
Abstract
Background
The proximity of the maxillary sinus floor to the maxillary molar roots increases the probability of oroantral communication on conducting any surgical or endodontic procedure in the involved area. The aim of this study is to evaluate the relationship between each maxillary molar root and maxillary sinus floor using cone beam computed tomography. Predicting the probability of protrusion of each root into the sinus will consequently predict the probability of occurrence of the oroantral fistula in a sample of the Egyptian population.
Results
The total number of roots located outside the sinus was 121 (35.3%), while those contacting the sinus floor were 80 (23.3%) and those intruded the sinus were 141 (41.2%). The percentage of root intrusion into the sinus in males (56.9%) was significantly (p = 0.01) higher than females (42.9%). The probability of root intrusion in the left molars (54.2%) was non-significantly (p = 0.067) higher than that of the right side (44.3%). As for the type of tooth, the second molar showed the highest probability of root intrusion into the sinus (55.3%) followed by the third molars (52.6%) then the first molars (40.9). According to the type of root, the mesiobuccal root showed the highest probability of intrusion into the sinus (50.9%) followed by the palatal root (49.1%) then the distobuccal root (47.4%). However, the difference in both type of tooth and type of root was statistically non-significant (p = 0.051 and 0.869 respectively). As for the individual root with the highest probability of intrusion, the mesio-buccal root of the right third molar is the most frequent root to intrude the sinus (71.4%) and the mesio-buccal root of the right first molar is the least frequent (22.7%).
Conclusions
In a sample of the Egyptian population, males exhibit higher probability of root protrusion into the sinus than females. The side and type of tooth are of higher impact on the probability of its intrusion into the sinus compared to the type of root. Left second molars are at a higher risk of oroantral communications on surgical or endodontic procedures compared to other molars due to its highest probability of intrusion into the sinus.
Similar content being viewed by others

Background
The maxillary sinuses (MS) are one of the four paired sets of the paranasal sinuses and the first to develop in fetal life [1]. It is considered the most important paranasal sinus that impacts most of the work of the dentists and the maxillofacial surgeons [2]. This is due to the close proximity of its floor to the apices of the premolar and molar roots that are separated from the sinus floor either by a thin layer of bone or by its mucous membrane which is called Schneiderian membrane [3].
The sinus becomes at a risk of exposure to the oral cavity either due to a surgical procedure carried out in the area of the maxillary posterior teeth or due to a pathologic invasion from a lesion arising from this area. This leads to the occurrence of the popular accident known as oroantral fistula or oroantral communication. This accident, which has always been a concern for dental practitioners, consists in the violation of the maxillary sinus floor (MSF) and may or may not involve tearing of the Schneiderian membrane [4].
Having a previous idea about the high probability of the occurrence of an oroantral communication may strongly affect the treatment plan. A general practitioner may prefer to refer this case to a maxillofacial surgeon who should bear in mind that it is a complicated procedure that may require the closure of the fistula by one of the following methods: local flaps, distant flaps, and grafting. These include rotating or advancing soft tissues such as palatal flap, submucosal tissue, buccal flap, submucosal tissue, buccal fat pad, and tongue flap [5].
The two-dimensional (2D) imaging, represented in the periapical and the panoramic radiography, is considered the most widely available modality that provides acceptable data with minimal dose and cost. However, cone beam computed tomography (CBCT) was the imaging modality used by most of the researchers to study the sinus-root relation. This is related to its three-dimensional nature that can provide information that was lost or restricted due to superimposition, magnification, and blurring of the 2D imaging [6, 7].
Many studies used different scoring systems to categorize the sinus-root relation in different populations [8,9,10,11,12,13,14,15]. The simplest of all these systems consists of three classes, class 1: root tip is outside the sinus, class 2: root tip is against the sinus wall, and class 3: root tip is in the sinus [16,17,18,19,20,21]. The most popular classification was that introduced by Kwak et al. [22] and it was widely implemented by researchers [23, 24]. Other studies depended on the linear measurements in the involved area [25,26,27].
Many studies were concerned with analyzing the sinus-root relation in different populations including the Chinese [9, 28], Iranian [11, 26], Brazilian [29, 30], Bulgarian [25], and Saudi Arabian [14] populations. The aim of this study is to assess the relationship between the roots of the maxillary molars and MSF in a sample of the Egyptian population—that was not involved in any previous study—using CBCT.
Methods
Study design and population
This is an observational descriptive study that comprised 342 maxillary molar roots from 23 male and female Egyptian patients who were referred by their dentists to the Department of Oral and maxillofacial radiology in Faculty of Dentistry, at our University to undergo CBCT scanning on the maxillary arch for different purposes including implant planning, maxillofacial surgery, FDASU-Rec IM121804. Patients were recruited in the period between October 2019 and October 2020. From a total of 35 patients, only those who consented to participate in this study were included. They were selected according to the following criteria:
Inclusion criteria:
-
1-
Patients should have at least two normally erupted upper molars on each side.
-
2-
Patient’s age should be above 23 years.
Exclusion criteria:
-
1-
Roots with chronic periapical lesions, root abnormalities (e.g., external resorption), or any radiological evidence of intraosseous pathology (e.g., cysts or tumors).
-
2-
Supernumerary and supplemental teeth.
Ethical consent
The study was approved by the Research Ethics Committee of the Faculty of Dentistry—approval number FD….-Rec IM121804. All patients were informed about the nature and the purpose of the study and were asked to sign a written informed consent.
Observation and scoring
The CBCT images were obtained using i-CAT Next Generation scanner (Imaging Sciences International, Hatfield, PA, United States) operating at tube voltage 120 kVp, tube current 5 mA, voxel size 0.2 mm, field of view 16 × 6 cm and scanning time 26.9 s. Images were observed by three oral radiologists independently, with minimum of 3 years of experience in CBCT images interpretation.
For standardization, all the observers agreed on a certain protocol for observation to decrease bias. The observation was performed for each molar on each side on the coronal cuts of the multiplanar reconstruction screen (MPR) of i-CAT Vision viewer software (version 1.9.3.13 provided by Imaging Sciences International, USA). They were allowed to use the zoom tool and to change the brightness, contrast, and sharpness if they felt necessary [16].
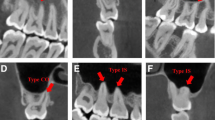
Images were classified and given a score as follows (Fig. 1): score 1: when the root apex is placed outside the sinus, score 2: when the root apex is just contacting the sinus floor, and score3: when the root apex is projected into the sinus [14,15,16,17,18,19].

Cropped CBCT coronal cuts, a shows roots with score 1, b shows root with score 2, and c shows root with score 3
Statistical analysis
The interrater reliability between the observers was detected using Fleiss’s Kappa test. All the data were collected and any disagreement between the observers about the result was solved by consensus. Chi-square test was used to analyze the effect of gender, type of tooth (first or second or third molar), the involved side (right or left), and type of root (mesiobuccal, distobuccal, or palatal) on the intrusion of root into the sinus. The level of statistical significance was set at p value < 0.05. In this categorial analysis scores 1 and 2 were collectively representing the placement of the root outside the sinus., while score 3 represents its placement inside the sinus. Contingency cross-tables for each score were created in terms of frequency and percentages for the side, type of tooth, and the type of root. All statistical analysis was performed using IBM SPSS Statistics.
Case presentation
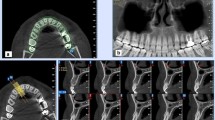
A 32-year-old female patient was referred by her dentist to the Oral and Maxillofacial Radiology department, Faculty of Dentistry, at our University to undergo a maxillary CBCT imaging for immediate implant placement in the anterior maxilla. All the required criteria were present in this patient. She was informed by the nature of the study and she signed a written consent. CBCT images (Figs. 2 and 3) were assessed on the MPR screen of the i-Cat Vision Viewer and the scores were recorded in Table 1.

Cropped coronal cuts for a the mesiobuccal root of the right first maxillary molar, b distobuccal and palatal roots (image b) of the right first maxillary molar, c the mesiobuccal root of the right second maxillary molar, d distobuccal and palatal roots of the right second maxillary molar, e the buccal root of the right third maxillary molar, and f the palatal root of the right third maxillary molar

Cropped coronal cuts for a the mesiobuccal root of the left first maxillary molar, b distobuccal and palatal roots of the left first maxillary molar, c the mesiobuccal root of the left second maxillary molar, d distobuccal and palatal roots of the left second maxillary molar, and e the fused roots of the left third maxillary molar
Results
Using Fleiss’s Kappa test, the interrater reliability between the observers upon CBCT images was overall very good, excellent at roots away from the sinus floor (score 1), very good at roots at the sinus floor (score 2), and excellent at roots inside the sinus (score 3) (Fig. 4).

Interrater reliability between the observers upon CBCT images
The total number of roots involved in this study is 342, 121 of them are located outside the sinus (score 1), 80 of them contact the sinus floor (score 2), and 141 intrude the sinus (score 3) (Fig. 5).

Percentage of each of the three scores
According to the demographic data of the participants, this study involved 23 patients aged 33.4 ± 10.7 [mean ± standard deviation] 10 of which were males with a total of 153 roots and 13 of them were females with a total of 189 roots. Table 2 demonstrates the number and percentage of the roots intruding and extruding the sinus in each gender and reveals that the percentage of intrusion of the roots into the sinus in males was significantly higher (56.9%) than females (42.9%) (p = 0.01).
The statistical analysis of the prevalence of intrusion and extrusion of the roots of each side, each of the three molars and each type of root separately is demonstrated collectively in Table 3. It reveals that the probability of root intrusion in the left molars (54.2%) was non-significantly (p = 0.067) higher than that of the right side (44.3%). As for the type of tooth, the second molar showed the highest probability of root intrusion into the sinus (55.3%) followed by the third molars (52.6%) then the first molars (40.9). According to the type of root, the mesiobuccal root showed the highest probability of intrusion into the sinus (50.9%) followed by the palatal root (49.1%) then the distobuccal root (47.4%). However, the difference in both type of tooth and type of root was statistically non-significant (p = 0.051 and 0.869 respectively).
The frequency and percentage of occurrence of each root in the three scores regarding its type, tooth, and side is shown in Table 4 and Fig. 6.

Percentage of occurrence of each root in each of the 3 scores
The mesiobuccal root of the right third molar is the most frequent root to be inside the sinus with 71.4% and the mesiobuccal root of the right first molar is the least one with 22.7%. The most frequent root to be just contacting the sinus floor is the distobuccal root of the left third molar with 30.7% and the least one is the palatal root of the left first molar with 4.5%. Lastly, the most frequent root to be outside the sinus is the mesiobuccal root of right first molar with 54.5% and the least frequent one is the mesio-buccal root of the left second molar with 13% (Fig. 6).
Discussion
The study demonstrates the probability of intrusion of each root of the maxillary molar teeth into the MS in a sample of the Egyptian population that was not involved in any previous study. This alerts the operator to the probability of undesirable complications of oroantral communication allowing him to take all the appropriate precautions before carrying out any invasive procedure in the maxillary posterior region.
Patients were selected to have at least two normally erupted upper molars on each side to include the largest number of roots within the smallest acceptable sample size. Only patients older than 23 years were included to ensure the complete eruption and formation of both the upper molars and MS [31, 32].
Premolars were not involved in the current study since many studies performed during the last decade agreed that the premolars roots are rarely in contact with the MSF and they represent the lowest risk of oro-antral communication [14, 15, 18, 23, 25, 29, 33,34,35,36]. Roots with chronic periapical lesions and root abnormalities were excluded to avoid any confusion in the observation. Supernumerary and supplemental teeth were excluded because of their confusing abnormal shapes and positions.
Among all radiographic techniques, CBCT was the imaging technique used in this study because of its tomographic nature, high contrast and accuracy in evaluating the sinus floor without any superimposition, and magnification or blurring in comparison to conventional imaging [7, 10, 27]. The i-CAT Next Generation scanner with its proprietary software was used in image acquisition and observation in this study following the track of many other studies, because of its availability, high image resolution, and ease of manipulation [19, 27, 29, 30, 37].
The relation between the MSF and the root tips of the maxillary posterior teeth was categorized by many studies [8,9,10,11,12,13,14,15,16,17,18,19,20,21, 23, 24]. The classification used in the current study was previously documented by many authors in different studies [16,17,18,19,20,21]. It is represented in class 1: root tip is outside the sinus, class 2: root tip is against the sinus wall, and class 3: root tip is in the sinus. This scoring system was implemented in this study due to its simplicity.
A popular and more complicated classification proposed by Kwak et al. [22] and implemented by Razumova et al. [23] and Ali et al. [24] is represented as type I: the inferior wall of the MS is located above the root apex of the buccal and palatal roots, type II: the inferior wall of the MS is located below the level connecting the buccal and palatal root apices without an apical protrusion over the MS, type III: an apical protrusion of the buccal root apex is observed over the inferior wall of the MS, type IV: an apical protrusion of the palatal root apex is observed over the inferior wall of the MS, and type V: apical protrusions of the buccal and palatal root apices are observed over the inferior wall of the MS.
The interrater reliability between the observers upon the images was high because of the high image quality, standardization of all exposure factors, and the good experience of the three observers in the field of oral radiology especially CBCT images.
The result of the present study revealed that, from a total of 342 maxillary molar roots of the Egyptian population, 35.3% was located outside the sinus, 23.4% contacted the sinus floor, and 41.2% protruded the sinus. While Estrela et al. [29], who implemented a closely related scoring system in studying the Brazilian population also using the i-CAT Vision CBCT software (Imaging Sciences International, USA), reported that 25.16% out of 600 maxillary molar were located outside the sinus, 40.67% contacted the sinus floor, and 34.17% protruded the sinus. This difference in the results is related to difference in populations and sample size.
Pagin et al. [30] performed another study on the Brazilian population to assess the sinus-root relation also using i-CAT Vision CBCT software (Imaging Sciences International, USA). They reported that from a total of 601 maxillary tooth root 130 roots (21.6%) were in close contact with the MSF without sinus floor elevation which is considered a very close percentage to that of the current study that was 23.4%. While 86 roots (14.3%) were protruded into the sinus producing an elevation of the bony cortex and that was far away from the percentage of the current study that was 41.2%. This difference may be related to the difference in populations and sample size.
Haghanifar et al. [11] used on Demand CBCT software (Cybermed, Korea) to categorize the sinus-root relation in the Iranian population. They reported that from a total of 419 maxillary molar, 23.9% were located outside the sinus, while the current study reported that 35.3% of the roots were outside the sinus. They reported that 66.6% contacted the sinus floor which is considered a very high percentage compared to that of the current study represented in 23.4%. Only 9.5% protruded the sinus and this is a very low percentage compared to that of the current study represented in 41.2%. This obvious discrepancy between the two studies is related to the difference in populations, sample size and CBCT software used in observation.
Zhang et al. [28] studied the sinus-root relation in the Chinese population on a total of 800 right and left first and second molars using CBCT images without mentioning the employed software. They nearly agreed with the current study in the percenatge of the roots contacting the sinus floor where they reported 21.75% and this study reported 23.4%. The major difference between both studies was represented in the percentage of roots located outside the sinus and intruding the sinus. They reported that 57.1% of these teeth were placed outside the sinus and 21.23% protruded the sinus, while the percentages of the current study was 35.3% and 41.2% respectively. The discripancy between both studies in reporting the sinus-root relation may be due to differences in populations, manipulated softwares, and sample size. Moreover, they involved only the first and second molars while the current study included the three maxillary molars.
A study implemented by Mattar et al. [14] that involved panoramic images of 266 premolar and molar tooth from a sample of the Saudi Arabian population reported that 37.6% of the teeth were outside the sinus, 20.3% contacted the sinus floor, and 42.1% of the teeth protruded the sinus. Despite the difference in sample size, technique used, and the involvement of the premolars, these results are considered the closest of all previously mentioned ones to ours. This high degree of agreement between the two studies may be related to the similarity of both populations being both Arabian and exhibiting similar circumstances.
The current study reported that—in a sample of the Egyptian population—gender is an influencing factor to the intrusion of roots into the sinus where the involved probability is significantly higher in males than in females. The result of this study agreed with Shokri et al. [10] and Haghanifar et al. [11] who reported that males are more susceptible to root protrusion into the sinus than females of the Iranian population. Also Kilic [33] reported the same result; however, he did not specify a certain population. While Gu Yehen et al. [18] and Pei et al. [9] who evaluated the relationship between the maxillary posterior teeth and MSF in the chinese population reported the little influence of gender on this relation.
Despite approaching the traditional threshold of statistical significance, we cannot assert that the left molars are of higher probability of intrusion into the sinus in relation to the right ones in the involved sample of the Egyptian population. A number of studies reached the same result including Shokri et al. [10], Kilic [33], and Pei et al. [9].
Concerning the probability of intrusion of each molar as a whole, the p value approached the threshold of statistical significance but did not reach it. Therefore, we also can not assert that the second molar has the highest probability of intrusion into the sinus in the involved sample of the Egyptian population although it exceeded the percentage of the third and first molars by 3% and 15% respectively. Georgiev et al. [25] also reported that the maxillary second molar was the most common teeth to project into the sinus in patients from the Varna region in Bulgaria.
The influence of the type of root on its probability of intrusion into the sinus is very limited as the three types (mesiobuccal, distobuccal, and palatal) had very close intrusion probabilities and the p value was far away from the threshold of statistical significance (p = 0.869).
As for the individual root with the highest probability of intrusion, the current study reported that the mesio-buccal root of the right third molar is the most frequent root to be inside the sinus and the mesio-buccal root of the right first molar is the least frequent. However, many studies recently carried out agreed that the mesiobuccal root of the maxillary second molar is the closest root to the MSF among all maxillary teeth roots [8, 9, 15, 19, 23, 28, 30, 34, 36, 38, 39].
While other studies agreed that the distobuccal root of the maxillary second molar is the closest to the MSF with the highest risk of oro-antral communication [25, 26, 33, 40, 41]. However, Kaushik et al. [17] and Didilescu et al. [27] concluded that the roots of the first maxillary molar are the nearest to the MSF among all posteriors. Didilescu et al. [27] specified the palatal root of the involved tooth with this close relation.
Limitations
One limitation of this study is the small sample size. A larger sample size could have allowed more subgroup analysis to be implemented including the patients age. Besides, the statistical significance of the side and type of the tooth on its relation to the sinus could have been more reliable with a larger sample size.
Another limitation of this study is that it was a single-center study. The study results could have been more representative to the Egyptian population if the participants were recruited from different study centers not from a single dental facility.
Conclusions
In a sample of the Egyptian population, males exhibit higher probability of root protrusion into the sinus than females. The side and type of tooth are of higher impact on the probability of its intrusion into the sinus compared to the type of root. Left second molars are at a higher risk of oroantral communications on surgical or endodontic procedures compared to other molars due to its highest probability of intrusion into the sinus. For future research, it is recommended to investigate the influence of age on the sinus-root relation in the Egyptian population.
Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MS:
-
Maxillary sinus
- MSF:
-
Maxillary sinus floor
- 2D:
-
Two-dimensional
- CBCT:
-
Cone beam computed tomography
- MPR:
-
Multiplanar reconstruction
References
Nurbakhsh B, Friedman S, Kulkarni GV, Basrani B, Lam E (2011) Resolution of maxillary sinus mucositis after endodontic treatment of maxillary teeth with apical periodontitis: A cone-beam computed tomography pilot study. J Endod 37(11):1504–1511. https://doi.org/10.1016/j.joen.2011.07.007
Dobele I, Kise L, Apse P, Kragis G, Bigestans A (2013) Radiographic assessment of findings in the maxillary sinus using cone-beam computed tomography. Stomatologija 15(4):119–122
Okada T, Kanai T, Tachikawa N, Munakata M, Kasugai S (2016) Long-term radiographic assessment of maxillary sinus floor augmentation using beta-tricalcium phosphate: analysis by cone-beam computed tomography. Int J Implant Dent 2(1):8. https://doi.org/10.1186/s40729-016-0042-6
Lopes LJ, Gamba TO, Bertinato JVJ, Freitas DQ (2016) Comparison of panoramic radiography and CBCT to identify maxillary posterior roots invading the maxillary sinus. Dentomaxillofacial Radiol 45(6):20160043. https://doi.org/10.1259/dmfr.20160043
Nedir R, Nurdin N, Paris M, El Hage M, Abi Najm S, Bischof M (2017) Unusual etiology and diagnosis of oroantral communication due to late implant failure. Case Rep Dent 2017(1):1–5
Low KMT, Dula K, Bürgin W, von Arx T (2008) Comparison of periapical radiography and limited cone-beam tomography in posterior maxillary teeth referred for apical surgery. J Endod 34(5):557–562. https://doi.org/10.1016/j.joen.2008.02.022
Alaqel S (2016) Comparing panoramic radiography with Cone beam computed tomography (CBCT) in the detection of anatomical structures and its effect on treatment planning in the placement of implants in the posterior region of the mandible and maxilla (a Pilot Study). ProQuest Dissertations and Theses.
Binhuwaishel LA (2020) Proximity differences of maxillary posterior root apices to the maxillary sinus floor according to different skeletal patterns: a retrospective CBCT study. ProQuest Dissertations and Theses. 2020
Pei J, Liu J, Chen Y, Liu Y, Liao X, Pan J (2020) Relationship between maxillary posterior molar roots and the maxillary sinus floor: Cone-beam computed tomography analysis of a western Chinese population. J Int Med Res 48(6):300060520926896. https://doi.org/10.1177/0300060520926896
Shokri A, Lari S, Yousefi F, Hashemi L (2015) Assessment of the relationship between the maxillary sinus floor and maxillary posterior teeth roots using cone beam computed tomography. J Contemp Dent Pract 15(5):618–622
Haghanifar S, Moudi E, Bijani A, Arbabzadegan N (2018) Relationship between the maxillary molars roots and sinus in a selected iranian population : a CBCT study. J Res Med Dent Sci 6(2):544–549
Sun W, Xia K, Tang L, Liu C, Zou L, Liu J (2018) Accuracy of panoramic radiography in diagnosing maxillary sinus-root relationship: a systematic review and meta-analysis. Angle Orthod 88(6):819–829. https://doi.org/10.2319/022018-135.1
Dehghani M, Motallebi E, Navabazam A, Montazerlotfelahi H, Ezoddini F, Ghanea S (2017) The relation between maxillary sinus floor and posterior maxillary teeth roots using panoramic and cone beam computed tomography. J Dentomaxillofacial Radiol Pathol Surg 6(3):49–60
Mattar E, Hammad L, Faden A, Khalil H (2010) Relation of maxillary teeth to the maxillary sinus in normal Saudi individuals living in Riyadh. Biosci Biotechnol Res Asia 7(2):695–700
Tang L, Xu L, Liu H (2019) A retrospective study on the relationship between maxillary posterior teeth and maxillary sinus floor using cone-beam computed tomographic images. J Anat Soc India 68(4):253–259
Hassan B (2010) Reliability of periapical radiographs and orthopantomograms in detection of tooth root protrusion in the maxillary sinus: correlation results with cone beam computed tomography. J Oral Maxillofac Res 1(1):e6. https://doi.org/10.5037/jomr.2010.1106
Kaushik M, Kaushik P, Mehra N, Sharma R, Soujanya E, Kumar U (2020) Anatomical relationship between roots of maxillary posterior teeth and maxillary sinus using cone—beam computed tomography. Endodontology 32(3):124–129, Anatomical relationship between roots of maxillary posterior teeth and maxillary sinus using cone-beam computed tomography, DOI: https://doi.org/10.4103/endo.endo_25_20.
Gu Y, Sun C, Wu D, Zhu Q, Leng D, Zhou Y (2018) Evaluation of the relationship between maxillary posterior teeth and the maxillary sinus floor using cone-beam computed tomography. BMC Oral Health 18(1):164. https://doi.org/10.1186/s12903-018-0626-z
Makris LML, Devito KL, D’Addazio PSS, Lima CO, Campos CN (2020) Relationship of maxillary posterior roots to the maxillary sinus and cortical bone: a cone beam computed tomographic study. Gen Dent 68(2):e1–e4
Bokkasam V, Muddepalli P, Jayam R, Devaki S, Pakerla A, Koduri S (2015) Comparison of panoramic radiograph with cone-beam computed tomography in assessment of maxillary sinus floor and nasal floor. J Indian Acad Oral Med Radiol 27(2):194
Terlemez A, Tassoker M, Kizilcakaya M, Gulec M (2019) Comparison of cone-beam computed tomography and panoramic radiography in the evaluation of maxillary sinus pathology related to maxillary posterior teeth: Do apical lesions increase the risk of maxillary sinus pathology? Imaging Sci Dent 49(2):115–122. https://doi.org/10.5624/isd.2019.49.2.115
Kwak HH, Park HD, Yoon HR, Kang MK, Koh KS, Kim HJ (2004) Topographic anatomy of the inferior wall of the maxillary sinus in Koreans. Int J Oral Maxillofac Surg 33(4):382–388. https://doi.org/10.1016/j.ijom.2003.10.012
Razumova S, Brago A, Howijieh A, Manvelyan A, Barakat H, Baykulova M (2019) Evaluation of the relationship between the maxillary sinus floor and the root apices of the maxillary posterior teeth using cone-beam computed tomographic scanning. J Conserv Dent 22(2):139–143. https://doi.org/10.4103/JCD.JCD_530_18
Ali SM, Hawramy FA, Mahmood KA (2012) The relation of maxillary posterior teeth roots to the maxillary sinus floor using panoramic and computed tomography imaging in a sample of Kurdish people. Tikrit J Dent Sci 1(2):81–88
Georgiev D, Peev S, Arnautska H (2015) Relationship between root apices of maxillary posterior teeth and the maxillary sinus floor in patients from the Varna region. J Med Dent Pract 2(4):300–369. https://doi.org/10.18044/MedInform.201524.300
Tafakhori Z, Masoudi M (2018) Evaluating the distance between posterior teeth and the maxillary sinus floor using cone beam computed tomography (CBCT). J Dentomaxillofacial Radiol Pathol Surg 7(4):145–150
Didilescu A, Rusu M, Săndulescu M, Georgescu C, Ciuluvică R (2012) Morphometric analysis of the relationships between the maxillary first molar and maxillary sinus floor. Open J Stomatol 2(4):352–357. https://doi.org/10.4236/ojst.2012.24060
Zhang X, Li Y, Zhang Y, Hu F, Xu B, Shi X, Song L (2019) Investigating the anatomical relationship between the maxillary molars and the sinus floor in a Chinese population using cone-beam computed tomography. BMC Oral Health 19(1):282. https://doi.org/10.1186/s12903-019-0969-0
Estrela C, Nunes CABCM, Guedes OA, Alencar AHG, Estrela CRA, Silva RG, Pécora JD, Sousa-Neto MD (2016) Study of anatomical relationship between posterior teeth and maxillary sinus floor in a subpopulation of the Brazilian central region using cone-beam computed tomography – Part 2. Braz Dent J 27(1):9–15. https://doi.org/10.1590/0103-6440201600679
Pagin O, Centurion BS, Rubira-Bullen IRF, Alvares Capelozza AL (2013) Maxillary sinus and posterior teeth: accessing close relationship by cone-beam computed tomographic scanning in a Brazilian population. J Endod 39(6):748–751. https://doi.org/10.1016/j.joen.2013.01.014
Köhler S, Schmelzle R, Loitz C, Püschel K (1994) Development of wisdom teeth as a criterion of age determination. Ann Anat 176(4):339–345. https://doi.org/10.1016/S0940-9602(11)80513-3
Lorkiewicz-Muszyńska D, Kociemba W, Rewekant A, Sroka A, Jończyk-Potoczna K, Patelska-Banaszewska M, Przystańska A (2015) Development of the maxillary sinus from birth to age 18. Postnatal growth pattern. Int J Pediatr Otorhinolaryngol 79(9):1393–1400. https://doi.org/10.1016/j.ijporl.2015.05.032
Kilic C, Kamburoglu K, Yuksel SP, Ozen T (2010) An assessment of the relationship between the maxillary sinus floor and the maxillary posterior teeth root tips using dental cone-beam computerized tomography. Eur J Dent 4(4):462–467
Hussein ZA, Al-Nakib LH (2013) Assessment of the relationship between maxillary sinus floor and maxillary posterior teeth root apices using spiral CT scan. J Baghdad Coll Dent 25(3):80–86. https://doi.org/10.12816/0015001
Von Arx T, Fodich I, Bornstein MM (2014) Proximity of premolar roots to maxillary sinus: a radiographic survey using cone-beam computed tomography. J Endod 40(10):1541–1548. https://doi.org/10.1016/j.joen.2014.06.022
Jang JK, Kwak SW, Ha JH, Kim HC (2017) Anatomical relationship of maxillary posterior teeth with the sinus floor and buccal cortex. J Oral Rehabil 44(8):617–625. https://doi.org/10.1111/joor.12525
Lavasani SA (2015) CBCT measurements of maxillary molars and relation to the buccal/palatal plate and sinus. ProQuest Dissertations and Theses.
Lavasani SA, Tyler C, Roach SH, McClanahan SB, Ahmad M, Bowles WR (2016) Cone-beam computed tomography: anatomic analysis of maxillary posterior teeth—impact on endodontic microsurgery. J Endod 42(6):890–895, Cone-beam Computed Tomography: Anatomic Analysis of Maxillary Posterior Teeth—Impact on Endodontic Microsurgery, DOI: https://doi.org/10.1016/j.joen.2016.03.002.
Oishi S, Ishida Y, Matsumura T, Kita S, Sakaguchi-Kuma T, Imamura T, Ikeda Y, Kawabe A, Okuzawa M, Ono T (2020) A cone-beam computed tomographic assessment of the proximity of the maxillary canine and posterior teeth to the maxillary sinus floor: Lessons from 4778 roots. Am J Orthod Dentofac Orthop 157(6):792–802. https://doi.org/10.1016/j.ajodo.2019.06.018
Asthana G, Bhargava S, Parmar GJ (2015) Proximity of maxillary sinus floor to the roots of maxillary molars: a CBCT evaluation. Endodontology 27(1):47–51
Pagariya N, Chourasiya R, Banerjee PK, Rangari P (2018) Evaluating the relationship between the maxillary molar roots and maxillary sinus floor—a retrospective study using cone-beam computerized tomography. Int J Med Sci Diagnosis Res 2(5):78–85.
Acknowledgements
We gratefully acknowledge Dr. Kareem Samir for his efforts in observation and statistical analysis, Dr. Amr Ramah for his aid in observation, and Dr. Haneen Mousa for her endless support.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
EA performed the data collection, analysis, interpretation, and wrote the primary manuscript. FE aided in designing the study and optimizing the study methodology. WH performed the final revision and supervision. All authors offered meticulous aid in writing and editing the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Research Ethics Committee of the Faculty of Dentistry Ain-Shams University, approval number FDASU-Rec IM121804. All patients signed a written consent that explained the procedure involved in this study.
Consent for publication
All patients included in this research gave written informed consent to publish the data contained within this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eid, E.A., El-Badawy, F.M. & Hamed, W.M. Intrusion of maxillary molar roots into the maxillary sinus in a sample of the Egyptian population using cone beam computed tomography. Egypt J Radiol Nucl Med 52, 163 (2021). https://doi.org/10.1186/s43055-021-00540-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-021-00540-y