
Abstract
Background
CBCT is widely used in dentistry and is used for a variety of purposes. The presence of different artifacts can reduce the quality of images. Since the implants mainly contain metals, they can cause many artifacts in CBCT images. Due to the importance of CBCT and the effects of artifacts on the final image quality, this study was conducted to investigate the effect of FOV size on the artifacts.
Methods
Three human skulls with unbroken mandible and maxilla were selected. CBCT images were prepared under normal exposure conditions and with three ranges of FOV (4 × 5 cm2, 5 × 8 cm2, 8 × 8 cm2). Then an implant was placed in the empty dental sockets in the incisor, canine, and premolar areas, and CBCT images were taken with similar conditions. The Hounsfield Unit obtained before and after implant placement was compared, and their difference was considered as metal artifact. Data were analyzed using two-factor variance analysis.
Results
In this study, the mean difference of artifacts with a large FOV in both jaws and in the mandible for medium and small radiation ranges from the central to the premolar side was always decreasing. However, in the maxilla for the medium and small radiation ranges, the mean difference increased from the central side to the canine, but again decreased relatively significantly from the canine to the premolar. The mean interaction between the dental areas and the FOV sizes was not significant (p = 0.997), and it was found that the amount of artifacts in the studied areas does not change with changing the size of the FOV. Also there was no significant difference of artifacts between the three types of FOV size (p = 0.730), but there was a significant difference between the dental areas (p = 0.020).
Conclusions
According to the findings of this study, it can be concluded that the amount of metal artifacts is not related to the size of FOV. However, it is related to the position of the implant in the jaws and the density of the surrounding tissues.
Similar content being viewed by others

Background
CBCT is a new imaging technique that was first introduced in 1982 and was first used for angiography and later for maxillofacial imaging. CBCT has been introduced in dentistry as an alternative to CT [1]. The cone beam technique involves simultaneous movements around the patient's head by an X-ray source with an angle of more than 180 degrees and intermittent movements of the surface detector. During rotation, many images are captured by the device at regular intervals, which are called base images. The complete set of base images is read as radiation data. Software programs with a special algorithm including backfiltered projection are applied to the radiation data to produce a series of three-dimensional volumetric information that can be used to provide initial reconstruction images in three orthogonal planes (axial, sagittal, and coronal) [2]. Numerous factors such as FOV, quality and quantity of X-ray cone, pixel size, and jaw arch affect the final CBCT image and image features such as noise, resolution contrast, and artifacts [3]. The use of implants in the reconstruction of complete and partial edentulousness improves masticator performance and increases patient satisfaction compared to removable or fixed dentures. As a result, this treatment has grown exponentially in recent decades [4]. The goal of modern dentistry is to restore comfort, physiological function, beauty and health to patients who have lost their teeth [5]. Today, the use of CBCT imaging is very widespread and is used for a wide variety of diagnostic purposes. Various factors can affect the final quality of CBCT images. The presence of different artifacts in CBCT can affect the quality and sometimes makes diagnosis difficult. Because implants are mainly made of metal, CBCT examinations can create many metal artifacts. Various factors and solutions have been proposed to reduce the artifacts [6].
E. Costa et al. investigated the effect of radiation range on metal artifacts. They concluded that images scanned with a larger FOV had higher noise and quality loss [7]. In the study of R.Pauwels et al., the amount of metal artifacts in different CBCT devices and with different exposure protocols was investigated. They concluded that in some cases the use of high-dose protocols and the selection of large FOVs reduce the amount of artifacts [8]. Panjnoush et al. [9] and Codari et al. [10] concluded that the type of metal has the greatest impact on the amount of metal artifacts. Shokri et al. [11] concluded that the rate of artifacts was lower in small FOVs.
Given the importance of CBCT images as well as the effect of artifacts on the image quality, this study was performed to investigate the effect of field of view (FOV) size and different dental areas on the amount of dental implant artifacts in CBCT images.
Methods
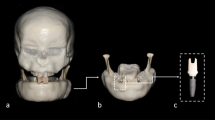
This study was performed in the radiology department of Mashhad Dental School. Three dry human skulls with healthy mandible and maxilla with at least one empty cavity in the central, canine, and second premolar areas were borrowed from the anatomy department of the medical school for implant placement. Exclusion criteria included fractures of the skulls during preparation and lack of suitable dental cavity for implant placement. To simulate soft tissue in imaging, the buccal surface of the maxilla and mandible was covered with two layers of soft rose gold wax [9]. The mandibular condyle was also fixed in glenoid fossa with adhesive tape. The skull was then fixed on a support plate. In the CBCT machine, the Frankfurt plan was placed parallel to the ground and the two jaws were adjusted in FOV with the help of guidelines.
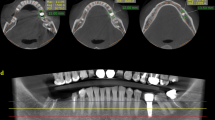
CBCT images in normal exposure conditions including 14 mA, 84 kVP, and voxel size = 160 with three types of FOV radiation ranges (small: 5 × 4 cm2, in each toothless area, medium: 5 × 8 cm2, for each jaw and large: 8 × 8 cm2 for both jaws) were prepared. In this study, CBCT Planmeca Promax classic device was used. A Luna South Korea dental implant was placed separately in the empty spaces, and CBCT was prepared again with the mentioned conditions. A total of 54 CBCT images of three skulls were taken. In this way, at first, the sagittal line was completely adjusted in the middle of the skull and the image in the sagittal section was adjusted so that the axial plane passes through the PNS and ANS. The sagittal plane was then adjusted with the middle of the mesial dental socket of the area to be implanted. Then, in the axial section, 6 cuts with a distance of 1 mm from each other and a thickness of 0.5 mm were selected and adjusted so that the most gingival cut corresponds to the edge of the bone crest in the sagittal view (Fig. 1). Then, on each of the 6 images in the axial view, the desired sac was selected (mesial dental socket of the implant) (Fig. 2). After selection on all 6 images, the average HU in volume was obtained using Romexis viewer software (Figs. 3, 4). The difference between the HU obtained before and after implant placement in exact same place, which indicates the added metal artifact after placement of the implant, was measured in three size of FOV using and compared with each other. Initially, the measurements in 16% of CBCT images were repeated twice and compared. Measurement error was low and acceptable. Data analysis was performed using two-way analysis of variance (FOV and region). Significance level in statistical tests was considered equal to 5%.

Adjusting the cuts

Selection of the study area in 6 axial images

Hounsfield Unit in axial images

Hounsfield Unit in different plans
Results
In this study, which was performed on 3 skulls, central, canine, and premolar areas were selected and CBCT images were taken from each part with small, medium, and large FOVs. Then implants were placed in the same areas, and exactly the same images were taken as before. Then, the Hounsfield Unit obtained in the images before and after implant placement was compared and their differences were measured. The data distribution of quantitative variables was examined for normality. The result is given in Table 1. As can be seen, HU differences had a normal distribution in all regions and ranges of radiation, so this issue was considered in data analysis. All the data obtained for 6 areas in each of the 3 evaluated skulls with 3 different FOV sizes are listed in Table 2 compared. Then, the difference in HU between the dental areas and the FOV size was compared. Table 3 shows the number, mean, and standard deviation of the HU difference variable by dental areas and radiation range. As can be seen, in both jaws with a large FOV, the mean difference of HU from the central to the premolar side was always decreasing. This was also true in the mandible for medium and small radiation ranges. However, the mean difference of HU in the maxilla for the medium and small radiation ranges, increased from the central side to the canine, but again decreased relatively significantly from the canine to the premolar. The mean interaction between the dental area and the FOV sizes was not significant (p = 0.997), and it was found that the amount of artifacts in the studied areas does not change with changing the size of the FOV. Also there was no significant difference between the three types of FOVs (p = 0.730), but there was a significant difference between the dental areas (p = 0.020). According to Table 3, the highest amount of artifacts was observed in the lower central region and the lowest amount of artifacts was observed in the premolars (posterior) of the maxilla. According to Table 4, comparing the two groups in terms of the mean variable of bone density difference, it was found that the mean difference in the lower central tooth was significantly higher than all other areas except the canine tooth. Also, the mean difference in the lower canine tooth area was significantly higher than the upper premolars. But there was no significant difference between other teeth.
The summary of Tables 3 and 4 can be seen more clearly in Fig. 5. The first half of the table on the left represents the central, canine, and maxillary premolars, respectively. From the first point (central) to the second point (canine), the blue line, which indicates the large radiation range, is descending, and the Hounsfield Unit difference, which represents the amount of artifact, is reduced, but in the two lines, which are the medium radiation range, the yellow line for the small radiation range is ascending. Of course, as can be seen in the graph, this increase is very small.

Mean difference of Hounsfield Unit by dental areas and radiation range
In general, the difference in HU in the mandible is greater than in the maxilla, and changes from anterior to posterior in the mandible are more pronounced than in the maxilla. This may be due to differences in bone structure and the location of the sockets relative to each other.
Discussion
In this study, three areas including central, canine, and second premolar were identified and CBCT images were taken from each of them with small, medium, and large FOV. Then implants were placed in the same areas, and exactly the same images were taken as before. Then, the Hounsfield Unit obtained in the images before and after implant placement, in exact same place, was compared and their differences were obtained. This number was related to different FOVs in each area. In this study, it was found that in all studied areas, the amount of artifact does not change with changing the size of the FOV. Also, with large FOVs in both jaws, the Hounsfield Unit decreases from central to premolars, but with small and medium FOVs, this trend is only true for the mandible. The mean interaction between dental areas and FOV size was not significant but was significant between different areas. The highest rate of artifacts was observed in the lower central region, and the lowest rate of artifacts was observed in the premolars (posterior) of the maxilla.
FOV size is different and adjustable between different devices [12], which is one of the most important factors in determining the image quality and received dose by the patient [13]. In this study, no significant difference was observed in the amount of artifacts due to the presence of dental implants between different FOVs.
Shokri et al. [11] investigated the effect of exposure parameters such as FOV and milliampere on the amount of metal artifacts caused by oral implants. Unlike our study, they found that at smaller FOVs, the amount of metal artifacts around the oral implants was lower. The reason for the difference could be due to the use of bone blocks placed in the wax, unlike the present study, which implanted implants on a human skull. As in the present study, the study of Queiroz et al. [14] as well as the study of Codari et al. [10] stated that the size of FOV has no effect on the change of metal artifacts. In the study, Parsa et al. [13] investigated the imaging parameters with two different CBCT devices on the amount of metal artifacts. In Accuitomo 170®, Morita, Japan, with increasing FOV, the density difference increased, but in NewTom 5G®, QR, Verona, Italy, with increasing FOV, the density difference decreased, although this difference between the two devices was not significant. The difference between the results of this research and our research may be due to the differences between the studied devices and the program used for image processing. In the study, Costa et al. [7] investigated the effect of scan mode (full rotation or partial) and FOV size on the formation of artifacts in CBCT. Larger FOVs showed more image noise than smaller FOVs; the reason for the difference could be the use of the phantom in this study, as well as different settings and the use of different CBCT devices. They also examined the amount of noise, while in the present study the amount of metal artifacts was measured. In the study of Pauwels et al. [8] that was stated that in general, using high-dose protocols and larger FOV, there was no improvement in the amount of metal artifacts. Machado et al. [15] concluded that the rate of artifacts in the mandible as well as in the anterior is higher, which are similar to the present study. In various studies, in addition to the effect of FOV, the effects of other items such as kVp, amp, and time were also investigated. The effect of kVp seems to be more important than other factors (14, 40–42), although the effect of amp on the amount of metal artifacts did not have a significant effect in the studies of Chindasombatjareon, Pauwelse, and Shokri [8, 11, 16]. According to the results of this study and similar studies, FOV size has no significant effect on the amount of artifacts caused by dental implants. Due to this issue, it is concluded that when adjusting the FOV for CBCT imaging, reducing the received dose by the patient along with a complete imaging of the study area should be considered. Due to the creation of more metal artifacts in the anterior areas of the jaw, especially in the mandible, the use of artifact reduction methods such as creating a distance between the teeth of the two jaws and also creating a distance between the lips and teeth and proper kVp adjustment can be helpful. The above results can help the clinician to achieve better results in order to make better adjustments to achieve better results.
Limitations and future work
One of the limitations of the present study is that due to the impossibility of imaging on living models, it was not possible to evaluate the effect of the patient’s natural soft tissue and the artifact caused by its presence. The use of one CBCT device model is another limitation of the study. It is recommended to use different CBCT devices from different manufacturers. In addition to the study of artifacts from oral implants, metal artifacts from different restorative materials and different types of implants can also be effective in better studies.
Conclusions
According to the findings of this study, it can be concluded that the amount of metal artifacts is not related to the amount of FOV. Due to this issue, it is concluded that when adjusting the FOV for CBCT imaging, the reduction of the patient's dose should be considered along with the complete imaging of the study area. Also, the amount of metal artifacts is related to the density of surrounding tissues and bones and is higher in the anterior region of the jaws.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CBCT:
-
Cone beam computed tomography
- FOV:
-
Field of view
- HU:
-
Hounsfield Unit
- KVP:
-
Peak kilovoltage
References
Hassan B, Jacobs R (2008) Cone beam computed tomography-3D imaging in oral and maxillofacial surgery. Eur Med Imaging Rev 1(1):38–40
Brüllmann D, Schulze R (2015) Spatial resolution in CBCT machines for dental/maxillofacial applications—What do we know today? Dentomaxillofac Radiol 44(1):20140204
Pauwels R et al (2015) Technical aspects of dental CBCT: state of the art. Dentomaxillofac Radiol 44(1):20140224
Buser D et al (2012) 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: a retrospective study in 303 partially edentulous patients. Clin Implant Dent Relat Res 14(6):839–851
Přikrylová J, Procházková J, Podzimek Š (2019) Side effects of dental metal implants: impact on human health (metal as a risk factor of implantologic treatment). BioMed Res Int 2019:2519205
Gaviria L et al (2014) Current trends in dental implants. J Korean Assoc Oral Maxillofac Surg 40(2):50–60
Costa EDD et al (2019) Influence of scan mode (partial/full rotations) and FOV size in the formation of artefacts in cone beam CT. Dentomaxillofac Radiol 48(4):20180340
Pauwels R et al (2013) Quantification of metal artifacts on cone beam computed tomography images. Clin Oral Implant Res 24:94–99
Panjnoush M et al (2016) Effect of exposure parameters on metal artifacts in cone beam computed tomography. J Dent (Tehran, Iran) 13(3):143
Codari M et al (2017) Quantitative evaluation of metal artifacts using different CBCT devices, high-density materials and field of views. Clin Oral Implant Res 28(12):1509–1514
Shokri A et al (2019) Effect of exposure parameters of cone beam computed tomography on metal artifact reduction around the dental implants in various bone densities. BMC Med Imaging 19(1):1–10
Hatcher DC (2010) Operational principles for cone-beam computed tomography. J Am Dent Assoc 141:3S-6S
Parsa A et al (2013) Influence of cone beam CT scanning parameters on grey value measurements at an implant site. Dentomaxillofac Radiol 42(3):79884780
Queiroz PM et al (2017) Evaluation of the efficacy of a metal artifact reduction algorithm in different cone beam computed tomography scanning parameters. Oral Surg Oral Med Oral Pathol Oral Radiol 123(6):729–734
Machado AH et al (2018) Effect of anatomical region on the formation of metal artefacts produced by dental implants in cone beam computed tomographic images. Dentomaxillofac Radiol 47(1):20170281
Chindasombatjaroen J et al (2011) Quantitative analysis of metallic artifacts caused by dental metals: comparison of cone-beam and multi-detector row CT scanners. Oral Radiol 27(2):114–120
Acknowledgements
This research was presented in the Organizational Ethics Committee of the Faculty/Regional of Mashhad University of Medical Sciences under the title “Investigation of the effect of radiation range (Field Of View) on the amount of dental implant artifacts in CBCT images” and with number 980669 and code IR.MUMS.DENTISTRY.REC 1398.100 has been approved.
Funding
The Research Deputy of Mashhad University of Medical Sciences financially supported this research.
Author information
Authors and Affiliations
Contributions
SM contributed as a research assistant as well as a technical advisor. ZK and MP were a major contributor to image analyzing and writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mortazavi, S., Khadem-Reza, Z.K. & Parvaresh, M. Investigation of the effect of field of view on the amount of dental implant artifacts in cone beam computed tomography images. Egypt J Radiol Nucl Med 55, 100 (2024). https://doi.org/10.1186/s43055-024-01274-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01274-3