
Abstract
Background
Hepatorenal syndrome is still a diagnosis of exclusion despite new classification.
Aims
To validate the accuracy of urinary neutrophil gelatinase-associated lipocalin, interleukin-18, and kidney injury molecule-1 in the new diagnostic criteria of hepatorenal syndrome in Egyptian patients with hepatitis C virus-related liver cirrhosis using serum creatinine as a gold standard test for acute kidney injury.
Methods
One-hundred twenty cirrhotic patients with ascites were recruited and divided into two groups depending on the presence or absence of renal impairment, and 40 age- and sex-matched cirrhotic patients without ascites used as controls participated in the study. Urinary biomarkers were measured and compared with conventional biomarkers used to assess kidney function (serum creatinine, estimated glomerular filtration rate).
Results
The mean urinary neutrophil gelatinase-associated lipocalin, interleukin-18, and kidney injury molecule-1 were statistically significantly higher in patients with hepatorenal syndrome and were found to be helpful in the early detection with cutoff values of 125 ng/ml, 34.8 pg/ml, and 3.1 pg/ml, respectively.
Conclusions
Urinary neutrophil gelatinase-associated lipocalin, interleukin-18, and kidney injury molecule-1 levels are higher in patients with cirrhotic ascites complicated by HRS-AKI using the new definition of HRS, but IL-18 has lower sensitivity and specificity for the prediction of HRS-AKI as compared to NGAL and KIM-1.
Similar content being viewed by others


Background
Renal dysfunction is a common complication of liver cirrhosis, occurring in approximately 20–50% of all patients with cirrhosis admitted into hospital [1]. Most of these cases are due to episodes of acute kidney injury (AKI). Two-thirds of these AKI episodes are functionally related to hemodynamic changes in cirrhosis, consisting of splanchnic and systemic arterial vasodilatation with resultant reduction in effective arterial blood volume [2], whereas the remainder of AKI episodes are related to renal structural damage, more commonly tubular than glomerular [3]. The most severe form of AKI is type 1 hepatorenal syndrome (HRS-AKI), which, if left untreated, has a median survival of 7–10 days [4]. The use of vasoconstrictors in HRS-AKI has led to improvement in renal function in only one-third of patients for unclear reasons [5]. This may be attributed to the delayed initiation of vasoconstrictor therapy in HRS-AKI, in which many patients may have crossed the “no return” threshold. This delay may be attributed to the use of serum creatinine to assess renal function which tends to overestimate the glomerular filtration rate in decompensated cirrhosis [6]. Also, the increase in serum creatinine often lags (48–72 h) behind the onset of injury [7]. Prolonged ischemia secondary to renal vasoconstriction in late-presenting HRS-AKI can also result in structural damage, such as acute tubular necrosis (ATN), thus blurring the line between structural and functional causes of AKI in cirrhosis [6]. Moreover, ATN and HRS-AKI can present with the same features, thus making the differentiation of the different types of AKI and treatment decisions difficult.
To overcome some of these issues, the International Ascites Club and the Acute Dialysis Quality Initiative have proposed the following diagnostic criteria for the HRS-AKI: acute rise in serum creatinine ≥ 0.3 mg/dL within 48 h or ≥ 50% increase from baseline within 7 days irrespective of the final serum creatinine level in patients with acute or chronic liver disease with advanced liver failure and portal hypertension in the absence of any other apparent cause for the AKI [8]. However, HRS-AKI patients diagnosed with these new diagnostic criteria still had a worse survival, possibly reflecting delayed treatment intervention [9].
With the discovery and validation of candidate AKI biomarkers, we aimed in this study to compare the diagnostic value of three out of these biomarkers of tubular injury in the diagnosis of HRS which is up until now a diagnosis of exclusion with challenging differential diagnosis and to correlate these biomarkers with morbidity and mortality using different scoring systems. These biomarkers include neutrophil gelatinase-associated lipocalin (NGAL), interleukin 18 (IL-18), and kidney injury molecule-1 (KIM-1). The primary objective of this study was to determine whether these biomarkers may provide early diagnosis of HRS in patients with HCV-related liver cirrhosis.
Methods
Study participants
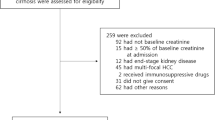
The study was reviewed and approved by Minia University Faculty of Medicine Research ethics committee and was conducted in accordance with the Helsinki Declaration. Informed consent was obtained from all study participants, and the study protocol was approved by the institute’s committee on human research. This study was an observational, prospective, hospital-based, case-controlled study with the participants recruited from the inpatient service of Internal Medicine Department, Minia University Hospital. The study enrolled one-hundred and sixty (160) patients with HCV-related liver cirrhosis. Patients were classified into three groups: cirrhotic patients without ascites used as controls (40 patients), cirrhotic patients with ascites but without renal impairment (60 patients), and cirrhotic patients with ascites and with renal impairment diagnosed as having HRS-AKI (formerly, HRS type 1) (60 patients). The inclusion criteria were cirrhotic patients who are HCV positive, with liver cirrhosis diagnosed on liver biopsy or through clinical, radiographic, and biochemistry investigations, and HRS-AKI patients were diagnosed using the revised diagnostic criteria of hepatorenal syndrome (HRS) with rapidly progressive decrease in kidney function, defined as absolute increase in serum creatinine ≥ 0.3 mg/dl within 48 h or relative increase in serum creatinine ≥ 50% from baseline within 7 days and/or decrease in urine output ≤ 0.5 ml/kg ≥ 6 h. The exclusion criteria were HRS-NAKI (formerly HRS type 2) defined as stable or slowly progressive decrease in kidney function with eGFR < 60 ml/min/1.73m2, serious comorbidities (functional class IV heart failure, O2-dependent COPD, advanced cancer), chronic kidney disease, other causes of liver cirrhosis, shock, documented established parenchymal kidney disease, obstructive uropathy, use of nephrotoxic drugs in the previous 30 days, urinary tract infection, anuria for 12 h, need for renal replacement therapy, or any solid organ transplantation.
Primary predictors and outcomes
The primary predictors were urinary concentrations of neutrophil gelatinase-associated lipocalin (NGAL), kidney injury molecule-1 (KIM-1), and interleukin-18 (IL-18). Within 2 to 3 h of admission, 10 mL urine was collected from study participants and centrifuged at 2000g for 20 min, and the supernatant was frozen at −800 °C and retained for analysis. We measured urinary NGAL, KIM-1, by commercially available enzyme-linked immunosorbent assay (ELISA) kit (BOSTER Biological Technology Co. USA), according to the manufacturer’s instructions.
Urine NGAL assay was performed according to the following steps: the microtiter plate was coated with monoclonal anti-NGAL antibody. A total of 100 μl of standards or samples are added to the appropriate microtiter plate and incubated for 90 min at 37 °C. Remove the liquid of each well, add 0.1 ml of a biotin-conjugated polyclonal anti-NGAL antibody to each well, and incubate for 1 h at 37 °C. Aspirate each well and wash with wash buffer, repeating the process three times for a total of three washes, followed by the addition of 100 μl of avidin conjugated to horseradish peroxidase (HRP) to each microplate and incubated for 30 min at 37 °C. Color development was achieved using a 90 μl TMB substrate solution is added to each well and incubated for 30 min in the dark at 37 °C. Only those wells that contain biotin-conjugated antibody and enzyme-conjugated avidin will exhibit a change in color. The enzyme-substrate reaction is terminated by the addition of 100 μl sulfuric acid solution, and the color change is measured spectrophotometrically at a wavelength of 450 nm ± 2 nm. Serial dilutions of recombinant human NGAL were used to establish a standard curve. The detection limit of NGAL with this research assay is 15.63–1000 pg/ml. The intra-assay coefficients of variations (CVs) were 3.9% and 6.2% at 1246 ± 48.6 and 6827 ± 423.3 pg/ml, respectively. Inter-assay CVs were 8.1% and 6.9% at 1522 ± 123.3 and 7133 ± 492.2 pg/ml, respectively.
Urine KIM-1 assay was performed according to the following steps: the microtiter plate was coated with monoclonal anti-KIM-1 antibody. A total of 100 μl of standards and samples are added to the appropriate microtiter plate and incubated for 90 min at 37 °C. Remove the liquid of each well, add 100 μl of a biotin-conjugated polyclonal anti-KIM-1 antibody to each well, and incubate for 1 h at 37 °C. Aspirate each well and wash with wash buffer, repeating the process three times for a total of three washes, followed by the addition of 100 μl of avidin conjugated to HRP to each microplate and incubated for 30 min at 37 °C. Color development was achieved using a 90 μl TMB substrate solution is added to each well and incubated for 30 min in the dark at 37 °C. Only those wells that contain biotin-conjugated antibody and enzyme-conjugated avidin will exhibit a change in color. The enzyme-substrate reaction is terminated by the addition of 100 μl sulfuric acid solution, and the color change is measured spectrophotometrically at a wavelength of 450 nm ± 2 nm. Serial dilutions of recombinant human KIM-1 were used to establish a standard curve. The detection limit of KIM-1 with this research assay is 31.2–2000 pg/ml. The intra-assay CVs were 4.6% and 6.1% at 253 ± 11.64 and 1220 ± 74.42 pg/ml, respectively. Inter-assay CVs were 6.4% and 7.9% at 317 ± 20.3 and 1458 ± 115.2 pg/ml, respectively.
Urine IL-18 assay was performed according to the following steps; the microtiter plate was coated with monoclonal anti-IL-18 antibody. A total of 100 μl of standards and samples are added to the appropriate microtiter plate and incubated for 90 min at 37 °C .Remove the liquid of each well, add 100 μl of a biotin-conjugated polyclonal anti-KIM-1 antibody to each well, and incubate for 1 h at 37 °C. Aspirate each well and wash with wash buffer, repeating the process three times for a total of three washes, followed by the addition of 100 μl of avidin conjugated to HRP to each microplate and incubated for 30 min at 37 °C. Color development was achieved using a 90 μl TMB substrate solution is added to each well and incubated for 30 min in the dark at 37 °C. Only those wells that contain biotin-conjugated antibody and enzyme-conjugated avidin will exhibit a change in color. The enzyme-substrate reaction is terminated by the addition of 100 μl sulfuric acid solution, and the color change is measured spectrophotometrically at a wavelength of 450 nm ± 2 nm. Serial dilutions of recombinant human IL-18 were used to establish a standard curve. The detection limit of IL-18 with this research assay is 15.6–1000 pg/ml. The intra-assay coefficients of variations (CVs) were 4.3% and 5.5% at 135 ± 5.8 and 762 ± 41.9 pg/ml, respectively. Inter-assay CVs were 5.2% and 5.8% at 141 ± 7.3 and 776 ± 45.1 pg/ml, respectively.
Other measurements
Demographic data, history of any serious comorbidities, diuretic therapy (dose and duration), chronic kidney disease, other causes of liver cirrhosis, shock, documented established parenchymal kidney disease, obstructive uropathy, use of nephrotoxic drugs in the previous 30 days, urinary tract infection, anuria for 12 h, need for renal replacement therapy, solid organ transplantation, history of complications such as hematemesis, melena, hepatic encephalopathy, or spontaneous bacterial peritonitis, and urine output were obtained at enrollment. Complete blood count (CBC) was measured. Another sample on red topped plane tube was used. Serum was separated from whole blood by centrifugation at 3000 rpm for 10 min and was used for measuring albumin, calcium, phosphorus, total cholesterol, triglycerides, urea, creatinine, and uric acid levels. Anti-HCV and HBsAg were detected using ELISA (Sanofi Diagnostic Pasteur, Marne-la-coquette, France), with the use of BIOELISA HCV kit, (BIO kit, SA Barcelona). Complete urine analysis with examination of urine sediment and spot morning protein to creatinine ratio were performed to all patients. Abdominal ultrasonography was done using General Electric Ultrasound, USA, and transducer with a frequency of 3.5 megahertz (MHz).
Estimated GFR (eGFR) was derived using the Modification of Diet in Renal Disease (four variables MDRD equation). The fractional excretion of sodium (FeNa) was calculated by the formula (SCr × UNa)/(SNa × UCr). The fractional excretion of urea (FeUrea) was calculated by the formula (SCr × UUrea)/(SUrea × UCr). We assess the severity of the underlying liver disease by MELD-Na score and Child-Turcotte-Pugh (CPT) score. We assess organ dysfunction, morbidity, and mortality using the sequential organ failure assessment score (SOFA score), APACHE II score, and Glasgow coma scale (GCS).
Statistical analyses
All the analyses were performed with Statistical Package of Social Science (SPSS), version 25. Qualitative data were expressed as frequency (%), and quantitative data were summarized as mean ± standard deviation (SD). Qualitative data were analyzed by chi-square test (χ2) and Fisher exact test as appropriate, while quantitative results were compared with either Student t-test or analysis of variance (ANOVA) followed by Bonferroni correction. Kruskal-Wallis test for nonparametric quantitative data followed by Mann-Whitney test and Dunn-Bonferroni. Also, simple and multiple logistic regression analyses were used to detect independent predictors. For all analyses, statistical significance was defined as p-values ≤ 0.05.
Results
Demographic characteristics of the study groups
Demographic, clinical, and laboratory characteristics of the three groups of patients are shown in Table 1. The three groups were age- and sex-matched.
Urinary biomarkers in study groups
Urinary NGAL, KIM-1, and IL-18 levels are shown in Table 2. Patients with cirrhotic ascites complicated by HRS-AKI (group III) had statistically significant higher levels of all three biomarkers as compared to the other 2 groups (Figs. 1, 2, and 3).

Box plot of urinary NGAL levels according to study groups

Box plot of urinary IL-18 levels according to study groups

Box plot of urinary KIM-1 levels according to study groups
Predictors of hepatorenal syndrome in cirrhotic patients
To evaluate the independent role of each risk factor of HRS-AKI, a simple logistic regression analysis was performed using all parameters that differed significantly between HRS patients and patients without renal impairment as shown in Table 3. It revealed that older age (OR = 1.2, 95 CI = 1.09–1.31, p < 0.001), prolonged hospital stay (OR = 1.83, CI = 1.37–2.44, p < 0.001), lower SBP (OR = 0.89, CI = 0.82–0.96, p = 0.003), lower MAP (OR = 0.88, CI = 0.79–0.97, p = 0.013), encephalopathy (OR = 21, CI = 5.51–79.99, p < 0.001), higher direct bilirubin (OR = 1.66, CI = 1.15–2.41, p = 0.007), higher INR (OR = 4.49, CI = 1.55–13, p = 0.006), higher CHILD score (OR = 2.58, CI = 1.69–3.95, p < 0.001), higher MELD score (OR =1.89, CI = 1.37–2.62, p < 0.001), higher MELD-Na score (OR = 1.87, CI = 1.39–2.5, p < 0.001), higher serum urea (OR = 1.007, CI = 1.001–1.012, p = 0.013), higher serum creatinine (OR = 1.64, CI = 1.17–2.32, p = 0.005), higher NGAL (OR = 1.003, CI =1.001–1.005, p < 0.001), higher KIM-1 (OR = 1.4, CI = 1.12–1.76, p = 0.003), higher IL-18 (OR = 1.05, CI = 1.01–1.09, p = 0.010), higher SOFA score (OR = 2.83, CI = 1.78–4.49, p < 0.001), higher APACHE II score (OR = 1.82, CI = 1.39–2.38, p < 0.001), and lower fractional excretion of sodium (OR = 6.96, CI = 1.6–30.12, p = 0.009).
The diagnostic cutoff values of the different urinary biomarkers
Table 4 and Fig. 4a show the receiver-operating characteristic (ROC) curve analysis of the urinary biomarkers as predictors of HRS-AKI. NGAL with a cutoff value > 125 pg/ml has 100% sensitivity, 100% specificity, PPV 100%, NPV 100%, and 100% accuracy, 95% confidence index was 0.96–1.0, and area under the curve (AUC) was 1 (Fig. 4b). Also, KIM-1 at a cutoff value of > 3.1 pg/ml was found to have 100% sensitivity and 68% specificity and 80% accuracy, confidence index was 0.67–0.86, positive predictive value was 62.5%, negative predictive value was 100%, and area under the curve was 0.780 (Fig. 4c). On the contrary, IL-18 was found to have lower sensitivity (50%), lower specificity (76%), and lower accuracy (66.25%), 95% confidence index was 0.51–0.73, positive predictive value 66, negative predictive value 56, and area under the curve was 0.624 at cutoff value of > 34.8 (Fig. 4d).

a ROC curves of urinary IL-18, urinary NGAL, and urinary KIM-1 for diagnosis of HRS. b ROC curve of urinary NGAL as a diagnostic tool for HRS. c ROC curve of urinary KIM-1 as a diagnostic tool for HRS. d ROC curve of urinary IL-18 as a diagnostic tool for HRS
Value of urinary biomarkers in the diagnosis of stage 1 HRS-AKI
Table 5 and Fig. 5a show the receiver-operating characteristic (ROC) curve analysis of the urinary biomarkers with the use of new diagnostic criteria of HRS. NGAL at cutoff value > 125 pg/mL has 100% sensitivity, 100% specificity, and 100% accuracy, 95% confidence index was 0.96–1.0, and area under the curve was 1 (Fig. 5b). IL-18 at cutoff value of > 34.8 pg/mL has lower sensitivity (51.72%), lower specificity (76%), and lower accuracy (67.09%), 95% confidence index was 0.52–0.74, positive predictive value 55.6, negative predictive value 73.1, and area under the curve was 0.641 (Fig. 5c). KIM-1 at cutoff value of > 3.1 has 100% sensitivity, 68% specificity, and 79.75% accuracy, confidence index was 0.68–0.86, positive predictive value was 64.4%, negative predictive value was 100%, and area under the curve was 0.783 (Fig. 5d).

a ROC curve to evaluate the capability of urinary IL-18, NGAL, and KIM-1 for diagnosis stage 1 AKI. b ROC curve to evaluate the capability of urine NGAL for diagnosis of stage 1 AKI. c ROC curve to evaluate the capability of urinary IL-18 for diagnosis of stage 1 AKI. d ROC curve to evaluate the capability of urinary KIM-1 for diagnosis of stage 1 AKI
Discussion
Acute kidney injury (AKI) is frequent in patients with advanced cirrhosis occurring in up to 20–50% of hospitalized patients. AKI is associated with higher mortality, which increases with increasing severity of AKI [10]. The definition of AKI in cirrhosis has undergone significant changes over the past several years with the use of relative changes in serum creatinine instead of absolute cutoffs due to the limitations of serum creatinine [11]. The incidence of hepatorenal syndrome is increasing and mirrors that of chronic liver disease, but this may be attributed in part to change of diagnostic criteria over time [12].
Early identification of the phenotype of AKI is important as management differs according to the etiology which may affect recovery. One of the most challenging issues in patients with advanced cirrhosis is the ability to differentiate HRS from ATN. Serum creatinine (SCr), creatinine clearance, and SCr-derived equations tend to overestimate GFR in cirrhosis which affect their utility in the early diagnosis of AKI. Conventional tools such as urine output, fractional excretion of sodium or urea, or proteinuria have been shown to have significant limitation in patients with advanced cirrhosis as well as poor correlation with biopsy findings in candidates for liver transplantation [6]. Emerging literature continues to validate and refine the use of functional and damage biomarkers for the diagnosis and prognosis of AKI in liver cirrhosis.
NGAL is a small 25 KDa glycoprotein detected in proliferating nuclear antigen-positive proximal tubular cells. The urine usually does not contain NGAL in significant amounts in healthy individuals, and its appearance in urine indicates either a failure to reabsorb filtered NGAL caused by proximal tubular structural damage or induction of renal tubular NGAL production in more distal tubular injury, as opposed to the functional impairment marked by increases in serum urea, creatinine, and cystatin C [13]. We found that cirrhotic patients with HRS had significantly higher urinary NGAL, compared to cirrhotic patients with normal renal function with or without ascites. Similar results have been reported in patients with cirrhosis and AKI with urinary NGAL higher in patients with impaired kidney function than patients without AKI irrespective of the presence of ascites and are markedly higher in patients with ATN when compared to those with HRS-AKI, prerenal azotemia, or CKD. Urinary NGAL was significantly higher in the subset of patients with HRS-AKI associated with concomitant infections [14]. We demonstrate that urinary NGAL could predict HRS at a cutoff point of > 125 ng/ml. Similar findings have been reported in other studies which demonstrated that patients with HRS had urinary NGAL levels intermediate between prerenal azotemia and intrinsic AKI but with different cutoff points [15, 16]. However, NGAL has several limitations in general and in patients with liver cirrhosis. In general, urinary NGAL level increases during other conditions such as anemia, hypoxia, malignancies, inflammation whether chronic and acute, and CKD [17]. In patients with cirrhosis, NGAL should be interpreted with caution for several reasons. Firstly, NGAL liver synthesis increases during sepsis [18]. Secondly, there is a significant overlap between ATN and HRS groups, which is more pronounced with plasma NGAL levels [14]. Finally, the diagnosis of AKI is based on clinical criteria, as the gold standard of biopsy for AKI diagnosis cannot be used in almost all patients with cirrhosis [19].
Interleukin 18 (IL-18) is a proinflammatory cytokine overexpressed in proximal tubule and released in urine following AKI [20, 21]. We found that patients with HRS-AKI had significantly higher urinary IL-18, compared to cirrhotic patients with normal renal function with or without ascites. Based on the receiver-operating characteristic analysis, at a cutoff point of > 34.8 pg/ml, IL-18 is helpful in diagnosing HRS. In another study of IL-18 in patients with liver cirrhosis but not limited to patients with HRS, they have found significantly higher urinary IL-18 levels in patients with a clinical diagnosis of ATN compared to non-ATN AKI [22].
Kidney injury molecule-1 (KIM-1) is a transmembrane protein, which is upregulated by the renal epithelial cells after ischemic injury [23] and is a marker of proximal tubular injury [24]. We found that patients with HRS had significantly higher urinary KIM-1, compared to cirrhotic patients with normal renal function with or without ascites. Based on receiver-operating characteristic analysis, KIM-1 could predict HRS-AKI at a cutoff point of > 3.1 pg/ml. Previous studies have found that urinary KIM-1 to be increased in patients with ATN but not in those with prerenal AKI, urinary tract infections, or CKD [25]. The role of KIM-1 as a diagnostic biomarker in patients with cirrhosis and AKI has been studied in only few studies which demonstrate increase in urinary KIM-1 levels in ATN as opposed to other causes of AKI [16, 22].
The finding of high levels of the three urinary biomarkers in HRS-AKI observed in our study is in agreement with the emerging data of the presence of parenchymal renal disease before hemodynamic derangements that characterize HRS pathogenesis [26]. This is supported by the finding of reflux of proximal convoluted epithelium into Bowman’s space in 71.4% of cases of HRS [27]. Also, in another study which compares the level of urinary NGAL to the treatment response in patients with cirrhosis and HRS-AKI, they found that complete responders had the lower value of urinary NGAL when compared to partial responders and nonresponders [28]. Finally, up to 21% in one study and 42% in another study of patients with HRS have persistent renal dysfunction after orthotopic liver transplantation, which may reflect the underlying structural abnormality in HRS [29, 30].
We found in this study that the predictors for HRS occurrence in cirrhosis are encephalopathy (OR = 21), higher INR, higher CPT score, higher serum creatinine, higher NGAL, higher KIM-1, higher IL-18, higher SOFA score, higher APACHE2 score, and lower FeNa. These findings may help to invent a risk score for HRS in cirrhotic patients using some or all these variables.
We observed that HRS-AKI patients had higher incidence of SBP than patients with normal renal function. Both HRS and SBP have similar chronologic and pathologic connection, and HRS is precipitated by SBP in 28% of cases despite treatment and resolution of infection. This is due to the release of proinflammatory cytokines and endotoxins that leads to systemic vasodilation secondary to increased production of nitric oxide and other vasodilator substances and decreased cardiac output secondary to sepsis-induced cardiomyopathy [31].
We found that serum sodium is lower in patients with HRS as compared to patients with normal renal function. This finding is in accordance with the study conducted by Angeli and his colleagues who observe that the existence of serum sodium < 135 mmol/L was associated with severe ascites, as indicated by high prevalence of refractory ascites, large fluid accumulation rate, frequent use of large-volume paracentesis, and impaired renal function, compared with normal serum sodium levels. Moreover, low serum sodium levels were also associated with greater frequency of hepatic encephalopathy, spontaneous bacterial peritonitis, and hepatorenal syndrome, but not gastrointestinal bleeding [32]. Hyponatremia was used to support the diagnosis of HRS in the old diagnostic criteria. Hyponatremia in patients with cirrhosis and ascites is an important predictor of mortality associated with lower survival [33] and also an independent predictive factor for the development of hepatic encephalopathy [34].
The current study is limited by the small number of patients. Another important limitation is the lack of serial measurements of the studied biomarkers to assess their impact on response to therapy and outcome. We also correlate the urine biomarkers with serum creatinine which overestimates kidney function in cirrhosis, but there is no consensus statement on accurate measurement of GFR in cirrhotic patients. Moreover, we did not use kidney biopsy to exclude other diagnoses than HRS which up until now is a diagnosis of exclusion.
Conclusion
Urinary neutrophil gelatinase-associated lipocalin, interleukin-18, and kidney injury molecule-1 levels are higher in patients with cirrhotic ascites complicated by HRS-AKI using the new definition of HRS, but IL-18 has lower sensitivity and specificity for the prediction of HRS-AKI as compared to NGAL and KIM-1.
Availability of data and materials
Available
Abbreviations
- NGAL:
-
Neutrophil gelatinase-associated lipocalin
- IL-18:
-
Interleukin-18
- KIM-1:
-
Kidney injury molecule-1
- HCV:
-
Hepatitis C virus
- AKI:
-
Acute kidney injury
- HRS:
-
Hepatorenal syndrome
- ATN:
-
Acute tubular necrosis
- SCr:
-
Serum creatinine
- GFR:
-
Glomerular filtration rate
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- MAP:
-
Mean arterial pressure
- Hb:
-
Hemoglobin
- Hct:
-
Hematocrit
- WBCs:
-
White blood cells
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate transaminase
- INR:
-
International normalized ratio
- CPT:
-
Child-Pugh-Turcotte score
- MELD:
-
Model for end-stage liver disease
- MELD-Na:
-
Model for end-stage liver disease-sodium
- Na:
-
Serum sodium
- K:
-
Serum potassium
- FeNa :
-
Fractional excretion of sodium
- FEUrea :
-
Fractional excretion of urea
References
Thapa P, Kc S, Hamal AB, Sharma D, Khadka S, Karki N et al (2020) Prevalence of acute kidney injury in patients with liver cirrhosis. JNMA J Nepal Med Assoc 58(228):554–559
Wong F (2012) Recent advances in our understanding of hepatorenal syndrome. Nat Rev Gastroenterol Hepatol 9(7):382–391
Garcia-Tsao G, Parikh CR, Viola A (2008) Acute kidney injury in cirrhosis. Hepatology 48(6):2064–2077
Alessandria C, Ozdogan O, Guevara M, Restuccia T, Jimenez W, Arroyo V et al (2005) MELD score and clinical type predict prognosis in hepatorenal syndrome: relevance to liver transplantation. Hepatology 41(6):1282–1289
Singh V, Ghosh S, Singh B, Kumar P, Sharma N, Bhalla A et al (2012) Noradrenaline vs. terlipressin in the treatment of hepatorenal syndrome: a randomized study. J Hepatol 56(6):1293–1298
Francoz C, Glotz D, Moreau R, Durand F (2010) The evaluation of renal function and disease in patients with cirrhosis. J Hepatol 52(4):605–613
Slocum JL, Heung M, Pennathur S (2012) Marking renal injury: can we move beyond serum creatinine? Transl Res 159(4):277–289
Wong F, Nadim MK, Kellum JA, Salerno F, Bellomo R, Gerbes A et al (2011) Working party proposal for a revised classification system of renal dysfunction in patients with cirrhosis. Gut 60(5):702–709
Tsien C, Wong F (2013) The impact of acute kidney injury in cirrhosis: does definition matter? Gut 62(7):1091–1092
Tandon P, James MT, Abraldes JG, Karvellas CJ, Ye F, Pannu N (2016) Relevance of new definitions to incidence and prognosis of acute kidney injury in hospitalized patients with cirrhosis: a retrospective population-based cohort study. PLoS One 11(8):e0160394
Angeli P, Gines P, Wong F, Bernardi M, Boyer TD, Gerbes A et al (2015) Diagnosis and management of acute kidney injury in patients with cirrhosis: revised consensus recommendations of the International Club of Ascites. J Hepatol 62(4):968–974
Pant C, Jani BS, Desai M, Deshpande A, Pandya P, Taylor R et al (2016) Hepatorenal syndrome in hospitalized patients with chronic liver disease: results from the Nationwide Inpatient Sample 2002-2012. J Investig Med 64(1):33–38
Devarajan P (2014) NGAL for the detection of acute kidney injury in the emergency room. Biomark Med 8(2):217–219
Fagundes C, Pepin MN, Guevara M, Barreto R, Casals G, Sola E et al (2012) Urinary neutrophil gelatinase-associated lipocalin as biomarker in the differential diagnosis of impairment of kidney function in cirrhosis. J Hepatol 57(2):267–273
Verna EC, Brown RS, Farrand E, Pichardo EM, Forster CS, Sola-Del Valle DA et al (2012) Urinary neutrophil gelatinase-associated lipocalin predicts mortality and identifies acute kidney injury in cirrhosis. Dig Dis Sci 57(9):2362–2370
Qasem AA, Farag SE, Hamed E, Emara M, Bihery A, Pasha H (2014) Urinary biomarkers of acute kidney injury in patients with liver cirrhosis. ISRN Nephrol 2014:376795
Martensson J, Bellomo R (2014) The rise and fall of NGAL in acute kidney injury. Blood Purif 37(4):304–310
Macdonald SP, Stone SF, Neil CL, van Eeden PE, Fatovich DM, Arendts G et al (2014) Sustained elevation of resistin, NGAL and IL-8 are associated with severe sepsis/septic shock in the emergency department. PLoS One 9(10):e110678
Ostermann M, Joannidis M (2015) Biomarkers for AKI improve clinical practice: no. Intensive Care Med 41(4):618–622
Ariza X, Sola E, Elia C, Barreto R, Moreira R, Morales-Ruiz M et al (2015) Analysis of a urinary biomarker panel for clinical outcomes assessment in cirrhosis. PLoS One 10(6):e0128145
Liu Y, Guo W, Zhang J, Xu C, Yu S, Mao Z et al (2013) Urinary interleukin 18 for detection of acute kidney injury: a meta-analysis. Am J Kidney Dis 62(6):1058–1067
Belcher JM, Sanyal AJ, Peixoto AJ, Perazella MA, Lim J, Thiessen-Philbrook H et al (2014) Kidney biomarkers and differential diagnosis of patients with cirrhosis and acute kidney injury. Hepatology 60(2):622–632
Ichimura T, Bonventre JV, Bailly V, Wei H, Hession CA, Cate RL et al (1998) Kidney injury molecule-1 (KIM-1), a putative epithelial cell adhesion molecule containing a novel immunoglobulin domain, is up-regulated in renal cells after injury. J Biol Chem 273(7):4135–4142
Han WK, Bailly V, Abichandani R, Thadhani R, Bonventre JV (2002) Kidney injury molecule-1 (KIM-1): a novel biomarker for human renal proximal tubule injury. Kidney Int 62(1):237–244
Parikh CR, Devarajan P (2008) New biomarkers of acute kidney injury. Crit Care Med 36(4 Suppl):S159–S165
Deshpande P, Rausa K, Turner J, Johnson M, Golestaneh L (2011) Acute kidney injury as a causal factor in mortality associated with hepatorenal syndrome. Hepatol Int 5(3):751–758
Kanel GC, Peters RL (1984) Glomerular tubular reflux--a morphologic renal lesion associated with the hepatorenal syndrome. Hepatology 4(2):242–246
Cavallin M, Fasolato S, Marenco S, Piano S, Tonon M, Angeli P (2015) The treatment of hepatorenal syndrome. Dig Dis 33(4):548–554
Nadim MK, Sung RS (2012) Living donor liver transplantation for hepatorenal syndrome: to do or not to do? That is the question. Liver Transpl 18(10):1138–1139
Marik PE, Wood K, Starzl TE (2006) The course of type 1 hepato-renal syndrome post liver transplantation. Nephrol Dial Transplant 21(2):478–482
Wadei HM, Mai ML, Ahsan N, Gonwa TA (2006) Hepatorenal syndrome: pathophysiology and management. Clin J Am Soc Nephrol 1(5):1066–1079
Angeli P, Wong F, Watson H, Gines P, Investigators C (2006) Hyponatremia in cirrhosis: results of a patient population survey. Hepatology 44(6):1535–1542
Kim WR, Biggins SW, Kremers WK, Wiesner RH, Kamath PS, Benson JT et al (2008) Hyponatremia and mortality among patients on the liver-transplant waiting list. N Engl J Med 359(10):1018–1026
Guevara M, Baccaro ME, Torre A, Gomez-Anson B, Rios J, Torres F et al (2009) Hyponatremia is a risk factor of hepatic encephalopathy in patients with cirrhosis: a prospective study with time-dependent analysis. Am J Gastroenterol 104(6):1382–1389
Acknowledgements
We thank our colleagues from Internal Medicine Department who provided insight and expertise that greatly assisted the research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
MAAM contributed to the design of the study, interpretation of the data of the work, and reviewing the final manuscript; YZM contributed to the design of the work and reviewing of data; HKHK contributed to the design of the study, interpretation of data, drafting and revising of the work, and corresponding author. MMM contributed to the performance of laboratory work, data acquisition, and review; SMME was responsible for collection of samples and preparation of data. All authors critically revised the manuscript, agreed to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The research was conducted in accordance with the ethical standards of Minia University committee on human experimentation and with Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
El-Makarem, M.A.ER.A., Mahmoud, Y.Z., Moussa, M.M. et al. Do old urinary biomarkers have a place in the new definition of hepatorenal syndrome in the Egyptian cirrhotic patients? A single-center experience. Egypt Liver Journal 12, 23 (2022). https://doi.org/10.1186/s43066-022-00185-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43066-022-00185-0