
Abstract
Background
Adrenal hemangioma is a rare and non-functional benign tumor. Since the first case in 1955, approximately 90 cases have been reported in literature frequently presenting as a large and incidentally discovered retroperitoneal mass or as a result of hemorrhage caused by spontaneous rupture.
Case presentation
A 69-year-old man was admitted to our hospital for right hypocondrium pain and anemia. A computed tomography (CT) scan was performed and a large right adrenal mass measured 18 cm was found.
The patient underwent laparoscopic right adrenalectomy. Histopathological diagnosis revealed a cavernous adrenal hemangioma.
Conclusion
Cavernous hemangiomas are uncommon tumors. We reported a case of adrenal cavernous hemangioma incidentally discovered by ultrasound and CT. In the case of finding adrenal masses, cavernous hemangiomas, although rare, should be considered a possible diagnosis.
The appropriate treatment is surgical resection to rule out any potential for malignancy, to relieve symptoms secondary to the mass effect, and to prevent complications such as retroperitoneal bleeding.
Similar content being viewed by others


Background
Adrenal hemangioma is a rare and non-functional benign tumor. Since the first case in 1955, approximately 90 cases have been reported in literature [1], manifesting unspecifically with a retroperitoneal hemorrhage or found accidentally during diagnostic investigations performed for other reasons [2]. The clinical presentation of adrenal hemangiomas is usually vague, with non-specific abdominal pain [3]. Adrenal hemangiomas are indistinguishable from adrenal malignant tumors on imaging findings [4].
Case presentation
We report the case of a 69-year-old man, without a specific clinical history, referred 5 years ago to the radiology unit of our hospital for an abdominal discomfort of the right upper quadrant lasting a few months. The patient had no gastrointestinal symptoms or hematuria and did not report recent weight and appetite changes.
An ultrasound was performed which showed a clearly demarcated mass in the right hypocondrium, measuring 18 × 18 cm, with heterogeneous echogenicity, as for necrotic-hemorrhagic phenomena, probably of renal provenance, which compresses the right hepatic lobe (Fig. 1a, b).

a, b Abdomen ultrasound showed a demarcated mass probably of right renal provenance, measuring 18 × 18 cm, with heterogeneous echogenicity, as for necrotic-hemorrhagic phenomena
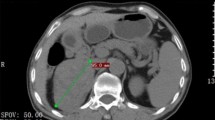
After a few days, the patient went to the hospital emergency room for right hypocondrium pain and anemia. A computed tomography (CT) scan was performed. It revealed a well-defined, ovoid, hypodense expansive lesion in the right adrenal lodge, which measured 18 × 18 × 15 cm with pericapsular speckled calcification and inhomogeneous density. It showed enhancement in arterial and venous phase, with peripheral vascular lacunae, suspected for active bleeding (Fig. 2a, b). The mass displaced the right kidney inferiorly, the pancreas to the left, and compressed the hepatic parenchyma, in the absence of signs of infiltration (Fig. 3a, b).

a, b CT with contrast revealed a well-defined expansive lesion in the right adrenal lodge, with inhomogeneous density. It showed enhancement in arterial (a) and venous (b) phase, with peripheral vascular lacunae (marked with the arrows)

Coronal (a) and sagittal (b) CT reconstruction with MIP technique showed the peripheral vascular lacunae (marked with the arrows) of the mass. The lesion displaced the right kidney inferiorly and compressed the hepatic parenchyma, without infiltration
Due to the non-specific radiological findings, the size of the lesion, and patient’s anemization, a surgical resection was decided the day after through an intraperitoneal laparoscopic right adrenalectomy. In this case, the laparoscopic approach was considered for the following reasons:
-
1.
No evidence of lesion malignancy (according to 2016 Clinical Practice Guidelines [5], the laparoscopic approach is the first choice in the case of benign lesions and also malignant at ≤ 6 cm, provided there are no signs of local infiltration/invasion)
-
2.
The laparoscopic approach initially had more of an “exploratory” intent (exploratory laparoscopy).
The surgery lasted 185 min and the patient lost about 180 cc of blood. He had not encountered postoperative complications and was discharged on the fourth day.
An adrenal mass, encapsulated in a fibrotic tissue, measuring 18 cm in maximum diameter and weighing 1200 g, was resected. Macroscopically, the mass had large hemorrhagic areas (Fig. 4a–c).

a–c Resection of adrenal mass, encapsulated in a fibrotic tissue (marked with a circle in c), with hemorrhagic areas, through an intraperitoneal laparoscopic right adrenalectomy
Pathological microscopic evaluation revealed a benign cavernous hemangioma, with hemorrhagic tissue in different stages of organization and endothelial vascular structures.
After 4 years from resection, CT follow-up was performed and there was no evidence of recurrence (Fig. 5a, b).

a, b CT follow-up performed 4 years after surgical removal. There was no evidence of relapse
Discussion
Cavernous hemangiomas are rare tumors. They are benign lesions that histopathologically consist of vascular lacunae lined by a single layer of endothelial cells [6].
Most are non-functioning tumors; only few secreting adrenal hemangiomas have been described until now [7].
Adrenal hemangiomas are mostly unilateral lesions, which appear between the ages of 50 and 70 years, more frequently in women (2:1 female-to-male ratio) [3].
Adrenal hemangiomas are often asymptomatic until the size of the mass has grown significantly and they are discovered accidentally during imaging studies [8]. The tumor size has ranged from 2 to 25 cm in diameter, and the weight has ranged from a few grams to 5 kg [6]. Our mass falls within these characteristics.
According to Noh et al., the most common symptom was flank pain or distress (21.2%) [8]. Our patient had a right upper quadrant abdominal pain.
Among the imaging methods to characterize the adrenal masses, ultrasound appearance is non-specific, hypoechogenic or heterogeneously echogenic [9], while CT is the more useful. On CT, the adrenal hemangioma appears as a well-encapsulated, heterogeneous, hypodense lesion that shows peripheral patchy enhancements on contrast-enhanced CT [10], with spotty calcifications probably due to phleboliths in dilated vascular spaces [7]. These characteristics are non-specific, because they are also present in other adrenal tumors; therefore, the definitive diagnosis is postoperative, after histopathological evaluation [7, 8].
It is important to make a differential diagnosis with renal tumors, other adrenal tumors, and metastases of breast, renal, gastrointestinal, lung, and melanoma cancers [11]. On histopathological inspection, cavernous hemangiomas consist of blood-filled sinusoidal canals that, especially at the periphery of the lesion, determine the characteristic pattern of peripheral patchy contrast enhancement seen on CT imaging [11]. Most of these tumors may have areas of thrombosis, hemorrhage, necrosis, and contextual calcifications [6].
On other useful imaging modality is magnetic resonance. It may show homogeneous well-encapsulated masses hypointense on T1-weighted images with central hyperintense signal and with hyperintense signal on T2-weighted images, as a consequence of bleeding and calcification [1, 6]. Our patient did not perform this exam due to his clinical condition.
The indications for resection of this neoplasm are for masses larger than 3.5 cm, to relieve mass effect symptoms, to exclude malignant tumors, and to avoid complications such as retroperitoneal hemorrhage and rupture [12]. Our patient had a lesion of about 18 cm and was anemic, so he underwent urgent right adrenalectomy with an intraperitoneal laparoscopic approach.
Conclusions
In summary, we reported a case of adrenal cavernous hemangioma discovered by ultrasound and CT, the diagnosis of which was confirmed by histopathological examination. In the case of finding adrenal masses, cavernous hemangiomas, although rare, should be part considered a possible diagnosis. The appropriate treatment is surgical removal to rule out any potential for malignancy, to relieve symptoms secondary to the mass effect, and to prevent complications such as retroperitoneal bleeding.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CT:
-
Computed tomography
- cc:
-
Cubic centimeter
References
Al-Rawashdah S, Mansi H, Carbone A (2021) Adrenal cavernous hemangioma; a rare diagnosis of adrenal incidentaloma: a case report, and literature review. Urol Case Rep 34:101477
Nishtala M, Cai D, Baughman W, McHenry CR (2019) Adrenal cavernous hemangioma: a rare tumor that mimics adrenal cortical carcinoma. Surg Open Sci. 1(1):7–13. https://doi.org/10.1016/j.sopen.2019.04.001
Quildrian SD, Silberman EA, Vigovich FA, Porto EA (2013) Giant cavernous hemangioma of the adrenal gland. Int J Surg Case Rep. 4(2):219–221. https://doi.org/10.1016/j.ijscr.2012.11.022
Pang C, Wu P, Zhu G (2015) A rare cavernous hemangioma of the adrenal gland. Urol Case Rep 3(4):120–122. https://doi.org/10.1016/j.eucr.2015.03.009
Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A, Tabarin A, Terzolo M, Tsagarakis S, Dekkers OM (2016) Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol 175(2):G1–G34. https://doi.org/10.1530/EJE-16-0467
Wang L, Dang Y, He R, Chen G (2014) Rare cavernous hemangioma of adrenal gland: case report. Sao Paulo Med J. 132(4):249–252. https://doi.org/10.1590/1516-3180.2014.1324715
Feo CV, De Troia A, Pedriali M, Sala S, Zatelli MC, Carcoforo P, Feo CF (2018) Adrenal cavernous hemangioma: a case report. BMC Surg. 18(1):103. https://doi.org/10.1186/s12893-018-0429-9
Noh JJ, Choi SH, Hwang HK, Kang CM, Lee WJ (2014) Adrenal cavernous hemangioma: a case report with review of the literature. JOP. 15(3):254–257. https://doi.org/10.6092/1590-8577/2402
Foresti M, Parmiggiani A (2019) Adrenal adenoma-hemangioma collision tumor: description of two cases. J Radiol Case Rep. 13(6):1–12. https://doi.org/10.3941/jrcr.v13i6.3691
Yamada T, Ishibashi T, Saito H, Majima K, Tsuda M, Takahashi S, Moriya T (2002) Two cases of adrenal hemangioma: CT and MRI findings with pathological correlations. Radiat Med. 20(1):51–56
Arkadopoulos N, Kyriazi M, Yiallourou AI, Stafyla VK, Theodosopoulos T, Dafnios N, Smyrniotis V, Kondi-Pafiti A (2009) A rare coexistence of adrenal cavernous hemangioma with extramedullar hemopoietic tissue: a case report and brief review of the literature. World J Surg Oncol. 7(1):13. https://doi.org/10.1186/1477-7819-7-13
Forbes TL (2005) Retroperitoneal hemorrhage secondary to a ruptured cavernous hemangioma. Can J Surg 48:78–79
Acknowledgements
No acknowledgements
Funding
The authors received no financial sponsors or other funding for this research.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. The case was followed up clinically and surgically by LE, WG, and VF. Material collection was performed by VT, LE, and WG. All authors (VT, LE, WG, VF, FB, and GG) participated in the writing of the paper. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
The patients gave the written consent to publish images and other personal or clinical details. The consent to publish this information was obtained from study participant.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Testini, V., Eusebi, L., Giannubilo, W. et al. Imaging findings and 4 years follow-up of adrenal cavernous hemangioma: a case report. Egypt J Radiol Nucl Med 52, 169 (2021). https://doi.org/10.1186/s43055-021-00552-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-021-00552-8