
Abstract
Background
High-dose radioactive iodine-131 (I-131) is generally used post-total or subtotal thyroidectomy in differentiated thyroid cancer (DTC) patients. I-131 whole-body scan (WBS) is performed to localize I-131 accumulation in the body and for restaging after therapy. Nonetheless, there are numerous causes of false-positive uptake in I-131 WBS in the absence of residual thyroid tissue or thyroid cancer metastasis.
Case presentation
We present a case of 51-year-old lady with false-positive uptake in I-131 WBS mimicking lung metastasis. Patient underwent total thyroidectomy, and histopathological examination showed well-differentiated papillary thyroid microcarcinoma. Diagnostic I-131 WBS followed by two subsequent high-dose radioiodine ablation showed persistent I-131 uptake in the left lower lung field. However, the serum thyroglobulin (Tg) is incessantly undetectable (< 0.04 μg/ml) with negative anti-thyroglobulin antibody (anti-TgAb). Three serial CT scans over the course of treatment coupled with MRI of the thoracolumbar region revealed stable lung lesion in the posterior segment of left lower lobe which signifies pulmonary sequestration. Based on the clinical assessment, imaging findings and blood investigations, patient was no longer subjected to I-131 therapy and is maintained on TSH suppression with L-thyroxine. After due consideration of the pros and cons of surgical intervention, the patient opted against surgical removal of the pulmonary sequestration.
Conclusions
Meticulous assessment of patient with suspected disease recurrence or metastasis in thyroid carcinoma is essential to avoid unnecessary I-131 ablation or surgical intervention. In this case, the positive I-131 imaging is associated with undetectable serum Tg (with negative anti-TgAb). Albeit uncommon, pulmonary sequestration should be taken into consideration as one of the differentials in false-positive findings of an I-131 WBS.
Similar content being viewed by others


Background
Iodine-131 (I-131) has been used effectively over the years in both diagnosis and therapy of differentiated thyroid cancer (DTC). Whole-body scan (WBS) of I-131 from either diagnostic or therapeutic doses can reveal foci of normal residual thyroid tissue, carcinoma or remote metastasis in post-surgical DTC patients [1]. We report a case of DTC with persistent I-131 pulmonary uptake in the serial diagnostic and therapeutic WBS despite undetectable serum thyroglobulin (Tg). Although I-131 WBS is specific, there are myriad of abnormal lesions which can produce false-positive imaging results [1]. As for this case, radiological imaging advocates pulmonary sequestration (PS) as the main differential of persistent I-131 uptake in the left lower lung field. Although the diagnosis is not histopathologically proven, there are few articles which discussed the radiological imaging findings indicating the diagnosis [2, 3]. The precise interpretation of I-131 WBS is important to avoid unnecessary high-dose I-131 ablation and to optimize the management of DTC as well as other non-thyroidal lesions.
Case presentation
A 51-year-old lady presented with progressive anterior neck swelling in March 2011. Total thyroidectomy was performed, and histopathological examination revealed a right thyroid lobe nodule 6 mm in size, that was compatible with well differentiated papillary thyroid microcarcinoma. Post-operative serum Tg was 0.09 μg/ml, and the value of anti-thyroglobulin antibody (anti-TgAb) was 10.9kIU/L. She was risk stratified into the low-risk group (in view of microcarcinoma, low serum Tg and negative anti-TgAb) and based on the 2009 American Thyroid Association (ATA) guidelines, consideration for pretherapy diagnostic WBS is only recommended if a change of management is to be expected [4]. As the patient was in the low-risk group, levothyroxine was commenced for thyroid-stimulating hormone (TSH) suppression with concurrent serial serum Tg and anti-TgAb monitoring.
Three years later, she presented to the hospital with a chief complaint of haemoptysis. CT thorax (2.12.14) showed an ill-defined heterogeneously enhancing mass with spiculated margin at the posterobasal segment of left lower lobe (measuring 4.1 × 2.0 cm) suspicious of malignancy (Fig. 1). Subsequently, another two serial CT scans over a period of 1 year were performed in addition to an MRI of the thoracolumbar region with findings showing stable lung lesion in the posterior segment of left lower lobe that signifies pulmonary sequestration (Fig. 2). Both imaging modalities advocate pulmonary sequestration as the main differential.

CT thorax dated 2.12.14, a axial, b coronal and c sagittal views showing ill-defined heterogeneously enhancing mass at posterobasal segment of left lower lobe

Magnetic resonance imaging of patient (9.4.15); a T1 weighted, b T2 weighted and c T1 weighted with gadolinium showing lobulated lung lesion (arrow) at posterobasal segment of left lower lobe which is isointense to all muscle in all sequences and heterogeneously enhances post contrast. There is also a benign right paravertebral mass seen in the MRI study
Diagnostic I-131 WBS was subsequently ensued on 1.11.15 and demonstrates two foci of intense increased tracer uptake in the thyroid bed with accompanying star artefact as well as I-131 uptake at the left lower lung field (Fig. 3). The patient was then subjected to a high-dose radioiodine ablation (150 mCi) on 10.5.16 with post-therapy WBS which showed tracer accumulation in the thyroid bed and left lower lung field, similar to the initial diagnostic WBS. Another radioiodine ablation of 150 mCi (total cumulative dose of 300 mCi) was given after a period of 6 months. Post-therapy WBS portrays the resolution of the previously seen uptake in the thyroid bed with persistent I-131 avidity at the left lower lung field (Fig. 4).

I-131 diagnostic whole-body scan (DxWBS) on 1.11.15 showed tracer uptake in the thyroid bed and left lower lung field (arrow)

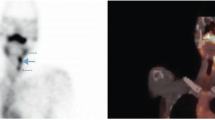
(Left) Post-therapy whole-body scan (150 mCi I-131 given on 2.11.16) and (right) spot view of the thorax showed persistent tracer uptake in the left lower lung field (arrow) which is more prominent posteriorly
Her sequential stimulated and unstimulated serum Tg levels from August 2015 till January 2017 were undetectable (negative anti-TgAb) with only one recorded reading of 5.9 μg/mL (1.11.15) prior to her I-131 diagnostic WBS, which was attributed to the presence of remnant thyroid tissue (Table 1).
Written consent was obtained from the patient to report the case.
This case illustrates persistent I-131 uptake in the left lower lung field. However, the serum Tg was incessantly undetectable (< 0.04 μg/ml) with negative anti-TgAb. Serial CT scans and MRI findings showed stable lung lesion in the posterior segment of left lower lobe that signifies pulmonary sequestration. Based on the clinical assessment, imaging findings and blood investigations, patient was no longer subjected to I-131 therapy and was presently on TSH suppression with Levothyroxine. After careful consideration of the risks and benefits, and lack of specialty for lung biopsy in our centre, patient opted against biopsy and surgical removal of the pulmonary lesion.
Discussion
Conscientious assessment of abnormal scans coupled with clinical assessment and biochemical correlation is essential to avert needless surgical intervention or ensuing ablation with high-dose radioiodine. False-positive I-131 uptake in WBS comprising the chest region has been reported in the literature. The aetiology encompasses acute respiratory infection, pulmonary tuberculosis, pulmonary aspergilloma, rheumatoid lung disease and bronchiectasis [1].
Pulmonary sequestration is an uncommon congenital anomaly of the lower respiratory tract which comprises a mass of lung tissue that is non-functioning [3]. The incidence of pulmonary sequestration is 1 in 10,000 to 35,000 live births and represents 1 to 6% of the congenital abnormalities involving the lower airway [2, 3]. In general, pulmonary sequestration can be classified into two forms. Intrapulmonary sequestration which is enclosed inside the visceral pleura of the adjoining lung accounts for 75% of the cases while extrapulmonary sequestration, which is situated externally with its own visceral pleura contributes the remaining 25% [2]. Interestingly, almost two-thirds of intrapulmonary sequestration are found in the posterobasal segment of the left lower lobe [3] as demonstrated in this case.
The pathophysiology of pulmonary sequestration is not completely understood. The universally approved understanding is that it is derived during development from an accessory lung bud inferior to the normal lung buds [2, 3]. At the time of embryogenesis, the accessory lung bud acquires a separate vascular supply, independent from the normal developing tracheobronchial tree [3]. The airways of the lesion often reveal mucus accumulation, regions of inflammation, microcystic changes and distortion of lung parenchyma, while pathological examination demonstrates enlarged and thickened airspaces in the abnormal parenchyma [3].
The majority of patients are asymptomatic, and the disease is often diagnosed during routine medical examination or in recurrent bacterial lung infection affecting the lower lobe [5]. Symptoms are often non-specific consisting of chest pain, breathlessness, wheezing, fever, cough and recurrent infections [5], with infection being noted as the most common complication [3]. Other complications include creation of left to right shunt and haemorrhage, which can be fatal [3].
Imaging of pulmonary sequestration includes (i) arteriogram, which is vital in documenting systemic blood supply, (ii) chest X-ray, which usually shows homogenous dense mass in the thoracic cavity, (iii) ultrasound, which shows echogenic mass that is well defined or irregular, (iv) computed tomography (with accuracy of diagnosis of approximately 90%), which shows solid homogenous or heterogenous mass and reveals anatomic position with vascular anatomy, and (v) magnetic resonance imaging, which demonstrates lung mass, systemic blood supply along with its venous drainage [2, 5]. Management of lung sequestration in the asymptomatic patient is subject to controversy. Most authors advocate surgical resection of the lesions owing to the propensity for recurrent infection and possibility of haemorrhage [5].
Up to the present, only two cases of pulmonary sequestration causing false-positive findings in I-131 whole-body scan have been reported. The first case was reported by Jimenez-Bonilla et al. [6] in 2013 which showed I-131 uptake in a lesion at the right posterior costodiaphragmatic recess followed by Spinapolice et al. [7] in the ensuing year which reported a case of I-131 uptake of a nodular lesion in the upper mediastinum in between the aortic arc and pulmonary artery. The mechanism of I-131 uptake in pulmonary sequestration is not known. Examination of the surgical specimen from the case report by Spinapolice et al. [7] demonstrates a huge haemorrhagic infiltrate which might be responsible for I-131 fixation in the pulmonary sequestration.
In cases of discordant findings of low or undetectable serum Tg (with negative anti-TgAb) but positive I-131 WBS, single-photon emission computed tomography/computed tomography (SPECT/CT) is strongly advocated whenever available. Study by Zilioli et al. [8] has shown that SPECT/CT has an additional value over planar whole-body scan in augmenting accuracy of diagnosis and lowering pitfalls and alters patient management by providing anatomical correlation and localization of radioiodine uptake.
Conclusions
Meticulous assessment of patient with suspected disease recurrence or metastasis in differentiated thyroid carcinoma is essential to avoid unnecessary I-131 ablation or surgical intervention. In this case, the positive I-131 imaging is associated with undetectable serum Tg (with negative anti-TgAb). Albeit uncommon, pulmonary sequestration should be taken into consideration as one of the differentials in false-positive findings of I-131 WBS.
Availability of data and material
Not applicable.
Abbreviations
- I-131:
-
Iodine-131
- WBS:
-
Whole-body scan
- DTC:
-
Differentiated thyroid carcinoma
- Tg:
-
Thyroglobulin
- TSH:
-
Thyroid-stimulating hormone
- PS:
-
Pulmonary sequestration
References
Oh J-R, Ahn B-C (2012) False-positive uptake on radioiodine whole-body scintigraphy: physiologic and pathologic variants unrelated to thyroid cancer. Am J Nucl Med Mol Imaging 2(3):362–385
Walker CM, Wu CC, Gilman MD, Godwin JD, Shepard JAO, Abbott GF (2014) The imaging spectrum of bronchopulmonary sequestration. Curr Probl Diagn Radiol 43(3):100–114. https://doi.org/10.1067/j.cpradiol.2014.01.005
Oermann CM (2019) Bronchopulmonary sequestration, UpToDate. Available from https://www.uptodate.com/contents/bronchopulmonary-sequestration. Accessed 15 July 2021.
Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ et al (2009) Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 19(11):1167–1214. https://doi.org/10.1089/thy.2009.0110
Qian X, Sun Y, Liu D, Wu X, Wang Z, Tang Y (2015) Pulmonary sequestration: a case report and literature review. Int J Clin Exp Med 8(11):21822–21825
Jiménez-Bonilla JF, Bravo Z, Quirce R, Martínez-Rodríguez I, Banzo I, Gómez J et al (2013) An exceptional false-positive finding in the postsurgical I 131 whole body scan of a differentiated thyroid carcinoma caused by an extralobar pulmonary sequestration. J Clin Endocrinol Metab 98(5):1797–1798. https://doi.org/10.1210/jc.2013-1057
Spinapolice EG, Chytiris S, Fuccio C, Leporati P, Volpato G, Villani L et al (2014) Pulmonary sequestration: a (131)I whole body scintigraphy false-positive result. Ann Nucl Med 28(7):683–687. https://doi.org/10.1007/s12149-014-0838-5
Zilioli V, Peli A, Panarotto MB et al (2017) Differentiated thyroid carcinoma: incremental diagnostic value of 131I SPECT/CT over planar whole body scan after radioiodine therapy. Endocrine 56(3):551–559. https://doi.org/10.1007/s12020-016-1086-3
Acknowledgements
We thank the Management of the Hospital Universiti Sains Malaysia (USM), Kubang Kerian Kelantan, Malaysia, for providing facilities for the study. Many thanks to co-authors for the contribution making this manuscript successfully produced.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
All the authors contribute in this case report. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethic approval and consent to participate
Not applicable.
Consent for publication
Consent obtained.
Competing interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rohani, M.F.M., Sohaimi, W.F.W., Nawi, N.M. et al. Pulmonary sequestration: a rare cause of false-positive uptake in Iodine-131 whole-body scan. Egypt J Radiol Nucl Med 53, 50 (2022). https://doi.org/10.1186/s43055-022-00723-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-022-00723-1