine as anti-platelet agent
Adenosine and one of its analogues 2-chloro adenosine have been indicated as anti-platelet agents. They act by activating two subtypes of adenosine receptor, A2A and A2B. This agonism results in increased levels of cAMP inside thrombocytes/platelets resulting in anti-platelet activity.
Although standard anti-platelet regimen includes a combination therapy with at least two anti-platelet drugs (e.g. aspirin and clopidogrel) yet patients (especially of type II Diabetes Mellitus) express resistance to these drugs after a course of time. Adenosine receptor agonist has shown an ability to curb this resistance [36,37,38]
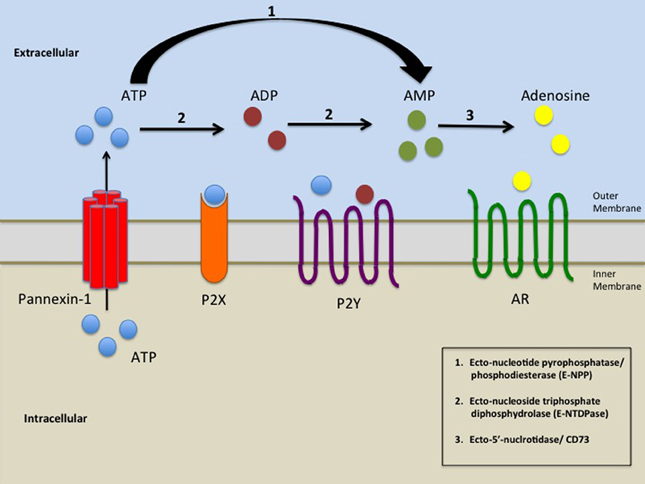
As shown in Fig. 2, ATP (Adenosine Triphosphate) breaks down to AMP (Adenosine Monophosphate) and then to adenosine by CD-39 and CD-73, respectively. Adenosine so formed either binds to its receptor and exerts it physiological/pathological action or is converted to inosine using Adenosine-de-aminase (ADA). Adenosine migrates inside the cell using ENT (Equilibrative nucleoside transporter). Inside the cell, adenosine is serially phosphorylated to form ATP which migrates outside the cell using connexin (a transmembrane protein in cell membrane) [39, 40] (Fig. 3).

Catabolism of ATP and formation of adenosine

Interaction of adenosine with its receptor in astrocytes and blood vessels
Figure 3 concerns the role of glial cells in controlling glutaminergic neuronal excitation and modulating neuronal blood flow, which are mediated by adenosine. Astrocytes are star-shaped cells (glial cells) found in brain, with typical neuron-to-glial cell ratio of 1:1. Main function of astrocytes is to clear synaptic neurotransmitter such as GABA and glutamate. It also regulates blood flow on neuronal activation. ATP is stored in presynaptic vesicles with glutamine. They both are released, concurrently, by glutaminergic neurons in response to action potential. As a matter of fact, adenosine appears in synaptic cleft either as metabolic product of adenosine triphosphate (attributed to EctoN or ectonucleotidases) or it is released by astrocytes itself (using ENT or Equilibrative Nucleoside Transporter), in response to ischemia. Adenosine can bind to both pre- and post-synaptic A1R, where it can reduce firing in presynaptic glutaminergic neuron and reduce responsiveness to glutamine in post-synaptic neuron. This property is being explored for developing new anti-epileptic agent. Adenosine can also bind to A2R and can cause vasodilation in response to ischemia and surged neural perfusion needs in response to neuronal activation. This property is being explored to devise pharmacological agents, which can control neurodegenerative disease, here IPSP: Inhibitory Post-Synaptic Potential and EPSP: Excitatory Post-Synaptic Potential [41,42,43].
Adenosine as anti-inflammatory agent
By activating A2(A) receptors, adenosine shifts the macrophage function from inflammatory factors production (TNF-alpha and IL-10) to anti-inflammatory factor production (VEGF and IL-10). During inflammation, neutrophils adhere to vascular endothelium and then migrate to site of inflammation under influence of chemicals (a phenomena known as chemotaxis or chemo kinesis). After this, they attack pathogens by phagocytosis and by generating reactive oxygen species (ROS)/oxygen radicals. Adenosine by interacting with A2A receptor can potentially retard the above-mentioned events thereby mitigating the inflammation. Adenosine derivative, S-adenosyl methionine, has been indicated as one of the mediators in therapeutic cascade which is modulated methotrexate especially when used in the treatment of rheumatoid arthritis disease. This further justifies the potential that adenosine and its congeners may have in treatment of inflammatory diseases [44,45,46,47,48,49,50,51] (Fig. 4).

Adenosine mediated inhibition of lymphotoxin and polyamine formation by methotrexate
As depicted in Fig. 4, first, methotrexate polyglutamate is formed from methotrexate. This event is followed by inhibition of enzyme dihydro-folate reductase. As the cascade progresses, the level of 5-methyl tetrahydro-folic acid decreases leading to reduced conversion of homocysteine to S-adenosyl methionine. This ultimately reduces the levels of lymphotoxin (a mediator indicated in rheumatoid arthritis disease) [52].
Adenosine in microbial pathogenesis
In order to survive inside the host by evading its immune system, a plethora of microbes utilize adenosine. This is prominent especially in the case of certain gram-positive microorganisms like Enterococcus faecalis, Bacillus anthracis, Staphylococcus aureus and Staphylococcus epidermidis. These microorganisms utilize an extracellular 5’-nucleotidase enzyme called adenosine synthase-A (AdsA) and with its help, these microbes convert adenosine monophosphate (AMP) to Adenosine. It is suggested that adenosine so formed (after binding to A2A receptor) leads to inactivation of multiple protective responses which arises on the part of host’s immune system which includes (but is not limited to) delayed activation of neutrophil and/or macrophages, arrested degranulation of neutrophils, suppression of diapedesis, arrested synthesis of TNF- α and Interleukin-12 in white blood cells [53,54,55,56,57,58,59].
Adenosine as pain reliever
Recent advances in research have attracted the attention of scientists towards adenosine and its agonist as potential antinociceptive agent. Adenosine A1 receptors are expressed in pain sensitive (nociceptive) neurons of spinal cord which are targets of such drugs. But because of short-lived lower back pain and head ache (as common side effects) along with limited clinical efficacy, adenosine and adenosine receptor agonists have not gain any edge over conventional analgesics clinically [60].
Adenosine in penile erection
Adenosine is also associated in erection of penis. This is achieved by relaxing a spongy tissue present in penis known as corpus cavernosum. It is worth to note that erectile dysfunction (ED) is attributed to compromised adenosine signalling. On the contrary, excess of adenosine activity in penis is often associated with a prolonged and painful erection of penis, a condition known as priapism [61,62,63,64,65].
Adenosine receptor agonist in medical practice
A drug named Regadenoson (A2 receptor agonist) has been approved for clinical use by USFDA & EMA (in OCT-2008 USFDA and SEP-2010 by EMA). This drug is used for testing functioning of myocardium (myocardial function testing) because of its ability to cause hyperaemia. Regadenoson has also been approved for myocardial perfusion imaging. Adenosine is also used as an anti-arrhythmic drug. It has been found as life-saving drug when cardioversion is tried in the case of paroxysmal supraventricular tachycardia (PSVT). Adenoject® and Adenocor® are two preparations available in Indian markets for such purpose (3 mg adenosine base per ml in 2 ml & 10 ml ampoule) [66,67,68,69,70,71,72,73].
Adenosine as antiviral agent
Two congeners of adenosine namely carbocyclic 3-deazaadenosine (C-c3Ado) and carbocyclic 3-deazaadenosine (C-c3Ado) have got attention as antiviral agents. These agents have established efficacy in retarding growth of certain viruses such as rotavirus, vesicular stomatitis virus, rotavirus and reovirus. Adding to in this series, 7-deazaadenosine (tubercidin) and 3-deazaadenosine are also two of adenosine analogues which have wide spectrum antiviral activity. It is worth mentioning here that activation of A2A receptors is implicated in antiviral activity of these agents. Another adenosine nucleoside analogue in this series is BCX-4430 which, after phosphorylation, mimics ATP. This agent is converted to its corresponding triphosphate by cellular kinases. After phosphorylation, this agent gets incorporated in growing RNA chain leading to premature termination of replication process. BCX-4430 was found to have promising in vitro efficacy against SARS-CoV, Ebola virus and MERS-CoV. Its phase 1 clinical trial is in progress [74].
Adenosine in cancer immunotherapy
Adenosine has also been implicated in the pathogenesis of cancer. A tumour cell expresses very high levels of CD-73 and CD-39 as compared to normal cell. This leads to high levels of adenosine in tumour microenvironment. Adenosine suppresses the immune system in tumour microenvironment providing tumour an immunity against being attacked by immune cells. This dampening of immune system by adenosine is attributed to A2A receptors expressed on cells of immune system. In future A2A receptor and A2B receptor antagonists are expected to widen new horizons in immunotherapy of cancer. CPI-444 is one of the A2A receptor antagonist molecules which is being studied for the treatment of RCC (Renal Cell Carcinoma) [75, 76].
Adenosine as therapeutic agent: recent advances and prospect
In one of the studies, adenosine amine congener (ADAC) has been found to be a promising agent in treatment of Huntington's disease (a neurodegenerative disorder characterized by challenged cognitive and motor functions) [77, 78].
In another research A2A receptor antagonist has been found to be a promising protective agent for 3-nitropropionic acid (3NP, a mitochondrial toxin)-induced striatal neurodegeneration [79, 80]. Adenosine A2A receptor antagonists have also been found to be prospective agents for treatment of Alzheimer’s disease (AD). One such agent is MSX-3, a selective and potent A2A receptor antagonist. In this study, APPsw/PS1dE9 mice (3–9 months of age) were treated for 6 months with MSX-3. This treatment significantly increased Aβ1-40 cortical levels while reduced the cortical levels of Aβ1-42, concluding that A2A receptor antagonist was found to have a promising therapeutic potential for treatment of AD. A selective A1 adenosine receptor agonist, adenosine amine congener (ADAC), has been indicated to have significantly reduced noise-induced hearing loss in Wistar rats (in a time and dose dependent manner). This suggests that adenosine and its congeners can be studied and developed further to make otic preparations as well [81].
An adenosine congener, WS0701 {(2R, 3S, 4R, 5R)-3, 4-dihydroxy-5-[6-[(4-hydroxy-3-methoxybenzyl) amino]-9H-purin-9-yl] tetrahydrofuran-2-yl} methyl decanoate (which is an N6-substituted adenosine derivative), has remarkably prolonged non-rapid-eye movement sleep in mice. This study proved that adenosine and its congeners have potential of being used as anti-anxiety and hypnotic agent [82]. This agent also has markedly increased the Bcl-2/Bax ratio in the hippocampus of mice brains. It also has significantly reduced the stress-induced apoptosis of hippocampal neurons in mice. This study has demonstrated adenosine and its congener as promising agent in treatment of post-traumatic stress disorder [83, 84].
Another adenosine congener WS090501 (binds to adenosine A1 receptor) has been found to significantly reduce spontaneous locomotion and increase non-rapid-eye movement sleep in mice. It also prolonged latency of pentylenetetrazole-induced convulsions. All these activities confirm its sedative, hypnotic and anticonvulsive nature. WS090501 may be utilized in future in treatment of seizures and convulsions [85, 86]. Adenosine receptors can control glutamatergic and dopaminergic neurons and they have a neuro-modulatory role which can be utilized in treating schizophrenia [87, 88]. Adenosine A2 receptor and dopaminergic D2 receptors interact. They have intra-membrane antagonistic interaction which may open up new perspective in treatment of schizophrenia with adenosine congeners [89,90,91,92,93]. 5′-Cl-5′-deoxy-ENBA, a selective adenosine A1 receptor agonist inhibited hyperlocomotion produced by amphetamine in rodents which suggest that 5′-Cl-5′-deoxy-ENBA has antipsychotic action [94]. Adenosine has also been attributed in inducing hypometabolic and hypothermic state in some animals during torpor [95].
Conclusion
Although an excellent advancement has been made in understanding the role of adenosine in physiology and pathogenesis, yet the number of formulations of adenosine and its congeners in markets are limited. More advancement has been warranted to achieve a breakthrough in treatment of inflammation/inflammatory disease, erectile dysfunction, neurodegenerative disease and infections using adenosine and its congeners.
Availability of data and materials
All the information in the manuscript has been referred from the included references and is available upon request from the corresponding author.
Abbreviations
- ATP:
-
Adenosine triphosphate
- DNA:
-
Deoxy-ribonucleic acid
- RNA:
-
Ribonucleic acid
- SAM:
-
S-adenosyl-L-methionine
- GPCR:
-
G protein-coupled receptor
- PSVT:
-
Paroxysmal supraventricular tachycardia
- ENTs:
-
Equilibrative nucleoside transporters
- SAHH:
-
S-adenosyl-homocysteine hydrolase
- ADP:
-
Adenosine diphosphate
- CD-73:
-
Cluster of differentiation-73
- AdoHcy:
-
S-(5′-Adenosyl)-L-homocysteine
- EctoN:
-
Ectonucleotidase
- cAMP:
-
Adenosine 3′ 5′-cyclic monophosphate
- ED:
-
Erectile dysfunction
- ADAC:
-
Adenosine amine congener
- 3NP:
-
3-nitropropionic acid
References
WebMD, Adenosine; 2021. https://www.webmd.com/vitamins/ai/ingredientmono-1067/adenosine. Accessed 13 Mar 2021
Saladin KS (2004) Anatomy and physiology: the unity of form and function, 1st edn. McGraw Hill Learning Solutions, New York
Tortora GJ (2008) Principles of anatomy and physiology: international student version. Handbook of anatomy and physiology, vol 01. Wiley, New York, pp 56–57
Martini FH (2007) Human anatomy & physiology, 4th edn. Prentice Hall College Div, San Francisco
Seeley RR (1995) Anatomy and physiology. Mosby, New York
Waugh A, Grant A (2014) Ross and Wilson Anatomy and physiology in health and illness, 12th edn. Elsevier, Canada
Guyton AC, Hall JE (2018) Text book of medical physiology, 10th edn. Saunders Harcourt, India
Jain AK (2010) Text book of physiology, vol 02. Avichal Publishing Company, New Delhi, p 1077
Lee GR, Shaefi S, Otterbein LE (2019) HO-1 and CD39: it takes two to protect the realm. Front Immunol 10:1765
Hermes M, Osswald H, Kloor D (2007) Role of S-adenosylhomocysteine hydrolase in adenosine-induced apoptosis in HepG2 cells. Exp Cell Res 313(2):264–283
Yang R, Elsaadi S, Misund K, Abdollahi P, Vandsemb EN, Moen SH, Kusnierczyk A, Slupphaug G, Standal T, Waage A, Slørdahl TS (2020) Conversion of ATP to adenosine by CD39 and CD73 in multiple myeloma can be successfully targeted together with adenosine receptor A2A blockade. J Immunother Cancer 8(1):e000610
Samuel CE (2019) RNA editing, reference module in biomedical sciences. Elsevier, Amsterdam. https://doi.org/10.1016/B978-0-12-801238-3.11364-9
Estevez-Herrera J, Dominguez N, Pardo MR, Gonzalez-Santana A, Westhead EW, Borges R, Machado JD (2016) ATP: the crucial component of secretory vesicles. Proc Natl Acad Sci 113(28):E4098–E4106
Deaglio S, Robson SC (2011) Ectonucleotidases as regulators of purinergic signaling in thrombosis, inflammation, and immunity. Adv Pharmacol 61:301–332
Allard B, Longhi MS, Robson SC, Stagg J (2017) The ectonucleotidases CD39 and CD73: novel checkpoint inhibitor targets. Immunol Rev 276(1):121–144
Benjdia A, Balty C, Berteau O (2017) Radical SAM enzymes in the biosynthesis of ribosomally synthesized and post-translationally modified peptides (RiPPs). Front Chem 8(5):87
Boswell-Casteel RC, Hays FA (2017) Equilibrative nucleoside transporters: a review. Nucleos Nucleot Nucl 36(1):7–30
Young JD, Yao SY, Sun L, Cass CE, Baldwin SA (2008) Human equilibrative nucleoside transporter (ENT) family of nucleoside and nucleobase transporter proteins. Xenobiotica 38(7–8):995–1021
Borea PA, Gessi S, Merighi S, Vincenzi F, Varani K (2018) Pharmacology of adenosine receptors: the state of the art. Physiol Rev 98(3):1591–1625
Adair TH (2005) Growth regulation of the vascular system: an emerging role for adenosine. AM J Physiol-Reg I 289(2):R283–R296
Belardinelli L, Shryock JC, Song Y, Wang D, Srinivas M (1995) Ionic basis of the electrophysiological actions of adenosine on cardiomyocytes. FASEB J 9:359–365
Carpenter B, Nehme R, Warne T, Leslie AGW, Tate CG (2016) Structure of the adenosine A2A receptor bound to an engineered G protein. Nature 536:104–107
Corriden R, Chen Y, Inoue Y, Beldi G, Robson SC, Insel PA, Junger WG (2008) Ecto-nucleoside triphosphate diphosphohydrolase 1 (E-NTPDase1/CD39) regulates neutrophil chemotaxis by hydrolyzing released ATP to adenosine. J Biol Chem 283:28480–28486
Corriden R, Self T, Akong-Moore K, Nizet V, Kellam B, Briddon SJ, Hill SJ (2013) Adenosine-A3 receptors in neutrophil microdomains promote the formation of bacteria-tethering cytonemes. EMBO Rep 14(8):726–732
Cronstein BN, Daguma L, Nichols D, Hutchison AJ, Williams M (1990) The adenosine/neutrophil paradox resolved: human neutrophils possess both A1 and A2 receptors that promote chemotaxis and inhibit O2 generation, respectively. J Clin Invest 85(4):1150–1157
Fishman P, Bar-Yehuda S, Liang BT, Jacobson KA (2012) Pharmacological and therapeutic effects of A3 adenosine receptor agonists. Drug Disco Today 17(7–8):359–366
Fredholm BB, Arslan G, Halldner L, Kull B, Schulte G, Wasserman W (2000) Structure and function of adenosine receptors and their genes. N-S Arch Pharmacol 362(4–5):364–374
Modi BN, Rahman H, Sherif SA, Ellis H, Eruslanova K, Chiribiri A, Perera D (2018) Is heart rate response a reliable marker of adenosine-induced coronary hyperemia? Int J Card Imaging 34(7):1117–1125
Adjedj J, Toth GG, Johnson NP, Pellicano M, Ferrara A, Flore V, Di-Gioia G, Barbato E, Muller O, De-Bruyne B (2015) Intracoronary adenosine: dose-response relationship with hyperemia. JACC Cardiovasc Interv 8(11):1422–1430
Mediero A, Cronstein BN (2013) Adenosine and bone metabolism. Trends Endrocrinol Metab 24(6):290–300
He W, Cronstei B (2011) The roles of adenosine and adenosine receptors in bone remodeling. Front Biosci 3:888–895
Mediero A, Wilder T, Shah L, Cronstein BN (2018) Adenosine A2A receptor (A2AR) stimulation modulates expression of semaphorins 4D and 3A, regulators of bone homeostasis. FASEB J 32(7):3487–3501
Evans BA (2012) Does adenosine play a role in bone formation, resorption and repair? Purinergic Signal 8(2):177–180
Kara FM, Doty SB, Boskey A, Goldring S, Zaidi M, Fredholm BB, Cronstein BN (2010) Adenosine A(1) receptors regulate bone resorption in mice: adenosine A(1) receptor blockade or deletion increases bone density and prevents ovariectomy-induced bone loss in adenosine A(1) receptor-knockout mice. Arthritis Rheum 62(2):534–541
Mediero A, Kara FM, Wilder T, Cronstein BN (2012) Adenosine A(2A) receptor ligation inhibits osteoclast formation. Am J Pathol 180(2):775–786
Iyu D, Glenn JR, White AE, Fox SC, Heptinstall S (2011) Adenosine derived from ADP can contribute to inhibition of platelet aggregation in the presence of a P2Y12 antagonist. Arterioscler Thromb Vasc Biol 31(2):416–422
Wolska N, Boncler M, Polak D, Wzorek J, Przygodzki T, Gapinska M, Watala C, Rozalski M (2020) Adenosine receptor agonists exhibit anti-platelet effects and the potential to overcome resistance to P2Y12 receptor antagonists. Molecules 25(1):130
An emerging role for adenosine and its receptors in bone homeostasis: Scientific Figure on ResearchGate. https://www.researchgate.net/figure/Adenosine-synthesis-and-metabolic-pathways-inside-and-outside-of-a-cell-Within-thecellfig1231614255. Accessed 21 Jul 2021
Neonatal hepatic steatosis by disruption of the adenosine kinase gene: Scientific Figure on ResearchGate. https://www.researchgate.net/figure/Pathways-of-adenosine-metabolism-Adenosine-is-formed-either-by-hydrolysis-of-AMP-or-by_fig1_11374143. Accessed 21 Jul 2021
Colorado, adenosine. https://www.colorado.edu/lab/bachtell/sites/default/files/styles/medium/public/block/a1_d1_intx_0.jpg?itok=wJ7Iu0O2. Accessed 18 Jul 2021
Wikimedia, extracellular. https://upload.wikimedia.org/wikipedia/commons/f/f6/Purinergic_signalling.jpg. Accessed 18 Jul 2021
Hasko G, Cronstein B (2013) Regulation of inflammation by adenosine. Front Immunol 4:85
Cronstein BN, Sitkovsky M (2017) Adenosine and adenosine receptors in the pathogenesis and treatment of rheumatic diseases. Nat Rev Rheumatol 13(1):41–51
Cronstein BN (1994) Adenosine, an endogenous anti-inflammatory agent. J Appl Physiol 76(1):5–13
Cronstein BN, Levin RI, Philips M, Hirschhorn R, Abramson SB, Weissmann G (1992) Neutrophil adherence to endothelium is enhanced via adenosine A1 receptors and inhibited via adenosine A2 receptors. J Immunol 148(7):2201–2206
Krump E, Borgeat P (1999) Adenosine: an endogenous inhibitor of arachidonic acid release and leukotriene biosynthesis in human neutrophils. Adv Exp Med Biol 447:107–115
Barletta KE, Ley K, Mehrad B (2012) Regulation of neutrophil function by adenosine. Arterioscler Thromb Vasc Biol 32(4):856–864
Hasko G, Cronstein B (2013) Regulation of inflammation by adenosine. Front Immunol 8(4):85
Riksen NP, Barrera P, van den Broek PH, van Riel PL, Smits P, Rongen GA (2006) Methotrexate modulates the kinetics of adenosine in humans in vivo. Ann Rheum Dis 65(4):465–470
Friedman B, Cronstein B (2019) Methotrexate mechanism in treatment of rheumatoid arthritis. Jt Bone Spine 86(3):301–317
Thammavongsa V, Kern JW, Missiakas DM, Schneewind O (2009) Staphylococcus aureus synthesizes adenosine to escape host immune responses. J Exp Med 206(11):2417–2427
Zhang BZ, Cai J, Yu B, Xiong L, Lin Q, Yang XY, Xu C, Zheng S, Kao RY, Sze K, Yuen KY, Huang JD (2017) Immunotherapy targeting adenosine synthase a decreases severity of Staphylococcus aureus infection in mouse model. J Infect Dis 216(2):245–253
Thammavongsa V, Schneewind O, Missiakas DM (2011) Enzymatic properties of Staphylococcus aureus adenosine synthase (AdsA). BMC Biochem 12:56
Pernet E, Brunet J, Guillemot L, Chignard M, Touqui L, Wu Y (2015) Staphylococcus aureus adenosine inhibits sPLA2-IIA–mediated host killing in the airways. J Immunol 194(11):5312–5319
Tonello F, Zornetta I (2012) Bacillus anthracis factors for phagosomal escape. Toxins 4(7):536–553
Bouma MG, Jeunhomme TM, Boyle DL, Dentener MA, Voitenok NN, van den Wildenberg FA, Buurman WA (1997) Adenosine inhibits neutrophil degranulation in activated human whole blood: involvement of adenosine A2 and A3 receptors. J Immunol 158(11):5400–5408
Drygiannakis I, Ernst PB, Lowe D, Glomski IJ (2011) Immunological alterations mediated by adenosine during host-microbial interactions. Immunol Res 50(1):69–77
Baratloo A, Rouhipour A, Forouzanfar MM, Safari S, Amiri M, Negida A (2016) The role of caffeine in pain management: a brief literature review. Anesth Pain Med 6(3):e33193
Phatarpekar PV, Wen J, Xia Y (2010) Role of adenosine signaling in penile erection and erectile disorders. J Sex Med 7(11):3553–3564
Dai Y, Zhang Y, Phatarpekar P, Mi T, Zhang H, Blackburn MR, Xia Y (2009) Adenosine signaling, priapism and novel therapies. J Sex Med 6(3):292–301
Wen J, Xia Y (2012) Adenosine signaling: good or bad in erectile function? Arterioscler Thromb Vasc Biol 32(4):845–850
Chiang PH, Wu SN, Tsai EM, Wu CC, Shen MR, Huang CH, Chiang CP (1994) Adenosine modulation of neurotransmission in penile erection. Br J Clin Pharmacol 38(4):357–362
Wen J, Grenz A, Zhang Y, Dai Y, Kellems RE, Blackburn MR, Eltzschig HK, Xia Y (2011) A2B adenosine receptor contributes to penile erection via PI3K/AKT signaling cascade-mediated eNOS activation. FASEB 25(8):2823–2830
National centre for biotechnology information: PubChem Compound Summary for CID, 219024, Regadenoson, 2020. https://pubchem.ncbi.nlm.nih.gov/compound/Regadenoson. Accessed 04 Apr 2021
Zhao G, Serpllion S, Shryock J, Messina E, Xu X, Ochoa M, Belardinelli L, Hintze TH (2008) Regadenoson, a novel pharmacologic stress agent for use in myocardial perfusion imaging, does not have a direct effect on the QT interval in conscious dogs. J Cardiovasc Pharmacol Ther 52(5):467–473
Jager PL, Buiting M, Mouden M, Oostdijk AH, Timmer J, Knollema S (2014) Regadenoson as a new stress agent for myocardial perfusion SPECT imaging. Initial experience in Holland. Span J Nucl Med Mol Imaging 33(6):346–351
Wilbur SL, Marchlinski FE (1997) Adenosine as an antiarrhythmic agent. Am J Cardiol 79(12A):30–37
Tripathi KD (2017) Pharmacological classification of drugs, 5th edn. Jaypee Brothers Medical Publishers (P) Ltd., New Delhi, pp 99–101
Adenoject 6 mg injection; 2021. https://www.1mg.com/drugs/adenoject-6mg-injection-241034. Accessed 19 Mar 2021
Medicscientist: Adenoject; 2021. https://medicscientist.com/drug/adenoject-210ml-3mgml. Accessed 19 Mar 2021
Adenocor; 2021. https://www.1mg.com/drugs/adenocor-6mg-injection-41049. Accessed 19 Mar 2021
Virtual medical centre: Adenocor; 2021. https://www.myvmc.com/drugs/adenocor/. Accessed 19 Mar 2021
De Clercq E, Bergstrom DE, Holy A, Montgomery JA (1984) Broad-spectrum antiviral activity of adenosine analogues. Antivir Res 4(3):119–133
Taylor R, Kotian P, Warren T, Panchal R, Bavari S, Julander J, Dobo S, Rose A, El-Kattan Y, Taubenheim B, Babu Y (2016) BCX4430—a broad-spectrum antiviral adenosine nucleoside analog under development for the treatment of Ebola virus disease. J Infect Public Health 9(3):220–226
Leone RD, Emens LA (2018) Targeting adenosine for cancer immunotherapy. J Immunother Cancer 6(1):57
Adenosine—a critical checkpoint in the tumor microenvironment-Cancer Biology. http://blogs.shu.edu/cancer/2018/02/21/adenosine-a-critical-checkpoint-in-the-tumor-microenvironment/ Accessed 18 Jul 2021
Benarroch EE (2008) Adenosine and its receptors: multiple modulatory functions and potential therapeutic targets for neurologic disease. Neurology 70(3):231–236
Blum D, Gall D, Galas MC, d’Alcantara P, Bantubungi K, Schiffmann SN (2002) The adenosine A1 receptor agonist adenosine amine congener exerts a neuroprotective effect against the development of striatal lesions and motor impairments in the 3-nitropropionic acid model of neurotoxicity. J Neurosci 22(20):9122–9133
Blum D, Galas MC, Pintor A, Brouillet E, Ledent C, Muller CE, Bantubungi K, Galluzzo M, Gall D, Cuvelier L, Rolland AS, Popoli P, Schiffmann SN (2003) A dual role of adenosine A2A receptors in 3-nitropropionic acid-induced striatal lesions: implications for the neuroprotective potential of A2A antagonists. J Neurosci 23(12):5361–5369
Faivre E, Coelho JE, Zornbach K, Malik E, Baqi Y, Schneider M, Cellai L, Carvalho K, Sebda S, Figeac M, Eddarkaoui S, Caillierez R, Chern Y, Heneka M, Sergeant N, Muller CE, Halle A, Buee L, Lopes LV, Blum D (2018) Beneficial effect of a selective adenosine A2A receptor antagonist in the APPswe/PS1dE9 mouse model of Alzheimer’s disease. Front Mol Neurosci 11:235
Vlajkovic SM, Thorne PR, Rajan R, Gale JE (2015) Preventing hearing loss and restoring hearing: a new outlook. BioMed Res Int 868716:1–2
Bai XY, Zhang XQ, Zhang YH, Wu S, Hao LH, Liu R, Huang ZL, Zhang WK, Sun ZM, Du GH (2014) WS0701: a novel sedative-hypnotic agent acting on the adenosine system. Behav Pharmacol 25(7):648–660
Huang ZL, Liu R, Bai XY, Zhao G, Song JK, Wu S, Du GH (2014) Protective effects of the novel adenosine derivative WS0701 in a mouse model of posttraumatic stress disorder. Acta Pharmacol Sin 35(1):24–32. https://doi.org/10.1038/aps.2013.143
Li X, Han F, Liu D, Shi Y (2010) Changes of Bax, Bcl-2 and apoptosis in hippocampus in the rat model of post-traumatic stress disorder. Neurol Res 32(6):579–586. https://doi.org/10.1179/016164110X12556180206194
Li W, Zhang JJ (2011) Sedative, hypnotic and anticonvulsive effects of an adenosine analogue WS090501. Acta Pharmacol Sin 46(6):742–746
Masino SA, Kawamura M, Ruskin DN (2014) Adenosine receptors and epilepsy: current evidence and future potential. Int Rev Neurobiol 119:233–255
Turcin A, Dolzan V, Porcelli S, Serretti A, Plesnicar BK (2016) Adenosine hypothesis of antipsychotic drugs revisited: pharmacogenomics variation in nonacute schizophrenia. Omics J Integr Biol 20(5):283–289
Wardas J (2008) Potential role of adenosine A2A receptors in the treatment of schizophrenia. Front Biosci 13:4071–4096
Ballarin M, Reiriz J, Ambrosio S, Mahy N (1995) Effect of locally infused 2-chloroadenosine, an A1 receptor agonist, on spontaneous and evoked dopamine release in rat neostriatum. Neurosci Lett 185(1):29–32
Solinas M, Ferre S, You ZB, Karcz-Kubicha M, Popoli P, Goldberg SR (2002) Caffeine induces dopamine and glutamate release in the shell of the nucleus accumbens. J Neurosci 22(15):6321–6324
Borycz J, Pereira MF, Melani A, Rodrigues RJ, Kofalvi A, Panlilio L, Pedata F, Goldberg SR, Cunha RA, Ferre S (2007) Differential glutamate-dependent and glutamate-independent adenosine A1 receptor-mediated modulation of dopamine release in different striatal compartments. J Neurochem 101(2):355–363
Moser A, Liebetrau A, Cramer H (1991) Adenosine receptor-coupled adenylate cyclase in the caudate nucleus of the rat brain. Neuropharmacology 30(7):769–773
Ciruela F, Casado V, Rodrigues RJ, Lujan R, Burgueno J, Canals M, Borycz J, Rebola N, Goldberg SR, Mallol J, Cortes A, Canela EI, Lopez-Gimenez JF, Milligan G, Lluis C, Cunha RA, Ferre S, Franco R (2006) Presynaptic control of striatal glutamatergic neurotransmission by adenosine A1–A2A receptor heteromers. J Neurosci 26(7):2080–2087
Ossowska K, Kosmowska B, Wardas J (2020) Potential antipsychotic action of the selective agonist of adenosine A1 receptors, 5′-Cl-5′-deoxy-ENBA, in amphetamine and MK-801 rat models. Pharmacol Rep 72:580–588
Carlin JL, Jain S, Gizewski E, Wan TC, Tosh DK, Xiao C, Auchampach JA, Jacobson KA, Gavrilova O, Reitman ML (2017) Hypothermia in mouse is caused by adenosine A1 and A3 receptor agonists and AMP via three distinct mechanisms. Neuropharmacology 114:101–113
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
RB raised the basic theme and extracted the information for writing paper. He was a major contributor in writing the manuscript. PS provided guidance for content selection and referencing. VJ provided guidance for terms and language use and shared certain tips to minimize plagiarism. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
Cite this article
Batra, R., Jain, V. & Sharma, P. Adenosine: a partially discovered medicinal agent. Futur J Pharm Sci 7, 214 (2021). https://doi.org/10.1186/s43094-021-00353-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43094-021-00353-w