
Abstract
Background
Lingual abscess corresponds to an infection that manifests itself as a painful swelling in the tongue with purulent material inside. This is a rare entity and the information available in the literature is limited and based on clinical case reports. Therefore, the diagnosis, etiology, clinical manifestations, and treatment are not fully defined.
Case presentation
The aim of this work was to describe the imaging of a case of lingual abscess, focusing on imaging evaluation using ultrasound and computed tomography (CT), and comparing the diagnostic utility of both modalities in smaller lingual abscesses. This case was treated with antibiotics and adequate drainage was performed, with good evolution.
Conclusions
Tongue abscess is a rare pathology due to the various mechanisms that the tongue has to avoid infections; however, it is a diagnosis that we must consider. CT may be sufficient to diagnose it on imaging, but in smaller lesions, ultrasound with a high-frequency transducer provides more information.
Similar content being viewed by others


Background
Lingual abscess is an infrequent pathology since lesions on the tongue rarely become infected. Therefore, it is an entity with limited information in the literature, which comes mainly from clinical case reports [1].
Clinical manifestations and physical examination are quite nonspecific; consequently, imaging support is essential for proper diagnosis and timely treatment [2]. We present a clinical case in which the image was crucial to define a course of action but unlike what has been reported in other cases, the computed tomography was suggestive but not conclusive, and the ultrasound ended up defining the diagnosis.
The aim of this study is to describe a case of lingual abscess in a patient, focusing on imaging evaluation using ultrasound and computed tomography (CT), and comparing the diagnostic utility of both modalities in smaller lingual abscesses.
Case presentation
This was the case of a 24-year-old male patient, of Caucasian origin, university student, with no diseases, no history of immunosuppression, or other personal history of interest, presented with progressive pain on the right lateral border of the tongue for five days, accompanied by swelling for two days. The patient reported no history of trauma or previous wounds. During his initial evaluation, a lingual tumor was suspected, and he was treated with oral corticosteroids and analgesics which provided slight relief of his symptoms, pending deferred laboratory testing and evaluation by a specialist to define medical conduct. However, a day later, the patient experienced persistent swelling and a recurrence of pain. On physical examination, a reactive right submandibular lymphadenopathy was palpable and erythema stood out on the lingual mucosa of the right lateral border associated with an indurated painful area. A contrasted CT scan of the neck was requested, which showed nonspecific tongue lesion in the affected area (Fig. 1). It was suggested to characterize it with a tongue ultrasound. The examination was performed with a high-frequency linear transducer (22 MHz) and a small surface or “hockey stick” type, which allowed specific sectors to be better evaluated by providing high-resolution images, which were compatible with an abscess in formation, measuring approximately 9 × 8 × 5 mm (Fig. 2).

Computed tomography (CT) scan of the neck with intravenous contrast: showed hypodense area outlined by a slightly hyperdense area on the contrast. The lesion was not well defined and was inconclusive

Ultrasound with high-frequency transducer (24 MHz): showed marked inflammatory signs of the lateral edge of the tongue were evident, with a thickening of the mucosa and increased volume of the surrounding tissue. A partially delimited heterogeneous hypoechoic content collection was depicted (A), without vascularization or foreign body (B), with characteristics of an abscess in formation
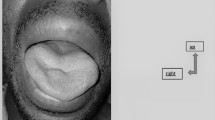
The therapeutic decision to start antibiotic treatment with intravenous ampicillin—sulbactam was made, followed by the oral overlap to amoxicillin—clavulanic acid until completing 10 days. After 48 h, an opening of the abscess was observed on physical examination and samples were taken for culture (Fig. 3). In the culture, there was development of a variety of gram-positive cocci (streptococci) corresponding to the usual bacterial microbiota. Five days later, a clear remission of the lingual abscess was evident and the laboratory only showed elevation of inflammatory parameters that normalized after treatment, and since there were no longer inflammatory signs or symptoms, clinical follow-up was decided without a new image, concluding in a medical discharge.

Purulent content was drained with digital pressure (48 h after starting antibiotic therapy)
Discussion
Lingual abscess is an unusual condition characterized by infection and accumulation of purulent material within the tongue. Despite being a rare entity, it presents diagnostic challenges due to limited literature and clinical reports [2, 3]. Our case report aimed to elucidate the imaging characteristics of a lingual abscess using both ultrasound and computed tomography (CT), highlighting the efficacy of ultrasound in cases where CT findings may be inconclusive, particularly in smaller abscesses.
The aim of this study is to describe a case of lingual abscess in a patient, focusing on imaging evaluation using ultrasound and computed tomography (CT), and comparing the diagnostic utility of both modalities in smaller lingual abscesses.
Comparative analysis with previously reported cases reveals a distinct feature of our case: the smaller size of the abscess [3,4,5]. In contrast to larger abscesses where CT imaging has proven more informative, our case illustrates the limitations of CT in visualizing smaller lesions. This discrepancy underscores the importance of utilizing alternative imaging modalities such as ultrasound, especially in cases where CT fails to provide definitive diagnostic clarity.
The diagnostic challenge posed by lingual abscesses lies in their varied etiology and clinical presentation. While trauma, foreign bodies, and dental diseases are commonly associated with abscess formation [2, 6, 7], identifying the exact cause can be elusive. Additionally, the tongue's robust vascular supply and muscular structure often mitigate the development of infections, further complicating diagnosis [3, 5].
In our case, initial suspicion of a lingual tumor prompted CT imaging, which yielded inconclusive results. Subsequent ultrasound examination with a high-frequency transducer provided clearer visualization of the abscess, facilitating accurate diagnosis and guiding therapeutic intervention. This highlights the complementary role of ultrasound in cases where CT fails to provide definitive diagnostic insight, particularly in smaller abscesses where resolution may be limited [3, 8].
Comparative studies with larger lingual abscesses underscore the diagnostic challenges posed by size discrepancies. While CT imaging remains a valuable tool in diagnosing larger abscesses, our case demonstrates the utility of ultrasound in smaller lesions, where higher resolution and clearer delineation of abscess boundaries are essential for accurate diagnosis and treatment planning. Therefore, lingual abscesses present diagnostic challenges, particularly in cases where imaging findings may be inconclusive. Our case highlights the efficacy of ultrasound in visualizing smaller abscesses, complementing CT imaging and facilitating accurate diagnosis and treatment. Further research and comparative studies are warranted to elucidate the optimal diagnostic approach for lingual abscesses of varying sizes.
Conclusions
Lingual abscess is a rare entity due to the various mechanisms that the tongue has to avoid infections; however, it is a diagnosis that we must consider. Treatment is mainly based on draining the contents and antibiotics. Although the diagnosis may be clinical, laboratory tests, fluid culture, and images may be necessary to confirm this pathology. In large lesions with suggestive symptoms, CT imaging may be sufficient, but in smaller lesions, ultrasound with a high-frequency transducer provides more information. In any case, follow-up is necessary to observe the evolution of the injury.
Availability of data and materials
Not applicable. If your manuscript does not contain any data, please state 'Not applicable' in this section.
Abbreviations
- CT:
-
Computed tomography
References
Little CC, Filimonov A, Schwam ZG (2022) Lingual abscess: a case report of a rare clinical entity. Otolaryngol Case Rep 23(100411):100411
Laguía M, Lahoz MT, Martínez J, Amieva M (2008) Abscesses of lingual base: our experience. ORL Aragon 6(2):20–22
Balatsouras DG, Eliopoulos PN, Kaberos AC (2004) Lingual abscess: diagnosis and treatment. Head Neck 26(6):550–554
Sánchez Barrueco Á, MelchorDíaz MA, Jiménez Huerta I, Millán Juncos JM, AlmodóvarÁlvarez C (2012) Absceso lingual recurrente. Acta Otorrinolaringol Esp 63(4):318–320
Kulkarni CD, Verma AK, Kanaujia R (2013) A rare case of hemilingual abscess in a 17-year-old girl: the ease of ultrasound and the advantage of MRI. Jpn J Radiol 31(7):491–495
Chyau Hong W, Shiun CC (2021) Tongue abscess: delayed diagnosis of a foreign body in the tongue. Clin Med Rev Case Rep 8(5):347
Srivanitchapoom C, Yata K (2018) Lingual Abscess: predisposing factors, pathophysiology, clinical manifestations, diagnosis, and management. Int J Otolaryngol 2018:e4504270
Solomon DM, Hahn B (2012) Lingual abscess. J Emerg Med [Internet] 43(1):e53–e54
Acknowledgements
To the Imaging Department of the Clínica Alemana de Santiago for helping us obtain the images.
Funding
The authors declare that there were no external funding sources.
Author information
Authors and Affiliations
Contributions
OC gathered the information from the case and the participants and largely contributed to the writing of the text. RA took the ultrasound, selected the images, and wrote what was related to ultrasound. FS performed most of the literature search and drafted much of the manuscript. CW performed final review and modifications of the text and selected the most appropriate images. LF was the patient's initial treatment and wrote the clinical history and management, and also requested the patient’s consent. PP was the treater who followed up the patient and who took the photograph of the drained abscess, wrote the description of the follow-up and its photograph.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The publication was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Ethics Committee of the Faculty of Medicine of the Universidad del Desarrollo—Clínica Alemana de Santiago.
Consent for publication
We obtained the patient’s informed consent for this publication in writing.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Campos, O., Aris, R., Santorcuato, F. et al. Imaging in lingual abscess: a case report. Egypt J Radiol Nucl Med 55, 83 (2024). https://doi.org/10.1186/s43055-024-01255-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01255-6