
Abstract
Background
The aim of the study is to characterize the breast lesions on high-resolution Ultrasound and digital mammography to find the patterns and prevalence of different breast lesions in different age groups of our population.
Results
This prospective study was conducted at a breast care clinic of a tertiary care hospital from Jan 2018 to Dec 2019. Patients with breast-related complaints were enrolled. Patients under the 35 years of age were evaluated on High-Resolution Ultrasound (HR-USG) and those over 35 years of age on digital Mammography. Any lesion on digital mammography was characterized on HR-USG. Fine Needle Aspiration (FNAC) and Trucut biopsy was done where pathological correlation required. Data of all enrolled patients were recorded and analyzed. Patients with known cases of carcinoma breast on follow-up were excluded from the study. Total 6850 patients enrolled in our breast care clinic during study period. 5111 were above the age of 35 years while 1739 were under the age of 35 years. No lesion could be found in 3915 patients and were reported normal. 2935 patients were found to have different breast lesions. The frequency of different lesions was different in both age groups. The overall frequency of lesions was as malignancy 16.2%, benign lesions including Fibroadenoma, simple cysts, Lipoma and Galactocele 16%, inflammatory lesions including abscess 7.86% and Duct Ectasia 2.75%.
Conclusions
In developing countries where mass screening programs are deficient, Breast Care clinics in tertiary care hospitals have a noteworthy role in early detection of breast cancer and other breast lesions.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Increasing awareness for breast cancer being the most common cancer in women worldwide [1] with a high mortality rate is the reason for the increasing number of patients reporting to breast care clinics for any breast-related symptoms [2]. Mastalgia, breast lump, nipple discharge and focal pain are common presenting complaints. Established and genuine workup is required for early diagnosis and treatment [3, 4]. Patients are evaluated by clinical examination that alone has limited value for detection of breast lesions, so evaluation on radiological imaging is mandatory for patients with breast-related symptoms [5]. Triple assessment by a combination of clinical evaluation, imaging and FNAC is established, management of breast lesions [6, 7].
Digital Mammography is the modality of choice for patients above the age of 35 years. It has an accepted role in screening of breast cancer and evaluation of clinically apparent breast lesions [8]. But its diagnostic and screening value is dependent on tissue density of breasts, being low sensitivity for dense breast [3, 9]. Patients below the age of 35 years are evaluated on Sonomammography/HR-USG that also allows the characterization of lesions detected on digital mammography [9,10,11]. USG of breast gains value in patients with dense breast tissue where digital mammography has poor sensitivity [9, 12]. Moreover, its sensitivity for detection of lesions is not impeded by tissue density [5]. Under usual working conditions solid lesion of up to 5 mm and cystic lesion of up to 3 mm size can be detected on HR-USG [11, 13, 14]. But literature shows reporting of solid lesion less than 5 mm [15].
Lesions are assigned grades 0–6 according to latest Breast Imaging Reporting and Data System (BIRADS) lexicon descriptors 2013, a standard system for reporting breast lesion on imaging defined by American college of Radiology (ACR), as inconclusive, benign, probably benign, probably malignant, malignant and biopsy proven, respectively [16]. Further evaluation by FNAC and biopsy may be needed for pathological correlation.
In developing countries like ours, there is no mass screening programs for early detection of breast cancer that has a fundamental role to fight against the high mortality rate of breast cancer due to late presentation. Breast care clinics have been established in few public sector organizations with the provision of imaging modalities to facilitate the early diagnosis of different breast lesions in symptomatic patients. Breast care clinic, where the study was conducted, is the only established clinic in the public sector of our region; it is equipped with latest imaging modalities of digital mammography, HR-USG and facilities for USG-guided FNAC and Trucut biopsy and are providing the services to the women of our population.
Methods
This prospective study was conducted at the breast imaging section of the Radiology department of a tertiary care hospital providing the services for evaluation of patients referred from primary and secondary healthcare centers with different breast-related symptoms. Total 6850 patients presented in two years from Jan 2018 to Dec 2019 with different presenting complaints including Mastalgia, nipple discharge, lump, focal pain, inverted nipple. As no patient’s personal data were involved for publication, so no patient consent was required. All patients were primarily evaluated on clinical history and examination. Mammography was performed on a digital mammography machine without tomosynthesis in patients with age more than 35 years of age. HR-USG with 7–10 MHz transducer was done in younger patients of less than 35 years and also in patients over 35 years with positive findings on digital mammography to characterize the lesion. On HR-USG, lesions were characterized with size, echogenicity in comparison with surrounding tissue, margins, calcifications, fluid movement in lesion and vascularity on Doppler flow. USG-guided FNAC and Trucut biopsies were done in cases where pathological correlation required.
Results
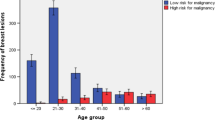
Total 6850 patients enrolled in our breast care clinic were divided into two groups, one below the 35 years of age and second above the age of 35 years. 1739 patients were enrolled in group 1 and 5111 in group 2. No lesion could be found in 3915 patients and were reported normal. Different breast lesions were found in 2935 patients. Pattern of different lesions was different in both age groups (Fig. 1 showing percentages of different breast lesions in patients with age < 30 years and Fig. 2 showing percentages of different breast lesions in patients with age > 30 years). A summary of different lesions in total patients is given in Table 1. Frequency of different lesions in specific age group in comparison with total patients is shown in Tables 2 and 3.

Percentages of different breast lesions in patients with age < 30 years

Percentages of different breast lesions in patients with age > 30 years
Different lesions were having different frequencies in both age groups. 3915 (57.19%) of total patients were found normal and reported as BIRADS 1. Overall, malignancy was found to be the most frequent lesion that constituted 16.2% of total and 15.35% in older age groups. Fibroadenoma was seen in 611 patients. Cysts were seen in 332 patients. 53 patients turned out to have Galactocele. Lipoma was seen in 80 patients. Intraductal papilloma was seen in 16 patients. 536 lesions were diagnosed as inflammatory lesions on aspiration of pus or inflammatory cells on cytology. 356 were labeled as breast abscess. Duct Ectasia was seen in 194 patients. Phyllodes tumor was diagnosed in 12 patients.
Discussions
Malignant lesions on digital Mammography show irregular, speculated and dense opacities with or without microcalcifications those on HR-USG appear ill defined irregular, ragged, microlobulated and hypoechoic masses with posterior shadowing and may show 1–3 mm calcifications [17]. Most of malignant lesions show different patterns of central, tortuous and penetrating vascularity on Doppler Flow. Malignancy is confirmed on histopathology of Trucut biopsies. We opted for Trucut biopsy in all lesions with irregular or micro lobulated margins (Fig. 3).

Lesion that appeared as well defined opacity on digital mammography, revealed microlobulated margins (Black arrows) on HR USG and was let out invasive Ductal carcinoma on Trucut biopsy in a patient of 38 years of age
Phyllodes tumor shows features of benign tumor with well-defined regular margins but larger in size with history of rapid growth and may show cystic areas and moderate vascularity on Doppler scan (not shown).
Benign lesions have more or less same incidence in both age groups with Fibroadenoma being the most common benign lesion in the younger age group and cysts in older age groups. Fibroadenoma is common in younger women and is characterized on HR-USG as well defined with smooth margins usually hypoechoic, parallel to skin surface and wider than taller mass which may show posterior enhancement or macrocalcifications. Higher risk of transformation in breast cancer is seen in complex Fibroadenomas those might appear as lobulated, might show calcifications or cystic changes. These patients are put on close follow-up for any change in size or shape so might be further evaluated by Pathological correlation [18, 19]. Our study elaborated the commensurate frequency of benign lesions in both age groups. Fibroadenoma was the most common benign lesion in our patients of all age groups.
Cysts are common in older age groups. Cysts may appear simple or complex on HR-USG. Simple cysts appear as well defined thin walled anechoic lesion and does not show vascularity while complex cyst might show thick or irregular wall, mural nodularity, internal echoes or intracystic solid component [11]. Complex cysts may show malignancy on histopathology so should be evaluated on aspiration cytology or biopsy of solid component or cyst wall (not shown).
Lipoma appears on HR-USG as well defined, superficially located in subcutaneous tissue, and is usually isoechoic but can appear Hyperechoic or Hypoechoic as well [20]. Our study showed Lipoma was one of the common benign lesions after Fibroadenoma seen in all age groups (not shown).
Galactocele is common finding in lactating mothers or in mothers who have recently stopped lactations. Blockage of milk duct is the main cause of Galactocele. Our patients presented with lumps during lactation. These on HR-USG appear as large commonly loculated or even complex cysts with moving echoes in it. Aspiration of milk confirms it (not shown).
Intraductal papilloma usually appears as well-defined echogenic lesions with smooth margins with in dilated duct or tubular cystic lesions. The common location for it is retroareolar region. The most of the patients presenting with nipple discharge or palpable retroareolar lump turn out to be intraductal papilloma or carcinoma [21]. On USG it is difficult to differentiate between papilloma and carcinoma. It is only confirmed on FNAC or Biopsy (Fig. 4).

Multiple dilated duct with echogenic solid areas in retroareolar region, later proved to be intraductal papillomas on cytology in a patient of 46 years of age
Inflammatory lesion is common in lactating women. Acute abscess present with fever, painful lump with skin redness and edema. Inflammatory lesion on Mammography is challenging for a Radiologist to differentiate from malignant lesion and appears as ill-defined irregular/speculated dense opacity (Fig. 5). Its findings on mammography mimic those of suspicious or malignant lesion and are only differentiated on HR-USG that shows ill-defined large, complex, irregular cystic or heterogeneous lesion that may show fluid movement in it (Fig. 6). Aspiration of pus or FNAC/Trucut biopsy confirms inflammatory lesion.

Mammogram showing ill-defined irregular opacity in right breast (black arrows) with overlying skin thickening (yellow arrow) labeled as BIRADS 5. HR USG revealed ill-defined irregular heterogeneous lesion that was divulged as inflammatory lesion on Trucut biopsy in a patient of 42 years of age

Abscess with irregular thick walled cystic lesion with echoes in it, on aspiration frank pus was aspirated in a young patient of 26 years of age with history of recent termination of breast feeding
Duct Ectasia is a benign condition seen most commonly in perimenopause age that occurs when a milk duct widens with thickening of its walls. This can cause the blockage of duct leading to fluid build-up. Common presentation is nipple discharge or lumpy feeling. HR USG reveals dilated ducts that are usually multiductal and bilateral [22].
Conclusions
Mass screening programs have proven pivotal role in early detection of breast cancer, but in developing countries where this service is not available, breast care clinics in tertiary care hospitals well equipped with imaging modalities play a significant role in fighting against breast cancer. So, it is recommended for developing countries that breast care clinics should be established at least in all tertiary care hospitals with trained and dedicated staff.
Availability of data and materials
Data and material is available for any kind of reference or use in future.
Abbreviations
- HR-USG:
-
High-Resolution Ultrasound
- FNAC:
-
Fine Needle Aspiration Cytology
- BIRADS:
-
Breast Imaging Reporting and Data System
References
Mukhtar R, Hussain M, Mukhtar MA, Ali SM (2020) Breast metastasis from medullary carcinoma of thyroid: a case report with literature view. JPMA J Pak Med Assoc 70(11):2051–2053
Saraswat S, Chandak S, Pratap V, Kumar A (2014) Sonomammographic evaluation and characterization of breast lumps. Int J Sci Study 1(4):50–53
Beerappa JR, Balu S, Kumar N (2016) Mammographic and sonomammographic evaluation of breast masses with pathological correlation: a prospective original study. Int J Anat Radiol Surg 5(3):9–12
Barton MB, Elmore JG, Fletcher SW (1999) Breast symptoms among women enrolled in a health maintenance organization: frequency, evaluation, and outcome. Ann Intern Med 130(8):651–657
Rotten D, Levaillant JM, Le Floch JP, Constancis E, André JM (1988) Mass screening for breast cancer with sonomammography: a prospective study. Eur J Obstet Gynecol Reprod Biol 28(3):257–267
Gonzaga MA (2010) How accurate is ultrasound in evaluating palpable breast masses? Pan Afr Med J 7(1):1–6
Mukhtar R, Mukhtar MA, Mushtaq S, Haider SR (2020) Fine needle aspiration cytology (FNAC) in combination with radiological imaging enhances the diagnostic accuracy of breast lesions in developing countries. Int J Sci Res Rev 9(4):20–27
Ekeh AP, Alleyne RS, Duncan AO (2000) Role of mammography in diagnosis of breast cancer in an inner-city hospital. J Natl Med Assoc 92(8):372
Malik G, Waqar F, Buledi GQ (2006) Sonomammography for evaluation of solid breast masses in young patients. J Ayub Med Coll Abbottabad 18(2):34–37
Evans WP (1995) Breast masses: appropriate evaluation. Radiol Clin N Am 33(6):1085–1108
Hooley RJ, Scoutt LM, Philpotts LE (2013) Breast ultrasonography: state of the art. Radiology 268(3):642–659
Jackson VP (1995) Management of solid breast nodules: what is the role of sonography? Radiology 196(1):14–15
Hansmann M, Hackelöer B-J, Staudach A (2012) Ultrasound diagnosis in obstetrics and gynecology. Springer, Berlin, pp 407–416. https://doi.org/10.1007/978-3-642-70423-9
Bassett LW, Gold RH, Kimme-Smith C (1985) Hand-held and automated breast ultrasound 19(12):204
Smallwood J, Guyer P, Dewbury K, Mengatti S, Herbert A, Royle G et al (1986) The accuracy of ultrasound in the diagnosis of breast disease. Ann R Coll Surg Engl 68(1):19
Mendelson EB, Berg WA, Merritt CR (2001) Toward a standardized breast ultrasound lexicon, BI-RADS: ultrasound. Semin Roentgenol 36(3):217–225
Hong AS, Rosen EL, Soo MS, Baker JA (2005) BI-RADS for sonography: positive and negative predictive values of sonographic features. Am J Roentgenol 184(4):1260–1265
Raza S, Chikarmane SA, Neilsen SS, Zorn LM, Birdwell RL (2008) BI-RADS 3, 4, and 5 lesions: value of US in management—follow-up and outcome. Radiology 248(3):773–781
Graf O, Helbich TH, Fuchsjaeger MH, Hopf G, Morgun M, Graf C et al (2004) Follow-up of palpable circumscribed noncalcified solid breast masses at mammography and US: can biopsy be averted? Radiology 233(3):850–856
Gao Y, Slanetz PJ, Eisenberg RL (2013) Echogenic breast masses at US: to biopsy or not to biopsy? Radiographics 33(2):419–434
Sabel MS, Helvie MA, Breslin T, Curry A, Diehl KM, Cimmino VM et al (2012) Is duct excision still necessary for all cases of suspicious nipple discharge? Breast J 18(2):157–162
Leung AKC, Kao CP (2004) Mammary duct ectasia: a cause of bloody nipple discharge. J Natl Med Assoc 96(4):543
Acknowledgements
Nil.
Funding
There is no funding body or sponsor for publication of this article.
Author information
Authors and Affiliations
Contributions
RM developed the idea and is the main author for manuscript writing. MH and MAM contributed to study design and manuscript writing and review. SR contributed to data collection, record and data analysis and helped in manuscript writing. All authors have reviewed the final version and approved it. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval from ethical committee of institute, MINAR Cancer Hospital was taken with reference Number of EC/MINAR- 008-2018 dated: 13-01-2018. As there was no experimental work involved human beings, so no need of informed consent.
Consent for publication
Not applicable as no identifying images or other personal or clinical details of participants are presented in manuscript.
Competing interests
All authors guarantee that there are no competing interests either directly or indirectly.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mukhtar, R., Hussain, M., Mukhtar, M.A. et al. Prevalence of different breast lesions in women of southern Punjab, Pakistan, characterized on high-resolution ultrasound and mammography. Egypt J Radiol Nucl Med 52, 245 (2021). https://doi.org/10.1186/s43055-021-00633-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-021-00633-8