
Abstract
Background
IgG4-mediated sclerosing cholangitis (IgG4-SC) is an autoimmune disease that generally occurs in association with type 1 autoimmune pancreatitis (AIP). However, an isolated variant of IgG4-SC is a rare disease that can occur without concurrent AIP and closely mimics extrahepatic cholangiocarcinoma both clinically and radiologically.
Case presentation
Here, we report a case of an isolated variant of IgG4-SC, which was pre-operatively diagnosed as hilar cholangiocarcinoma. Pathological and immunohistochemical examination revealed features suggestive of IgG4-SC, which was confirmed by elevated serum IgG4 levels measured postoperatively.
Conclusion
Therefore, IgG4-SC should be carefully ruled out in patients presenting with isolated bile duct obstruction, before performing morbid surgical procedures.
Similar content being viewed by others


Background
IgG4-related disease (IgG4-RD) is a systemic immune-mediated chronic inflammatory disease, commonly affecting middle-aged to elderly men, and is characterized by IgG4 type of plasma cell infiltration accompanied by dense fibrosis of the affected organs [1]. IgG4-mediated sclerosing cholangitis (IgG4-SC) is the biliary manifestation of this disease in which the patients present with obstructive jaundice and weight loss. It usually occurs in association with type 1 autoimmune pancreatitis (AIP) [2]. Isolated variant of IgG4-SC is a rare disease that occurs without concurrent AIP. The closest differential diagnosis for isolated IgG4-SC is extra-hepatic/ hilar cholangiocarcinoma (CCA), as both these entities have overlapping clinical and radiological findings. However, the management and prognosis of both these entities are entirely different.
Case presentation
A 57-year-old male, farmer by occupation and non-alcoholic, presented with dull aching upper abdominal pain and vomiting for 3 months associated with progressive yellowish painless discoloration of sclera, generalized pruritis, and significant weight loss noted in the past 2 weeks. He did not have a fever, abdominal distension, hematemesis, melena, clay-colored stools, chest and bony pain, or breathlessness. The patient was a chronic smoker for the past 30 years and a known hypertensive for the past 15 years on treatment. On examination, the patient was icteric and malnourished with multiple scratch marks on the skin. On abdominal examination, he had palpable hepatomegaly, 3 cm from the right costal margin. His liver function tests (LFT) suggested an obstructive pattern of jaundice. LFT values were as follows: total bilirubin, 7.73 mg/dl; direct bilirubin, 5 mg/dl; alanine aminotransferase (ALT), 53 IU/L; aspartate aminotransferase (AST), 41 IU/L; alkaline phosphatase (ALP), 280 IU/L; and gamma-glutamyl transferase (GGT), 41 IU/L. His CA19-9 levels were elevated (CA19-9, 80 U/mL; reference range: 0–37U/mL)
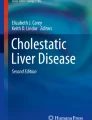
Contrast-enhanced computed tomography (CECT) in the abdomen showed enlargement of the liver with intra-hepatic biliary radicle dilatation (IHBRD). There was asymmetrical circumferential wall thickening of the common bile duct in the hilum, causing proximal bilobar IHBRD with few enlarged lymph nodes in the retro portal and peripancreatic region (Fig. 1). Pancreas and main pancreatic duct (MPD) appeared unremarkable. These findings were confirmed by Magnetic resonance cholangiopancreatography (MRCP). Correlating with clinical findings, LFT, serum CA19-9 levels, and imaging, a clinical diagnosis of hilar CCA was rendered.

MRI axial cuts at the level of hilum showing bilobar IHBRD with the absence of formation of the primary confluence
A staging laparotomy was performed, which showed a hard stricturous lesion of length 2.5 cm in the hilum extending to both right and left hepatic ducts proximally. He underwent open segment I and IV resection of the liver with extra-hepatic bile duct resection and standard lymphadenectomy followed by Roux-en-Y anastomosis. The resected tissue was submitted for histopathological examination.
Histopathological examination of the gross thickening present at the confluence of the hepatic and bile duct showed diffuse fibrosis of the duct wall with accentuation around the peri-biliary glands. There was a dense transmural inflammatory infiltrate as well as around the ductules comprising predominantly of plasma cells, lymphocytes, and few eosinophils with perineural extension (Fig. 2). However, there was no evidence of dysplasia or invasive malignancy in the biliary epithelium. Sections from the liver showed portal expansion by moderate lymphoplasmacytic infiltrates in the portal tracts, mild bile ductular reaction along with porto-portal bridging fibrosis. Lobular hepatocytes showed feathery degeneration with canalicular cholestasis. There was no obliterative cholangitis, peri-ductal onion skin fibrosis, or ductopenia. One of the hilar lymph nodes also showed paracortical expansion by plasma cells. The plasma cells in the hilar stricture and the hilar lymph node were highlighted by IgG and IgG4 immunostains. There were around 30 IgG4-positive plasma cells per high power field with an IgG4/IgG ratio of more than 40% (Fig. 3).

A Gross image of the resection specimen which shows thickening at the confluence of the hepatic and bile duct. B and C Dense transmural inflammatory infiltrate and diffuse fibrosis of the duct wall with accentuation around the peri-biliary glands (H&E; 40× and 100×). D Inflammatory infiltrate around the ductules comprises predominantly of plasma cells, lymphocytes, and few eosinophils (H&E; 400×)

A The plasma cells in the hilar stricture were highlighted by IgG immunostain (100×). B IgG4 immunostain highlighted around 30 IgG4-positive plasma cells per high power field (400×). C Liver showed portal expansion by moderate lymphoplasmacytic infiltrates, mild bile ductular reaction, and porto-portal bridging fibrosis. (H&E; 100×). D Porto-portal bridging fibrosis is highlighted by Masson’s trichrome stain (MT; 100×)
Correlating with the morphological and immunohistochemical findings, a diagnosis of IgG4-mediated sclerosing cholangitis (IgG4-SC) was favored. Retrospectively, postoperative serum IgG4 level was measured which was 16.6 g/L (reference range: 0.03 to 2.0 g/L). On thorough examination, there were no foci of IgG4-related disease in any other organs, henceforth a diagnosis of an isolated variant of IgG4-mediated sclerosing cholangitis (IgG4-SC) was favored.
Postoperatively, the patient’s bilirubin level dropped with an improvement in health status. The patient is on regular follow-up with no recurrence of the disease.
Discussion
IgG4-SC is the biliary manifestation of IgG4-RD which is usually associated with Type 1 autoimmune pancreatitis (AIP) [2]. Approximately 92 to 95% of IgG4-SC cases had concurrent Type 1 AIP [3]. Radiologically, there can be diffuse or segmental thickening and narrowing of the common bile duct causing IHBRD. On cholangiography, IgG4-SC was classified into four categories based on the location of the strictures in the biliary tract [3]. HISORt criteria were developed by Mayo Clinic to facilitate the diagnosis of IgG4-SC, which included histological findings, imaging, serological tests, other organ involvement, and response to steroid treatment [4].
Isolated variant of IgG4-SC is a rare entity described in the literature, which occurs in the absence of AIP with only a few published reports available [5,6,7,8,9]. Diagnosis of isolated IgG4-SC becomes challenging, as the closest clinical and radiological differential diagnosis is extra-hepatic CCA. Both isolated IgG4-SC and CCA are common in the elderly male population and exhibit similar clinical presentation and radiological findings [10]. It is very crucial to differentiate between these two entities, as there is an immense difference in their biological behavior, treatment, and prognosis. Steroid is the main stay of management for IgG4-RD and exhibits excellent prognosis, whereas cholangiocarcinoma is surgically resected and has a dismal prognosis.
Primary sclerosing cholangitis (PSC) is another entity that has a similar clinical presentation as that of IgG4-SC, but has the characteristic beaded appearance of bile ducts in radiology [11]. Histologically, PSC shows fibrosis causing onion skinning of large intrahepatic and/ or extrahepatic bile ducts leading to multiple strictures. It has a close association with inflammatory bowel disease and generally does not respond well to steroids.
Raised serum IgG4 levels and the presence of extra-biliary organ involvement provide vital clues which guide us toward the diagnosis of IgG4-RD. However, there are some case reports which describe the normal or modest elevation of serum IgG4 levels in isolated IgG4-SC [12]. Elevated serum IgG4 levels are also associated with other disease entities like PSC and cholangiocarcinoma. However, it is not a specific finding [1]. A cutoff value of four times the upper normal limit of serum IgG4 levels has 100% specificity for the diagnosis of IgG4 SC. In our case, IgG4 levels are 8 times elevated than the upper normal levels of IgG4. Hence, increasing the cut-off increases the specificity [13].
In our case, IgG4-SC was misdiagnosed as hilar CCA clinically, due to the presence of isolated thickening of bile ducts without pancreas involvement and enlargement of multiple hilar lymph nodes. Owing to the rarity of this disease and low clinical suspicion, pre-operative measurement of serum IgG4 levels was not performed as a part of our routine pre-operative investigation panel. However, the presence of classical histopathological findings in the resection specimen and elevated postoperative serum IgG4 levels aided us in the diagnosis of IgG4-SC.
Conclusion
Even though an isolated variant of IgG4-SC is a rare entity, it should be considered as a differential diagnosis of extrahepatic CCA while evaluating patients presenting with obstructive jaundice and bile duct strictures. Pre-operative measurement of serum IgG4 levels should be performed in cases with a high index of suspicion before performing invasive surgical procedures, especially in the absence of autoimmune pancreatitis. Hence, a careful correlation of clinical presentation, radiological findings to look for other organ involvement, and serological tests is necessary for accurate diagnosis of isolated IgG4-SC.
Availability of data and materials
Not applicable.
Abbreviations
- AIP:
-
Autoimmune pancreatitis
- ALP:
-
Alkaline phosphatase
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- CCA:
-
Cholangiocarcinoma
- GGT:
-
Gamma-glutamyl transferase
- IgG4-RD:
-
IgG4-related disease
- IgG4-SC:
-
IgG4-mediated sclerosing cholangitis
- IHBRD:
-
Intra-hepatic biliary radicle dilatation
- LFT:
-
Liver function tests
- MPD:
-
Main pancreatic duct
- PSC:
-
Primary sclerosing cholangitis
References
Cheuk W, Chan JKC (2010) IgG4-related Sclerosing Disease: A Critical Appraisal of an Evolving Clinicopathologic Entity. Advances in Anatomic Pathology 17:303–332
Lin J, Cummings OW, Greenson JK, House MG, Liu X, Nalbantoglu llk et al (2015) IgG4-related sclerosing cholangitis in the absence of autoimmune pancreatitis mimicking extrahepatic cholangiocarcinoma. Scand J Gastroenterol 50:447–53
Nakazawa T, Ohara H, Sano H, Ando T, Joh T (2006) Schematic Classification of Sclerosing Cholangitis With Autoimmune Pancreatitis by Cholangiography. Pancreas 32:229
Chari ST, Smyrk TC, Levy MJ, Topazian MD, Takahashi N, Zhang L et al (2006) Diagnosis of Autoimmune Pancreatitis: The Mayo Clinic Experience. Clinical Gastroenterology and Hepatology. 4:1010–6
Xiao J, Li G, Yang G, Jia C, Li B (2017) Case report: A female case of isolated IgG4-related sclerosing cholangitis mimicking cholangiocarcinoma. Medicine (Baltimore) 96:e6542
Minh Thong P, Dang Luu V, Tra My TT, Xuan Hien N, Anh Tuan T, Minh Duc N (2021) IgG4-Related Sclerosing Cholangitis Mimicking Cholangiocarcinoma. Case Rep Oncol 14:39–46
Mittelstaedt A, Meier PN, Dankoweit-Timpe E, Christ B, Jaehne J (2018) IgG4-related sclerosing cholangitis mimicking hilar cholangiocarcinoma (Klatskin tumor): a case report of a challenging disease and review of the literature. Innov Surg Sci 3:157–63
Rungsakulkij N, Sornmayura P, Tannaphai P (2017) Isolated IgG4-related sclerosing cholangitis misdiagnosed as malignancy in an area with endemic cholangiocarcinoma: a case report. BMC Surg 17:17
Nasser R, Gilshtein H, Mansour S, Yasin K, Borzellino G, Khuri S (2021) Isolated Type Immunoglobulin G4 Sclerosing Cholangitis: The Misdiagnosed Cholangiocarcinoma. J Clin Med Res 13:75–81
Joshi D, Webster GJM (2014) IgG4 Related Sclerosing Cholangitis. Advances in Hepatology. 2014:e632320
Tanaka A (2019) IgG4-Related Sclerosing Cholangitis and Primary Sclerosing Cholangitis. Gut Liver 13:300–307
Nguyen-tat M, Gamstätter T, Marquardt JU, Geißinger E, Schadmand-Fischer S, Lang H et al (2012) IgG4-related sclerosing cholangitis mimicking cholangiocarcinoma. Z Gastroenterol 50:1008–12
Ohara H, Nakazawa T, Kawa S, Kamisawa T, Shimosegawa T, Uchida K et al (2013) Establishment of a serum IgG4 cut-off value for the differential diagnosis of IgG4-related sclerosing cholangitis: a Japanese cohort. J Gastroenterol Hepatol 28:1247–51
Acknowledgements
Not applicable.
Funding
No funding is involved in this case report.
Author information
Authors and Affiliations
Contributions
SR – preparation of the manuscript. SBH – contribution to the manuscript and manuscript correction. SR and SBH – diagnosis of the case. SG and BP – collection of clinical information. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ravi, S., Hanuman, S.B., Gnanasekhran, S. et al. Isolated variant of IgG4-sclerosing cholangitis masquerading as hilar cholangiocarcinoma — an enigmatic entity. Egypt Liver Journal 13, 23 (2023). https://doi.org/10.1186/s43066-023-00256-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43066-023-00256-w