
Abstract
Background
Accurate measurement of the femoral neck shaft angle (NSA) is critical for the diagnosis and treatment of hip pathology, but its current reference values remain limited in the Egyptian adult population. This study was designed to provide reference that is reliable for femoral NSA measured by computed tomography (CT) in Egyptian healthy adults of both sexes. This was a cross-sectional descriptive study and analysis of the femoral NSA of healthy Egyptian adults of both sexes measured by CT. Six hundred hips in 300 adults (aged 18 and 60 years; 300 females) were evaluated in the simulated anterior pelvic plane (APP) and the rotation-corrected coronal reconstruction femoral neck plane (FNP) on both sides. We compared the measurements with age and sex, and a two-tailed nonparametric Wilcoxon test was used to discover differences between both measurements.
Results
The mean NSA was 129.46° ± 5.06°, with a mean value of 129.65° ± 4.13° for males and 129.28° ± 3.71° for females. Simulated APP had a higher mean NSA 129.6° (range 115.7°–146.7°; SD 5.06°) than rotation-corrected coronal reconstruction in the FNP 127.73° (range 115.3°–144.6°; SD 4.9°). It was observed that there was a significant variation in the measurements of NSA between the two methods. The side influenced the NSA significantly on both views (p < 0.001); no significant differences were found between age and gender.
Conclusions
The current study attempts to develop population-specific data for femoral NSA reference values in Egyptian communities. No considerable difference was measured in NSA among males and females. It was observed that there was a side difference, with the NSA value being higher on the left than the right. We noted also that proper measurement of NSA is made possible by using NSA values obtained from rotation-corrected coronal reconstruction in the FNP. We anticipate that the findings will contribute to a better understanding of proximal femur morphology and may aid the majority of our population in selecting an implant that is compatible with hip anatomy.
Similar content being viewed by others
Background
For the diagnosis of hip joint disorders and preoperative planning of total hip arthroplasty, accurate measurement of the femoral neck shaft angle (NSA) is crucial [1]. Several scholars from different countries throughout the world have researched the femoral NSA. Variations have been observed, which are explained by variable levels of activity, genetics, race, nutrition, and lifestyle [2]. This vast range of values demonstrates the urgent need for population-based research on this crucial aspect. Reference values for the NSA in adults are currently only available based on measurements taken from simple radiographs or a sparse collection of anatomical samples [3]. The accuracy and dependability of the NSA assessed on plain anteroposterior radiographs have been called into question, nevertheless, because of rotational impacts and erroneous placement of the femoral shaft and neck axis [4].
In addition, the current reference that is available refers to the NSA in adults and is based on western data measurements. Western data are used to create commercially viable hip joint prostheses, whose biomechanical and constitutional variables differ from those of Egyptian patients [5]. As a result, an ill-fitting hip prosthesis can have an impact on these functions. To develop a stronger bone plate structure, a better contour fit for the bone and plate is required [6]. This study was conducted to determine the value of the NSA of Egyptian healthy adults for the purpose of adequate planning, preparation, and preoperative selection of orthopedic implants for surgery in hospitals located in countries like Egypt. The target of the survey was to add reference values for NSA in Egyptian patients based on the analysis of hip rotation-corrected computed tomography (CT) scans and then to correlate these results with simulated AP pelvic radiographs.
Methods
Study design
This retrospective study was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cross-sectional studies [7]. All procedures performed were in accordance with the ethical standards of the institutional research committee and the Helsinki Declaration.
Setting and data source
This study was conducted in the department of Radiology and Anatomy and gained the approval of the ethical committee (MREC) (No. 21–04-05) with a waiver for informed consent.
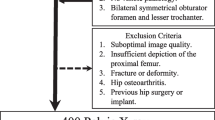
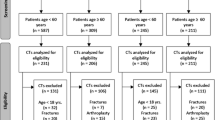
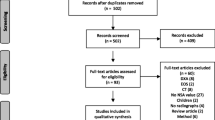
Between January 1, 2021, and December 31, 2023, 600 patients underwent a CT scan of the abdomen and pelvis for the indication of trauma without evidence of traumatic injury. Patients were excluded if their age was below 18, a fracture or deformity in the pelvis or femur was present, there were hip or femur implants, or there was visible hip pathology. This left a total of 300 patients (150 males and 150 females), with an average age of 40.9 ± 12.556 years (range 18–60 years). The following information was collected from the electronic medical records: age and gender. Patients were divided for further analysis into four groups: males 18–39 years old, females 18–39 years old, males 40–60 years old, and females 40–60 years old.
CT protocol
Computed tomography (CT) scans were acquired using a 16-row multiple detector CT (MDCT) scanner (Activation, Toshiba Medical, Tokyo, Japan), with patients in the supine position without contrast medium injection. The following setting parameters were used: Tube voltage, 120 kVp; Tube current modulation, 170–220 mAs; Gantry rotation time, 0.5 s; Helical pitch, 15; Pitch factor, 0.9375; Collimation width, 0.5; and slice thickness, 1 mm.
Image analysis
All images were transferred from the CT machine to the Philips Picture Archiving and Communication System (PACS) workstation. Three-dimensional volume rendering technique (3D VRT) as well as multiplanar coronal and sagittal reformatted images in soft and bone algorithms were obtained from thin slice images according to the parameters seen in Table 1.
The measurements were performed on a computer with a screen size of 19 inches. The measurement protocol involved loading CT scan images onto the software. Images were magnified according to the optimal view. From the software menu, 2D tools were activated.
Plans and reconstructions for measurements of the neck shaft angle
Firstly, simulation of an AP radiograph of the pelvis (Fig. 1) without hip rotation was done by reformatting the CT image into three-dimensional pelvic models (APP) (Fig. 2). Then, coronal reconstruction using the extended multi-planar reconstruction (EMPR) (Fig. 3) was created to eliminate the rotation of the hip of each femur head (FNP) (Fig. 4).

Simulated anteroposterior pelvic radiograph in the anterior pelvic plane

Reformatting the CT image into three-dimensional pelvic models (APP)

Extended multiplanar reconstruction of the femoral neck plane

Coronal reconstruction of the femur neck (FNP)
Reconstruction of the anteroposterior of the pelvis in the anterior pelvic plane (APP)
Three sets of reference planes were considered: The coronal plane defined as the plane that passes through the anterior edge of the pubic symphysis in sagittal view and the anterior superior iliac spines (ASIS) in axial view plane, axial plane which is perpendicular to the coronal one and coincides with the geometric center of the symphysis pubis, and parallel planes established through the femoral head. Reconstruction of the APP generated after rotation of the coronal and axial planes until both ASIS could be seen in the coronal reconstruction on the same axial plane.
Coronal reconstructions of the proximal femur in the plane of the femoral neck (FNP)
Reconstruction in the coronal plane of each hip was performed. The NSA is defined as the angle between the axis of the femoral neck and the femoral shaft. The coronal plane was defined as the plane between the femoral neck axis (FNA) in the axial reconstruction and the long axis of the femur (FLA) in the sagittal reconstruction.
Measurement of neck shaft angle
We have defined the NSA as described by Müller [8] (Fig. 5);
-
1.
Determining the center of the femur head and applying the circular template: The reference points for the circular arc are the lateral portion (outermost point) of the epiphysis and the medial corner of the femoral neck.
-
2.
A point is marked laterally at the strongest sidecut of the femoral neck.
-
3.
Another arc through this point is constructed with the femoral head as the center.
-
4.
The intersection points of the circle with the femoral neck are connected.
-
5.
The perpendicular to this straight line through the center of the femoral head represents the femoral neck axis (FNA).
-
6.
Two circles were drawn in the femur shaft at two positions. The center of circle one was positioned at the lower boundary of the lesser trochanter; the second circle was 2 cm below the first. The circles lie within the outer margins of the femur.
-
7.
A line crossing the centers of two circles was drawn. This line represented the femoral long axis (FLA) (femur shaft axis).
-
8.
The NSA was the angle between the FLA and the FNA.
The femur was classified with NSA less than 120° into the coxa vara (Fig. 6) and with NSA greater than 135° into the coxa valga (Fig. 7). The others were classified as normal [9].

Simulated AP radiograph of right proximal femur showing the reference points for measuring the neck shaft angle (NSA). M—Center of the femoral head, A—Point where the circle intersects the lateral cortex of the femoral neck, B—Point where the circle intersects the medial cortex of the femoral neck. FNA—femoral neck axis (line perpendicular to AB through M), NSA—femoral neck shaft angle, FLA—The long axis of the femur

Representative case of coronal reconstruction of the femur neck (FNP) shows a NSA of 118.7° (coxa vara) at the right femur (green arrow)

Representative case of construction of neck shaft angle (NSA). In a male 19 years old, simulated AP radiograph of the pelvis shows a NSA of 136.1° at the left femur (coxa valga) and 135.10° at the right femur (yellow arrows)
Data collection
The measurements were independently done by two researchers (MI, a consultant radiologist with 15 years of radiology experience, and MT, a senior anatomist with 5 years of anatomy experience) at different times, blinded to each other’s findings. The measurements that corresponded to one another were averaged, and the averaged measurements were then used in subsequent analysis.
Before the commencement of the measurement, the two researchers discussed and had forty CT images to test their measurements. The same goniometer was used for all the measurements. The mean values of the left and right femoral NSAs were recorded. Intra- and inter-rater reliabilities were calculated (Figs. 8, 9).

Representative case of construction of neck shaft angle (NSA). In a male 45 years old, simulated AP radiograph of the pelvis shows a NSA of 126.5° at the right femur and 127.6 0° at the left femur (yellow arrows)

Representative case of construction of neck shaft angle (NSA). In a female 20 years old showing left renal stone (white arrow), simulated AP radiograph of the pelvis shows a NSA of 121.1° at the right femur (brown arrow) and 125.3 0° at the left femur (green arrow)
Statistical analysis
For descriptive analysis, absolute mean values, ranges, and standard deviations (SD) were presented. Variables were tested for normality using the Kolmogorov–Smirnoff test. Spearman's correlation coefficient for normally distributed variables and the two-tailed Wilcoxon matched-pair test for non-normally distributed variables. Differences between variables were evaluated using the nonparametric Mann–Whitney U test or the Kruskal–Wallis test. Concordance between the reviewers regarding the measurements was assessed using the intra-class correlation coefficient (ICC). A p value of less than 0.01 was considered statistically significant. The two-tailed nonparametric Wilcoxon test for matched pairs was used to discover differences between NSAAPP and NSAFNP, with a significance level of p < 0.05. Our data were analyzed using SPSS version 23.0 (IBM Corp., Armonk, NY).
Results
Populations and descriptive data
The study comprised 150 females (median age, 40 years) and 150 males (50%) (median age, 39 years). The age distribution in years of male and female patients by age groups is given in Table 2.
The ages of the 300 subjects included in this study ranged from 18 to 60 years old. Males had a mean age of 40.6 ± 12.6 years and females of 41.17 ± 12 years. It was found that there was no statistically significant association between gender and age distribution (p = 0.43).
Intra-class correlation coefficients (ICC) for inter- and intra-reliability measurements are presented in Table 3 and 4. The intra-rater reliability rates for the two reviewers were 0.93 (95% CI (confidence interval) 0.85–0.97) and 0.87 (95% CI 0.83–0.95).
Neck shaft angle
The NSA values of the study population measured in two views are given in Table 5. The average of NSA in the simulated anterior pelvic plane (NSAAPP) was 129.46 ± 5.06 (range 115.7–146.7). There was no significant difference between observers’ measurements as determined by ANOVA (F(1, 8) = 4.8, P = 0.071).
The average of NSA in rotation-corrected coronal reconstruction femoral neck plane (NSAFNP) was 127.73 ± 4.93 (range 115.3–144.6). There was no significant difference between observers’ measurements as determined by ANOVA (F(1, 9) = 4.9, P = 0.061).
NSA in the simulated anterior pelvic plane (NSAAPP) had a higher mean NSA than the NSA in the rotation-corrected coronal reconstruction femoral neck plane (NSAFNP). The mean difference between NSAAPP and NSAFNP was 1.73°.
Descriptive results of NSA measurements in two views of 600 hips by age are given in Table 6.
The two-tailed nonparametric Wilcoxon test for matched pairs showed significant differences between both measurements (p < 0.000).
In the rotation-corrected coronal reconstruction (NSAFNP), eight (2.7%) femora were categorized as coxa vara (NSA 120°), 282 (94%) as physiologic (NSA 120°–135°), and ten (3.3%) as coxa valga (NSA 135°). The categorization of the NSA measured on the simulated anterior pelvic plane (NSAAPP) revealed the following distribution: coxa vara—3 (1%), physiologic—270 (90%), and coxa valga—27 (9%) hips.
Relation between NSA and age
NSAAPP did not appear to increase with age in either gender (p = 0.614). A relative decrease in NSAFNP with age was noted, which was also statistically not significant (p = 0.810).
The relationship between NSA and sex
Sex-dependent NSA measurements are shown in Table 7. It is evident that sex-dependent NSA measurements show no significant difference (p > 0.05).
Relation between NSA and side
The NSAAPP ranged from 115.70° to 141.40° on the right and 119.10° to 146.70° on the left. The NSAFNP ranged from 116.0° to 135.70° on the right and 115.30° to 144.60° on the left. The unpaired t test in Table 8 revealed a significant difference (p < 0.01).
The group-specific femur NSA of 600 femur bones was determined by two different methods and correlated using Spearman’s rank correlation coefficients given in Tables 9 and 10.
Discussion
The rates of hip arthroplasty have significantly increased, and the demand for primary total hip arthroplasty is predicted to increase by 174% by the year 2030 [10]. The NSA in the femoral head prosthesis's design is a key factor in total hip arthroplasty success. The standard femoral prosthesis in arthroplasty has an NSA of 131°. An improper angle can cause a number of complications, such as wear, poor biomechanics, and groin pain [11]. Hence, a precise measurement of femoral NSA that takes into account regional differences is essential for total hip replacement. The femoral NSA has been examined by several authors, and most authors agree that there is considerable individual variation and a wide standard deviation (Table 11). This difference may possibly be a result of factors affecting bone morphology such as genetic constitution, diet, nutrition status, environment, and physical activity [12]. Computed tomography measurements of the femoral NSA can be a useful tool for creating better-fitting and well-adjusted femoral implants and prostheses to improve treatment results in this situation of a rise in hip procedures [1].
In our CT-based study, the mean value of femoral NSA in adults of the Egyptian population is 129.46° ± 5.06°, with a mean value of 129.65° ± 4.13° for males and 129.28° ± 3.71° for females. These values are in accordance with the previous Egyptian plain radiography-based report in adults, with a mean value of 132.29° ± 4.38° for males and 130.13° ± 4.83° for females [13]. On the other hand, an Indian CT-based study has also reported the values of femoral NSA, which are very close to our findings (mean values of 129.4 4.31 for men and 130.9 ± 5.05 for women) [14]. Contrary to our results, European populations such as the German and Italian populations showed NSAs of 125° 6.0° and 125.3° ± 4.9°, respectively [15, 16]. Studies done in Chinese and American populations showed similar results, with a mean NSA of 133° [17, 18]. A Korean population study found the mean NSA of 130.27° [19].
Gilligan et al. [12], in their study involving multiple areas in the world, analyzed NSA values in relation to the climatic indices and found that most of the higher NSA group means were found within the tropics (e.g., Chad 132.3°, Ethiopia 132.2°, Gabon 130.0°, Guinea 133.5°, Mali 130.8°, Senegal 132.5°, and Sudan 130.5°). Conversely, most of the lower mean NSA values in Africa occurred in cooler parts of the continent (e.g., Algeria 123.4°, Morocco 120.0°, and Mozambique 120.8°). These data consolidated the belief that femoral NSA varies with geographical location.
This study revealed higher mean NSAs for males than for females, although statistically insignificant. This is what other studies have found. Hoaglund and Low [20] reported that in Caucasian people, the NSA was 136° in men and 134° in women; and in Chinese people from Hong Kong, 135° in men and 134° in women; thus, in both groups, a smaller angle was found in women. The larger angles in men have been attributed to a number of reasons, including the narrow pelvis, smaller bicondylar angle, and longer femur. Akbar and Kalim [21] in Pakistan, however, reported values of female NSA that were larger than those of males in both limbs. Radha et al. [22] also noted a higher NSA in females than in males in Indian subjects. Another study also states that there is no consistent pattern of sexual differences across the human population [23].
The side-by-side difference was noted in this study. We revealed a modest but statistically significant side difference for the NSA, with the left femur having a slightly higher NSA (by 4°) than the right femur. This was also reported by Akbar and Kalim [21]. Nwoha [24] and Gilligan et al. [12], however, noted a larger right NSA in their study, while other researchers [22, 25] did not show lateral differences of statistical significance. However, previous researchers postulated that the side difference could be due to leg dominance [12, 24].
Various results for the association with age have been described. Varus hips are more common in both sexes as they get older, whereas valgus hips are less common, which could be due to physiologic changes and lower bone mineral density [26, 27]. The correlation analysis in the present study showed no statistically significant difference regarding femoral NSA and age in both sexes. These results were consistent with [17] and [18]. They discovered that there were no significant changes in NSA between different age groups.
As has been hypothesized, measurements of non-corrected NSA (APP) are susceptible to rotation effects due to hip rotation and flexion. Therefore, the rotation-corrected FNP eliminates the rotational effects and counteracts this problem [28]. The current study documented a significant difference (p = 0.000) of 2° between rotation-corrected (FNP) and non-corrected NSA (APP), slightly higher than the study by Boese et al., who documented a difference of only 1° [29]. Furthermore, the categorization of coxa valga revealed an overestimation in the simulated APP roentgenograms.
The current study showed good intra- and inter-reviewer reliability. While previous studies presented comparable intra-rater reliabilities [30, 31], the inter-rater ICC values ranged from 0.58 to 0.89 in plain radiographs. Nevertheless, other studies have shown higher ICC on CT, such as the study done by Boese et al., reported an intra-rater reliability of 0.995 and an inter-rater reliability of 0.914 [29]. This suggests that the ICC for the femoral NSA has excellent reliability when using a CT scan compared to plain radiography.
Limitations
There are some limitations to this study. Our study population may not be representative of the entire Egyptian population. In particular, our participants were mostly adult residents living in a rural area. In addition, the relatively low number of subjects may have limited the statistical power. The study was also performed at a single institution. Furthermore, no pediatric cases were analyzed, limiting the provided reference values to adult patients. We were unable to evaluate factors such as bone mineral density and weight for the sample. Finally, the cross-sectional study design limits conclusions on cause-and-effect relationships. Thus, further longitudinal studies are necessary. Despite these limitations, we expect our data to provide useful reference ranges for epidemiologic studies in Egyptian adult populations.
The information from this study will be helpful for the Egyptian population with total hip replacement in designing the femoral hip stem. Currently, the majority of femoral hip stems that are produced for the orthopedic market have a fixed NSA. In order to accommodate patients with a variety of NSAs, multiple NSAs have been developed for each hip stem design, which increases inventory significantly for manufacturers.
Conclusions
The current study attempts to develop population-specific data for femoral NSA reference values in Egyptian communities. No considerable difference was measured in NSA among males and females. It was observed that there was a side difference, with the NSA value being higher on the left than the right. We noted also that proper measurement of NSA is made possible by using NSA values obtained from rotation-corrected coronal reconstruction in the FNP. We anticipate that the findings will contribute to a better understanding of proximal femur morphology and may aid the majority of our population in selecting an implant that is compatible with hip anatomy.
Availability of data and materials
MI and MB had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Data are available on reasonable request from the corresponding author.
Abbreviations
- NSA:
-
Neck shaft angle
- CT:
-
Computed tomography
- APP:
-
Simulated anterior pelvic plane
- FNP:
-
Femoral neck plane
- AP:
-
Anteroposterior
- PACS:
-
Picture archiving and communication system
- MDCT:
-
Multiple detector CT
- DICOM:
-
Digital Imaging and Communications in Medicine
- EMPR:
-
Extended multi planar reconstruction
- ASIS:
-
Anterior superior iliac spines
- FNA:
-
Femoral neck axis
- FLA:
-
Long axis of the femur
- SD:
-
Standard deviations
- NSAAPP:
-
NSA in simulated anterior pelvic plane
- NSAFNP:
-
NSA in rotation corrected coronal reconstruction femoral neck plane
- ICC:
-
Intra-class correlation coefficients
- CI:
-
Confidence interval
References
Boese CK, Frink M, Jostmeier J et al (2016) The modified femoral neck-shaft angle: age- and sex-dependent reference values and reliability analysis. Biomed Res Int 66:8645027
Boese CK, Dargel J, Oppermann J, Eysel P, Scheyerer MJ, Bredow J, Lechler P (2016) The femoral neck-shaft angle on plain radiographs: a systematic review. Skeletal Radiol 45(1):19–28
Skaria S, Kulkarni M, Gandotra A (2022) Influence of neck shaft angle of humerus in prosthesis design. J Clin Orthop Trauma 21(10):102045
Schlégl ÁT, Nyakas V, Kovács D, Maróti P, Józsa G, Than P (2022) Neck-shaft angle measurement in children: accuracy of the conventional radiography-based (2D) methods compared to 3D reconstructions. Sci Rep 3(10):16494
Eschweiler J, Hawlitzky J, Quack V, Tingart M, Rath B (2017) Biomechanical model based evaluation of Total Hip Arthroplasty therapy outcome. J Orthop 21(9):582–588
Bhaskar D, Rajpura A, Board T (2017) Current concepts in acetabular positioning in total hip arthroplasty. Indian J Orthop 51(4):386–396
Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP (2008) STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol 61(4):344–9
Di Stasio GD, Mansi L, Waldt S, Woertler K (2014) Measurements and classifications in musculoskeletal radiology. Eur J Nucl Med Mol Imaging 41:1991
Tönnis D (ed) (1984) Die angeborene Hüftdysplasie und Hüftluxation im Kindes- und Erwachsenenalter: Grundlagen, Diagnostik, konservative und operative Behandlung. Springer, Berlin, pp 178–179
Patel A, Pavlou G, Mújica-Mota RE, Toms AD (2015) The epidemiology of revision total knee and hip arthroplasty in England and Wales: a comparative analysis with projections for the United States. A study using the National Joint Registry dataset. Bone Joint J 97-B(8):1076–81
Fink B, Morgan M, Schuster P (2022) Reconstruction of the anatomy of the hip in total hip arthroplasty with two different kinds of stems. BMC Musculoskelet Disord 23:212
Gilligan I, Chandraphak S, Mahakkanukrauh P (2013) Femoral neck-shaft angle in humans: variation relating to climate, clothing, lifestyle, sex, age and side. J Anat 223(2):133–151
Zaghloul A, Mohamed EM, Maaty MT, El-Saied G-A, Hammad A (2020) Computing measurements of femoral neck shaft angle in children and adolescents from nile delta. Orthoped Rheumatol Open Access J 17(1):19–25
Pathak SK, Maheshwari P, Ughareja P, Gadi D, Prashanth RM, Gour SK (2016) Evaluation of femoral neck shaft angle on plain radiographs and its clinical implications. Int J Res Orthop 2:383–386
Merle C, Waldstein W, Gregory JS, Goodyear SR, Aspden RM, Aldinger PR et al (2014) How many different types of femora are there in primary hip osteoarthritis? An active shape modeling study. J Orthop Res 32:413–422
Ripamonti C, Lisi L, Avella M (2014) Femoral neck shaft angle width is associated with hip-fracture risk in males but not independently of femoral neck bone density. Br J Radiol 87:20130358
Jiang N, Peng L, Al-Qwbani M, Xie GP, Yang QM, Chai Y (2015) Femoral version, neck-shaft angle, and acetabular anteversion in Chinese Han population: a retrospective analysis of 466 healthy adults. Medicine 94(21):e891
Unnanuntana A, Toogood P, Hart D, Cooperman D, Grant RE (2010) Evaluation of proximal femur geometry using digital photographs. J Orthop Res 28(11):1399–1404
Cho HJ, Kwak DS, Kim IB (2015) Morphometric evaluation of Korean Femur by geometric computation: comparisons of the sex and the population. Biomed Research Int 2015:730538
Hoaglund F, Low WD (1981) Anatomy of the femoral neck and head, with comparative data from Caucasians and Hong Kong Chinese. Clin Orthopaed Rel Res 66:10–16
Akbar W, Kalim U (2015) A radiographic study of neck shaft angle in a population of Mardan region, Khyber Pukhtonkhwa, Pakistan. Biomedica 31:108–114
Radha P, Ravi SG, Naveen NS, Roopa CR (2015) Evaluation of neck shaft angle of femur on dry bones. J Evol Med Dent Sci 4:5518–5522
Janjua SN, Habib K, Kirn S, Fatima S, Nasir Erum (2020) A study of femoral neck shaft angle in adults of islamabad and its clinical implications. Pak J Med Res 1(59):32–36
Nwoha PU (1991) The collodiaphyseal angle of the femur in adult Nigerians. Afr J Med Med Sci 20:143–147
Kaur P, Mathew S, George U (2013) A study of neck shaft angle in the North-West Indian population on radiograph. Int J Basic Appl Med Sci 3:9–15
Nissen N, Hauge E, Abrahamsen B, Jensen J, Mosekilde L, Brixen K (2005) Geometry of the proximal femur in relation to age and sex: a cross-sectional study in healthy adult Danes. Acta Radiol 46:514–518
Elbuken F, Baykara M, Ozturk C (2012) Standardisation of the neck–shaft angle and measurement of age-, gender- and BMI-related changes in the femoral neck using DXA. Singap Med J 53(9):587–590
Fischer CS, Kühn JP, Völzke H, Ittermann T, Gümbel D, Kasch R, Haralambiev L, Laqua R, Hinz P, Lange J (2020) The neck-shaft angle: an update on reference values and associated factors. Acta Orthop 91(1):53–57
Boese CK, Jostmeier J, Oppermann J, Dargel J, Chang DH, Eysel P, Lechler P (2016) The neck shaft angle: CT reference values of 800 adult hips. Skeletal Radiol 45(4):455–463
Mast NH, Impellizzeri F, Keller S, Leunig M (2011) Reliability and agreement of measures used in radiographic evaluation of the adult hip. Clin Orthop Relat Res 469:188–199
Nelitz M, Guenther KP, Gunkel S, Puhl W (1999) Reliability of radiological measurements in the assessment of hip dysplasia in adults. Br J Radiol 72:331–334
Adekoya-Cole TO, Akinmokun OI, Soyebi KO, Oguche OE (2016) Femoral neck shaft angles: a radiological anthropometry study, Niger. Niger Postgrad Med J 23(1):17
Shrestha R, Gupta H, Hamal R, Pandit R (2018) Radiographic Anatomy of the neck-shaft angle of femur in Nepalese people: correlation with its clinical implication. Kathmandu Univ Med J 62:124–128
Jiang N, Peng L, Al-Qwbani M, Xie GP, Yang QM, Chai Y, Zhang Q, Yu B (2015) Femoral version, neck-shaft angle, and acetabular anteversion in Chinese Han population: a retrospective analysis of 466 healthy adults. Medicine 94(21):5
Altubasi I, Hamzeh H, Madi M (2020) Measurement of neck-shaft angle using CT Scout View in Healthy Jordanian Adults—a reliability and agreement study. J Adv Med Med Res 32(16):9–17
Mitra A, Khadijeh B, Vida AP, Ali RN, Farzaneh M, Maryam VF, Vahid Y (2014) Sexing based on measurements of the femoral head parameters on pelvic radiographs. J Forensic Leg Med 23:70–75
Acknowledgements
Not applicable.
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the research committee of faculty of medicine, Sohag University hospital. Sohag University November 2021 (Soh-Med-21-04-05).
Consent for publication
Not required.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ahmad, M.I.M., Bushra, M.T., Galal, A.T. et al. Computed tomography reference values estimation for femoral neck shaft angle in Egyptian healthy adults of both sexes. Egypt J Radiol Nucl Med 54, 96 (2023). https://doi.org/10.1186/s43055-023-01040-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-023-01040-x