
Abstract
Background
Bone scintigraphy is an appropriate tool in the management of cancers for the detection of bone metastasis. Technetium 99 m-methylene diphosphonate (99mTc-MDP) is commonly used as a bone-seeking agent. The bones take up 99mTc-MDP through a process called chemisorption, which is more evident in areas of increased osteoblastic activities. Nevertheless, extra-osseous 99mTc-MDP uptake is an infrequent occurrence, which warrants a thorough clinical assessment to evaluate such findings. An example of extraosseous uptake discovery is rhabdomyolysis, which requires prompt recognition and immediate management. Rhabdomyolysis secondary to an adverse reaction towards iodinated contrast material is a rare condition that warrants a high index of clinical suspicion.
Case presentation
We present a case of a 75-year-old gentleman with underlying benign prostatic hypertrophy, and chronic kidney disease who had undergone a coronary angiography examination and intervention for ischemic heart disease. Pre-scheduled bone scintigraphy with 99mTc-MDP for the work-up of raised serum prostate-specific antigen (PSA) was performed 2 weeks post coronary angiography examination. Whole-body bone scan with single-photon emission computed tomography/computed tomography (SPECT/CT) images showed an unexpected finding of extensive extra-osseous uptake in the muscles and soft tissues. Additional investigations confirmed the diagnosis of rhabdomyolysis. Nevertheless, despite the prompt recognition, administration of treatment and supportive care, the patient succumbed to life-threatening complications.
Conclusion
This case highlights the importance of recognising and identifying the pattern of extra-osseous uptake on bone scintigraphy imaging to ensure early intervention of severe and life-threatening conditions such as rhabdomyolysis.
Similar content being viewed by others

Background
Bone scintigraphy is an appropriate tool in the management of cancers for the detection of bone metastasis. Technetium 99 m-methylene diphosphonate (99mTc-MDP), Technetium 99 m-hydroxyethylene diphosphonate (99mTc-HDP) and Technetium 99 m-hydroxy methylene diphosphonate (99mTc-HMDP) are common bone-seeking agents. The bones take up these agents by the mechanism of chemisorption, which is aided by increased osteoblastic activity and regional hyperperfusion [1]. Nevertheless, the detection of extra-osseous99mTc-MDP uptake is an infrequent occurrence, which warrants a thorough clinical assessment to evaluate such findings. An example of extra-osseous finding is rhabdomyolysis, which requires prompt recognition and immediate medical management. Rhabdomyolysis secondary to an adverse reaction towards iodinated contrast agents is a rare condition that warrants a high index of clinical suspicion, as demonstrated in this case.
Case presentation
We report a case of a 75-year-old gentleman with underlying benign prostatic hypertrophy (BPH), chronic kidney disease (stage 3B) and ischemic heart disease. For the past 2 years, he had experienced lower urinary tract symptoms, i.e., increased urinary frequency, urgency, incomplete voiding and nocturia. He denied any constitutional symptoms and had no family history of malignancy. The digital rectal examination noted an enlarged prostate gland with a slightly prominent median sulcus suggestive of benign prostatic hyperplasia (BPH). His serum prostate-specific antigen (PSA) was elevated, measuring 115 ng/ml (normal value range, < 4 ng/ml). Recently, he also complained about worsening chest pain and lower back pain. Nevertheless, he was ambulating fairly well and was independent in his activities of daily living (ADL).
He eventually underwent a coronary angiogram in June 2020 for his worsening chest pain, which showed severe three-vessel disease. At that time, he was managed conservatively whereby he was prescribed with anticoagulant therapy, and the dosage of his other medications was optimised. Upon discharge, however, he complained of persistent chest pain thus was re-admitted for urgent percutaneous coronary intervention. Stenting was done in the left main stem, left anterior descending and left circumflex arteries.
Upon discharge, he developed progressive weakness of his lower limbs associated with bilateral thigh pain, which limited his mobility. Consequently, he became wheelchair bound within a month. He sought treatment at the nearest hospital; his symptoms were initially attributed to bilateral knee osteoarthritis based on the X-ray examination of his knees.
Subsequently, because of elevated serum PSA, he was worked up for prostate cancer and referred for bone scintigraphy to assess for possible bone metastasis. 99mTc-MDP bone scintigraphy was performed approximately 1-month post coronary angiography and intervention. He received 18.99 mCi (702.63 mBq) of 99mTc-MDP, and whole-body planar imaging was performed 3 h later (Fig. 1). Upon reviewing the planar imaging, a complementary SPECT/CT was performed which revealed a focus of increased tracer uptake in the mid shaft of the right humerus as well as intense muscular uptake at the bilateral pectoral muscles, muscles around the scapular, tensor fascia lata and quadriceps femoris (Fig. 2). Additionally, there was prominent diffuse soft tissue tracer uptake in the background that could have been contributed by poor renal function. It was concluded that the intense and diffuse muscular uptake was likely due to myositis/generalised rhabdomyolysis. Upon further questioning, he admitted to a previous history of a fall 3 years ago in which he sustained a fracture to his right arm. However, he denied any recent history of strenuous activity or trauma.

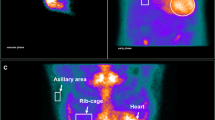
99mTc-MDP planar bone scintigraphy showing diffuse intense uptake at the soft tissue of bilateral shoulder region, upper thoracic and proximal thighs. A focus of increased tracer uptake in the mid shaft of the right humerus is contributed to a healing fracture caused by previous trauma

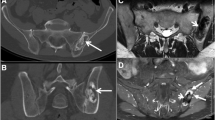
Fused bone SPECT/CT in coronal view. a Image in soft tissue window showing diffuse intense uptake at the bilateral pectoralis muscles, muscles around the scapular, tensor fascia lata and quadriceps femoris (white arrows). b Image in bone window highlights that there is no pathology in the adjacent bones; however, a focus of increased tracer uptake seen in the mid shaft of right humerus corresponds to a sclerotic lesion on CT, likely a healing fracture (red arrow)
The nuclear medicine team alerted the primary team regarding his bone scan findings. Hence, the primary team admitted him for further medical management because of suspected rhabdomyolysis. Clinically, the patient was conscious and orientated to time, place and person. His biochemical markers were elevated, indicating acute on chronic kidney injury (urea, 50 mmol/L; creatinine, 700 mmol/L). His creatinine phosphokinase (CPK) was markedly elevated, measuring 26,000 U/L (normal range, 22-198 U/L). His arterial blood gases revealed metabolic acidosis. His condition was attributed to rhabdomyolysis secondary to contrast-induced nephropathy. Subsequently, he underwent haemodialysis (HD) to treat the uraemia and metabolic acidosis.
The initial HD was performed without any extraction and was uneventful. Post HD, serum creatinine reduced from 700 to 408 mmol/L, and urea reduced from 50 to 33.0 mmol/L. The CPK level also reduced from 26000 to 18562 U/L. The patient was also started on intravenous normal saline infusion and had adequate urine output. A second HD was performed, during which he developed sudden shortness of breath and hypotension. Unfortunately, shortly afterwards, he developed acute coronary syndrome and despite best effort to resuscitate him, he succumbed and passed away.
Discussion
Unexpected extraosseous findings in bone scintigraphy need further attention by the reporting physician as it is pertinent towards the diagnosis of undetected disease pathology. In cases of soft tissue uptake of 99mTc-MDP, the aetiology is often multifactorial and mainly due to the presence of extracellular calcium and phosphate ions which forms calcium phosphate salts [1]. Particular to this patient, the cause of the generalised muscular uptake on bone scintigraphy was due to rhabdomyolysis. Common etiological factors of this condition include trauma, excessive strenuous activity, muscle ischemia, genetic, drugs and toxins [2]. There have been limited publications that have identified generalised muscular uptake on bone scintigraphy that have been attributed to rhabdomyolysis, inflammatory muscle disease, traumatic myositis, polymyositis and dermatomyositis [3, 4].
In this instance, our patient who was initially referred to rule out bone metastasis was incidentally suspected of having rhabdomyolysis based on the bone scintigraphy findings. The bone scintigraphy findings suggestive of rhabdomyolysis prompted immediate hospital admission and institution of treatment, which helped in changing the course of the management of this patient. The diagnosis of rhabdomyolysis was confirmed biochemically, as evidenced by more than 100-fold increase in serum CPK levels. We believed that the patient’s underlying chronic kidney disease and recent contrast media-induced nephrotoxicity were the aggravating factors to induce rhabdomyolysis. The prompt commencement of HD in this patient helped to alleviate the derangement of his renal function. Furthermore, aided by supportive therapies such as intravenous fluid administration and bicarbonates, his renal function improved, and the metabolic acidosis was neutralised. Unfortunately, due to the severity of the condition coupled with his comorbidities, the patient succumbed to his illness.
Renal failure is one of the major complications of rhabdomyolysis. There are several mechanisms in which rhabdomyolysis can lead to renal toxicity, such as the formation of intratubular myoglobin casts, renal vasoconstriction and direct toxicity of myoglobin to renal tubular cells [2]. It can cause severe morbidity and mortality from cardiac arrhythmia, hypovolemia, acute kidney injury, electrolyte imbalances and metabolic acidosis if left untreated [5]. A CPK cut-off value of 5000 U/L has been proposed to indicate the risk of developing AKI or death [6].
Furthermore, iodinated contrast material is a rare cause of non-traumatic rhabdomyolysis, and to the best of our knowledge, it has only been reported in a few publications [6,7,8]. Additionally, the prevalence of acute kidney injury after intravenous contrast media administration in patients with underlying chronic kidney disease was quoted to be 4%, and it is found to be > 10% in patients who had undergone percutaneous transluminal coronary angioplasty (PTCA) intra-arterially [8]. Interestingly, Moriarty et al. reported an unfortunate case of fatal rhabdomyolysis with anuric acute kidney injury secondary to the iodinated contrast material used during endoscopic retrograde cholangiopancreatography (ERCP) in a pancreatic carcinoma patient [7]. Another publication reported a patient who presented with giddiness and generalised muscle weakness of the upper and lower limbs, who was then diagnosed with rhabdomyolysis secondary to a recent iodinated contrast-enhanced computed tomography examination [9].
More interestingly, a case of rhabdomyolysis that presented with symptoms of profound weakness and delayed hypercalcemia was noted to occur after the initiation of high dose simvastatin combined with a history of recent coronary angiography and stenting procedure [10]. It is noteworthy that our patient was given rosuvastatin, instead of simvastatin, which was initiated post-angiography. As simvastatin is lipophilic, it has a higher tendency to interact with muscle tissues and lead to rhabdomyolysis [10]. Whereas rosuvastatin is a hydrophilic agent that dissolves well in water, hence, producing significantly less adverse effects with regards to muscle tissue damage. Furthermore, a review by Mendes et al. also showed that the incidence of rhabdomyolysis was higher amongst patients receiving simvastatin compared to rosuvastatin [11]. Thus, we believe that the initiation of rosuvastatin in this patient was unlikely an attributing factor for the development of rhabdomyolysis.
The uniqueness of our case is the fact that the remarkable findings on the bone scintigraphy alerted us to the patient’s life-threatening condition.
Conclusion
Although rare, iodinated contrast media-induced rhabdomyolysis is a serious complication that ought to be considered when dealing with atypical clinical presentations resulting from contrast media administration. A comprehensive approach in interpreting extraosseous uptake in 99mTc-MDP bone scintigraphy and an inclusive clinical approach with a high clinical index of suspicion can ensure that this life-threatening condition is not missed. Prompt diagnosis and intervention can improve the outcome in an otherwise high mortality related condition.
Availability of data and materials
All the data and materials pertaining to this case report were obtained from patient’s electronic and medical records of our institutions. All data used during this case report are included in this published article.
Abbreviations
- 99mTc:
-
Technetium 99 m
- MDP:
-
Methylene diphosphonate
- HDP:
-
Hydroxy ethylene diphosphonate
- HMDP:
-
Hydroxy methylene diphosphonate
- BPH:
-
Benign prostatic hyperplasia
- PSA:
-
Prostate-specific antigen
- ADL:
-
Activities of daily living
- SPECT/CT:
-
Single-photon emission computed tomography/computed tomography
- CPK:
-
Creatinine phosphokinase
- HD:
-
Haemodialysis
References
Peller P, Ho V, Kransdorf M (1993) Extraosseous Tc-99 m MDP uptake: a pathophysiologic approach. RadioGraphics 13:715–734. https://doi.org/10.1148/radiographics.13.4.8356264
Petejova N, Martinek A (2014) Acute kidney injury due to rhabdomyolysis and renal replacement therapy: a critical review. Crit Care 18(3):224. https://doi.org/10.1186/cc13897
Joshi D, Kumar N, Rai A (2009) Dermatomyositis presenting with rhabdomyolysis and acute renal failure; an uncommon manifestation. Ann Indian Acad Neurol 12(1):45. https://doi.org/10.4103/0972-2327.48853
Steuart R, Morrison R, Lot L (1993) An incidental finding of rhabdomyolysis on bone scintigraphy: case report. J Nucl Med Technol 21:63–64
Sudarsanan S, Omar A, Pattath R, Al Mulla A (2014) Acute kidney injury associated with rhabdomyolysis after coronary artery bypass graft: a case report and review of the literatures. BMC Res Notes 7:152. https://doi.org/10.1186/1756-0500-7-152
Candela N, Silva S, Georges B et al (2020) Short- and long-term renal outcomes following severe rhabdomyolysis: a French multicenter retrospective study of 387 patients. Ann Intensive Care 10(1):27. https://doi.org/10.1186/s13613-020-0645-1
Moriarty N, Moriarty J, Keating J (2020) European journal of case reports in internal medicine contrast-induced rhabdomyolysis occurring after ERCP in a patient with pancreatic cancer: a case report. Eur J Case Rep Intern Med 25(7):583. https://doi.org/10.12890/2020_001704
Ozkok S, Ozkok A (2017) Contrast-induced acute kidney injury: a review of practical points. World J Nephrol 6(3):86. https://doi.org/10.5527/wjn.v6.i3.86
Lee HF (2018) I feel unenergetic! Med emergency. MJEM 3(2):34
Ezad S, Cheema H, Collins N (2018) Statin-induced rhabdomyolysis: a complication of a commonly overlooked drug interaction. Oxford Med Case Rep 2018(3):omx104. https://doi.org/10.1093/omcr/omx104
Mendes P, Robles P, Mathur S (2014) Statin-induced rhabdomyolysis: a comprehensive review of case reports. Physiother Can 66(2):124. https://doi.org/10.3138/ptc.2012-65
Acknowledgements
The authors would like to thank the patient and his family members for providing informed consent to allow the use of his anonymized clinical data and images for the purpose of knowledge sharing and publication. The authors would also like to thank the Director, Institut Kanser Negara and the Director General of Health Malaysia for the permission to publish this manuscript.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
KA, MA, SS and NCS were involved in the interpretation of imaging findings and initial management of the patient. IMA was involved in the subsequent medical management as well as the consent taking from patient and family members. HH was responsible in proofreading of the manuscript writing. All authors contributed significantly to the manuscript writing and all authors read and approved the final manuscript for submission.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained from the patient to participate in this case report. The case report has been reviewed and approved by the local ethical board of the National Medical Research Register of the Institute of Health, Malaysia on 24 October 2020, with the registration ID of 20-2244-56616.
Consent for publication
Patient gave written informed consent to the publication of the manuscript. The images presented do not compromise the patient’s anonymity.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Arumugam, K., Onny, M.A.A., Amran, I.M. et al. Rhabdomyolysis following coronary angiography: an unexpected detection on 99mTc-methyl diphosphonate bone scintigraphy. Egypt J Radiol Nucl Med 52, 22 (2021). https://doi.org/10.1186/s43055-020-00397-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-020-00397-7