
Abstract
Background
Arachnoid web of the spine is a not so common lesion of the spinal cord. It is a band-like arachnoid tissue in the intradural extramedullary compartment that extends to the surface of the spinal cord, with a tendency to occur in the upper dorsal spine causing focal dorsal indentation of the cord that has been coined the ‘scalpel sign’. Patients usually present with progressive weakening and numbing of bilateral lower limb.
Case presentation
A 58-year-old man presented with difficulty in walking and weakness of right leg for 1 year, aggravated over the previous 2 months. There was no history of trauma or fever. Magnetic resonance imaging (MRI) of the dorsal spine was done which revealed a small syrinx within the cord at D4 vertebral level on right side. There was sharp dorsal indentation of the spinal cord and widening of the arachnoid space below this level. This appearance was similar to a surgical scalpel. The anterior subarachnoid space was preserved. On post-contrast images, no parenchymal or meningeal enhancement was detected. The patient was taken up for surgery as the symptoms further progressed. Laminectomy was done from D3 to D7 under general anesthesia, with release of arachnoid web and adhesions. Histology of the resected specimen revealed epithelial cells and fibrous tissue. No inflammatory or neoplastic cells were observed.
Conclusions
Thoracic arachnoid web is a rare entity, which if not treated can have devastating effects on a patient’s neurological function. Careful evaluation of radiological findings is important to avoid delay in diagnosis. Surgery is the only curative treatment and is known to have a favorable outcome.
Similar content being viewed by others
Background
Arachnoid web of the spine is an intradural extramedullary band of arachnoid tissue that extends to the surface of the spinal cord, with a tendency to occur in the upper dorsal spine focally indenting the dorsal surface of the cord that has been coined the ‘scalpel sign’[1]. It is an uncommon entity with only 63 reports in the literature till July 2021 [2].
The main presenting features are progressive bilateral lower limb weakness and numbness with long standing walking difficulties without any confirmatory diagnosis. Physicians need to have a high level of suspicion for this entity after exclusion of more common etiologies of these symptoms such as degenerative diseases or tumors.
The exact cause of arachnoid webs is still not certain. There are several theories put forth, like forceful flow of CSF that results in arachnoid herniating into a congenital dural defect and posttraumatic, postinfectious, and postoperative etiologies [3, 4]. These webs are also thought to be a variant of arachnoid cysts or remnants of arachnoid cysts that have collapsed [5] Although there are many theories, yet it is currently not known how non-traumatic arachnoid webs are formed, and the possibility of them being idiopathic or congenital is being considered [3].
This thickened membrane is thought to block the movement of CSF in the longitudinal direction, which may result in progressive alteration of the cerebrospinal fluid flow dynamics and ultimately lead to formation of syrinx [1, 5]. The location of the syrinx varies relative to the arachnoid web, and may be caudal or, more commonly, cranial to it [3].
MR imaging is the main imaging technique, though CT myelography has also been used less frequently. The precise localization of the arachnoid web is difficult before surgery, as the thin structure of the arachnoid web is usually difficult to visualize. Therefore, the main feature that implies the diagnosis of an arachnoid web is the anterior displacement and deformity of the spinal cord [5].
Arachnoid web is sometimes considered as another variant of arachnoid cysts [3, 6]. However, spinal arachnoid cysts show distinct imaging features like the frequently well-defined cyst borders, a slower filling of the cyst in CT myelography or MRI cerebrospinal flow imaging and a more diffuse distortion of the spinal cord without displaying the scalpel sign [3, 6].Thin wall of the cyst may be visible at its margins on high resolution thin section MRI. (Fig. 4).
Another condition which can mimic imaging features of arachnoid web is the herniation of spinal cord which forms an important differential. Although both conditions present with similar clinical signs and symptoms, yet subtle MRI findings can help to differentiate arachnoid web from spinal cord herniation. While the scalpel sign is thought to be pathognomonic for arachnoid web, ventral displacement of the spinal cord with a discontinuous ventral subarachnoid space and a C-shaped dorsal surface of the cord is characteristic for spinal cord herniation [7]. Surgery for spinal cord herniation requires the repair of the ventral dural defect through which the cord herniates [7].
Arachnoiditis ossificans is another differential in the diagnosis of focal arachnopathy. It is an uncommon calcification of the arachnoid layer with characteristic histo-pathological features. It causes spinal cord compression, similar to arachnoid web and is mostly located in the dorsal spine with corresponding symptomatology [8]. Associated syrinx is described in a some of these cases, but is not the norm as in arachnoid web. Imaging modalities such as magnetic resonance imaging and computed tomography show an intradural extramedullary calcified lesion compressing the spinal cord [8].
The most common surgical procedure is laminectomy with intradural excision of the arachnoid web including some variations of this with hemilaminectomy and minimally invasive techniques [9]. Less commonly, shunt and stent placement have been used for cerebrospinal fluid diversion flow diversion [2].
Case presentation
A 58-year-old man presented with difficulty in walking and weakness of right leg for 1 year, aggravated over the previous 2 months. There was no numbness or sensory disturbances of the limbs or torso. The patient was non-diabetic and non-hypertensive. There was no history of trauma or fever. On neurological examination, power in the right leg was 3/5 and that in the left leg was 4/5. Deep tendon refluxes were exaggerated. Upper limbs showed normal power and reflexes. All laboratory investigations were normal.
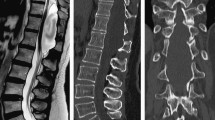
MRI of the dorsal spine was done (Fig. 1) which revealed a small syrinx within the cord at D4 vertebral level on right side. There was sharp dorsal indentation of the cord & widening of the subarachnoid space below this level. This appearance was similar to a surgical scalpel. The anterior subarachnoid space was preserved. On post-contrast images, no parenchymal or meningeal enhancement was detected. MRI brain was non-contributory (not shown).

MRI of the dorsal spine T2W sagittal (a, b) and axial (c, d) sections show a small syrinx within the cord at D4 vertebral level on right side (black arrow). There was sharp dorsal indentation of the cord (black arrow in a) and widening of the subarachnoid space below this level. This appearance is similar to a surgical scalpel. The anterior subarachnoid space is preserved
The patient was taken up for surgery as the symptoms further progressed. Laminectomy was done from D3 to D7 under general anesthesia, with release of arachnoid web and adhesions (Fig. 2). Histology of the resected specimen revealed epithelial cells and fibrous tissue. No inflammatory or neoplastic cells were observed.

Intraoperative image demonstrating the arachnoid web (yellow arrow)
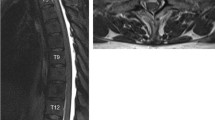
The patient’s symptoms subsequently improved. A repeat MRI was done 5 months later (Fig. 3) that showed resolution of the intramedullary signal abnormality and indentation of the cord seen previously.

Repeat MRI of the dorsal spine T2Wsagittal (a) and axial (b, c) 5 months later depicting resolution of the intramedullary signal abnormality and indentation of the cord seen previously in Fig. 1
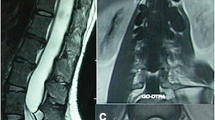
Figure 4 is high-resolution thin section MRI showing the thin wall of an arachnoid cyst which forms an important differential of arachnoid web. The classic ‘scalpel sign’ is not seen in arachnoid cyst.

MRI of the arachnoid cyst in dorsal spine T2W sagittal (a) and axial (b, c) sections demonstrating an increase in the posterior arachnoid space in mid and lower dorsal spine displacing and compressing the spinal cord anteriorly. A thin membrane is observed at the upper end (white arrow in a) and anterior edge (white arrows in c)
Conclusion
Thoracic arachnoid web is a not so common entity, which if not treated in time can have disastrous effects on a patient’s neurological function. Its early recognition along with careful evaluation of radiological findings is important to avoid delay in diagnosis. The presence of syringomyelia without any readily identifiable cause, along with ventral displacement of the cord and/or the appearance of the ‘scalpel sign’, is essential for the diagnosis of arachnoid web. Surgery is the only treatment and is known to have a favorable outcome.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author.
Abbreviations
- CSF:
-
Cerebrospinal fluid
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
References
Reardon MA, Raghavan P, Carpenter-Bailey K et al (2013) Dorsal thoracic arachnoid web and the “scalpel sign”: a distinct clinical-radiologic entity. AJNR Am J Neuroradiol 34(5):1104–1110
Hines TK, Wang C, Duttlinger C, Thompson J, Watford K, Motley B et al (2021) Thoracic dorsal arachnoid web with rapid onset of symptoms: a report of two cases and brief review of the literature. Surg Neurol Int 12:323
Ali HB, Hamilton P, Zygmunt S, Yakoub KM (2018) Spinal arachnoid web—a review article. J Spine Surg 4(2):446–450
Chang HS, Nagai A, Oya S et al (2014) Dorsal spinal arachnoid web diagnosed with the quantitative measurement of cerebrospinal fluid flow on magnetic resonance imaging. J Neurosurg Spine 20:227–233
Brasil PM, Pereira LP, Távora DGF, Camara ACF, Macedo Filho CL, Coimbra PPA (2020) Imaging findings in dorsal thoracic arachnoid web and the differential diagnosis of “Scalpel Sign.” Neurographics 10(2):96–102. https://doi.org/10.3174/ng.1900037
Paramore CG (2000) Dorsal arachnoid web with spinal cord compression: Variant of an arachnoid cyst? J Neurosurg Spine 93(2):287–290
Schultz R, Steven A, Wessell A, Fischbein N, Sansur CA, Gandhi D, Raghavan P (2017) Differentiation of idiopathic spinal cord herniation from dorsal arachnoid webs on MRI and CT myelography. J Neurosurg Spine 26(6):754–759
Ibrahim G, Kamali-Nejad T, Fehlings M (2010) Arachnoiditis ossificans associated with syringomyelia: an unusual cause of myelopathy. Evid-Based Spine-Care J 1(02):46–51
Nisson PL, Hussain I, Härtl R, Kim S, Baaj AA (2019) Arachnoid web of the spine: a systematic literature review. J Neurosurg Spine 31(2):175–184
Acknowledgements
Nil
Funding
No funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
VA contributed to conceptualization, methodology, validation, formal analysis, writing—original draft, review and editing, visualization, supervision and project administration. HV contributed to conceptualization, methodology, validation, formal analysis, writing—original draft, review and editing, visualization, supervision and project administration. RK contributed to conceptualization, methodology, validation and supervision. NAL contributed to formal analysis, supervision and project administration. All the authors have read and approved the submitted version and have agreed both to be personally accountable for their contributions and to ensure that the questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study is in accordance with the ethical standards of Institutional Review Board and the Declaration of Helsinki.
Consent for publication
Yes, written informed consent has been obtained from the study participants.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Arora, V., Verma, H., Kamal, R. et al. Dorsal arachnoid web: the ‘scalpel’ sign—a case report and differential diagnosis. Egypt J Radiol Nucl Med 53, 163 (2022). https://doi.org/10.1186/s43055-022-00847-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00847-4