
Abstract
Background
To investigate the use of fused positron emission tomography/computed tomography (PET/CT) compared to contrast-enhanced computed tomography (CECT) in the follow-up of treated gastric malignancies, all data were collected and analyzed retrospectively, enrolling 68 patients (18 females and 50 males) (their age range = 34–73 years). The patients had been referred to a private imaging center for their assessment by PET/CT.
Results
Adenocarcinoma was present in 73.5%, lymphoma was present in 23.5%, and malignant carcinoid was found in 3% of cases. All patients had received at least one treatment method including endoscopic/surgical resection, chemotherapy, and radiotherapy.
By PET/CT, gastric recurrence/residual was depicted in 30 patients (47.0%) compared 46 patients (67.5%) as detected by CECT, and this was statistically significant (P value = 0.006), nodal metastasis was present in 18 patients (26.5%) compared to 26 patients (38%) as detected by CECT (P value = 0.143), and distant metastasis was present in 18 patients (26.5%) compared to 24 patients (35%) as depicted by CECT (P value = 0.265).
Conclusion
PET/CT offered a useful diagnostic modality as compared to CECT for follow-up evaluation of cases with treated gastric malignancies through a precise detection of the gastric lesions but it had rather comparable results in the detection of nodal and distant metastases.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Gastric neoplasms are classified according to their cell of origin into epithelial and non-epithelial tumors; each of them could be further subdivided into benign and malignant lesions. Malignant lesions may be primary lesions that arise from the gastric tissues or secondary lesions which arise from other organs and then extend to the stomach [1].
Gastric carcinoma is a malignant epithelial lesion that has a wide distribution and is considered as the fourth most common cancer worldwide and the third common gastrointestinal cancer after colonic and pancreatic cancers. It has also a high mortality rate being second to the bronchogenic carcinoma [2].
Surgical resections of gastric cancers and adjacent lymphadenectomy are considered as the curative treatment of choice for early gastric cancers [2, 3]. However, a wide spectrum of treatment options is currently present, starting from the endoscopic resection of certain mucosal lesions to the extended radical resections in advanced cancers, in addition to chemotherapy and/or radiotherapy which are considered either as adjuvant therapies for surgery and endoscopy or may be the sole treatment options for certain types of malignancies and for surgically unfit patients [2, 3].
Gastric lymphoma is an example of non-epithelial tumors and represents 3% of all gastric malignancies; it can be subdivided histopathologically into a non-Hodgkin’s type which is—by far—considered more common than the Hodgkin’s type [1].
Multi-slice computed tomography (MSCT) with its multiplanar capabilities, optimal contrast enhancement, and the recent advances in its technology regarding thin sections acquisition had greatly helped in early tumor detection and staging; however, CT has some limitations regarding the demonstration of the small metastatic lymph glands and the peritoneal seeding as well as the small blood-borne distant metastasis [3].
Positron emission tomography (PET) with 2-[fluorine-18] fluoro-2-deoxy-d-glucose (FDG) (FDG PET) had been recently introduced as a part of the imaging workup in oncology through scanning a larger volume than the usual CT and demonstrating the metabolically active distant metastasis, the peritoneal metastasis, and the normal-sized but affected lymph glands; moreover, it is also considered a valuable imaging tool in the follow-up of the therapeutic response in the patients who had received chemotherapy [3].
The hybrid imaging technology had emerged with the combined use of the CT and PET (PET/CT) had also added great value in the preoperative tumor staging and in the follow-up of the therapeutic response in the treated patients, nevertheless, in the detection of tumor recurrences and residuals [3, 4].
Aim of work
The aim is to investigate the use of fused positron emission tomography/computed tomography (PET/CT) compared to CECT in the follow-up assessment of the patients with treated gastric malignancy.
Methods
All data were collected and analyzed retrospectively, enrolling 68 patients in the period from November 2017 till December 2018; they were cases of treated gastric malignancies. The patients had been referred to a private imaging center for their assessment by PET/CT and evaluation of their treatment response.
The patients’ ages ranged from 34 to 73 years with a mean age of 58.03 ± 10.37 years. They were 18 females (26.5% of cases) and 50 males (73.5% of cases) (Tables 1 and 2).
Inclusion criteria: The study included all cases of gastric malignancies that had a curative (surgical or endoscopic) resection, chemotherapy, radiotherapy, or any combination of them.
Exclusion criteria: patients who had been pathologically proven to have a benign gastric neoplasm and those who had gastric malignancy but had not received any treatment were also excluded from the study.
The protocol was reviewed and approved by the local ethics committee
Imaging technique
Methods
-
All patients were fasting for 6 h prior to the examination. They were well-hydrated by an oral route. Blood sugar levels were measured and found within the normal levels in all cases before the study. A maximum sugar level that was accepted for [fluorine-18] fluoro-2-deoxy-d-glucose (FDG) injection was 150 mg/dl.
-
0.22 mCi/kg (18F-FDG) were injected and then the patients were rested for three-fourth of an hour in a relaxed position which was considered as an uptake period.
-
High-quality PET/CT system with multi-detector (16 detectors) CT scanner (GE, Discovery IQ, USA) was used in scanning of the patients.
-
First low-dose non-contrast CT images were obtained for attenuation correction and for fusion images.
-
PET scans were extending from the midface to the upper thighs.
-
Serum creatinine level was measured routinely in all patients before contrast administration for the CECT examination.
-
Routine contrast-enhanced helical CT axial images of the brain, neck, chest, abdomen, and pelvis at 2 mm intervals following an intravenous injection of nonionic contrast material was acquired in all patients after they had finished their PET/CT examination.
-
The whole acquisition time for an integrated PET/CT scan was about half an hour.
Data analysis and interpretation
-
Special workstations were used in the reconstruction of PET image data sets using the CT data for attenuation correction and co-registered multiplanar images were displayed using special software.
-
The CT, PET, and fused PET/CT images were interpreted by an experienced radiologist (4 years of experience in PET/CT imaging) through a visual assessment considering the liver as an internal reference and by semi-quantitative evaluation via measuring the standardized uptake value (SUV). Follow-up (clinical and radiological) served as the reference standard for all patients in the study.
-
SUV was calculated automatically by software through a dedicated workstation.
Interpretation of the CE CT findings
-
The detection of gastric soft-tissue masses or mural thickening with or without surrounding tissue infiltration was considered as malignant.
-
The lymph node assessment used a size-based threshold of 1.0 cm (short axis) for malignancy. Furthermore, lymph nodes with a preserved fatty hilum or with calcifications were regarded as benign, whereas central necrosis was considered as malignant.
-
The hypodense hepatic focal lesions either with or without marginal contrast enhancement were considered as malignant lesions.
-
Any non-calcified pulmonary nodule was considered as a malignant while the calcified pulmonary nodules were considered as benign nodules.
Interpretation of the PET/CT findings
-
The gastric mural thickening or masses were considered as positive if their uptake was seen exceeding the background activity
-
The hepatic focal lesions were considered as positive if their uptake was higher than or equal to that of the rest of the hepatic parenchyma and, essentially, was considered as negative lesions if their uptake was lower than that of the rest of the hepatic parenchyma.
-
The lung nodules that were seen having a size of 5 mm were considered as positive if FDG uptake was greater than the mediastinal blood pool; however, a metastatic infiltration could not be excluded in the lung nodules that were < 0.5 cm.
-
If there was a manifest multifocal FDG avidity in the bone marrow, the patients were considered as PET/CT positive; nevertheless, the diffuse uptake pattern in reactive bone marrow hyperplasia following chemotherapy can mimic or mask a diffuse bone marrow involvement; therefore, an appropriate history taking was critical and might be problem-solving in such situations. A delay of 3–4 weeks after completion of therapy could permit the physiologic marrow activity to diminish.
-
The peritoneal nodules or masses were considered positive if their uptake was more than the background activity
Statistical methods
Data management and analysis were performed using the Statistical Package for Social Sciences (SPSS) vs. 23. Numerical data were summarized using means, standard deviations, and ranges, as appropriate. Categorical data were summarized as numbers and percentages. For comparing categorical data, chi-squared (χ2) test was performed. Exact test was used instead when the expected frequency is less than 5 [5] P values less than 0.05 were considered as statistically significant.
Results
Sixty-eight patients were retrospectively enrolled in the current study (50 males and 18 females). Adenocarcinoma was the histopathologic tumor type that was present in 50 patients (73.5%), lymphoma was found in 16 patients (23.5%), and malignant carcinoid was depicted in two patients (3%) (Tables 2 and 3).
All patients had received at least one treatment method or a combination of more than one. The treatment options include endoscopic or surgical resection, chemotherapy, and radiotherapy (Table 4).
Tumor recurrence was categorized as gastric recurrence/residual, nodal metastasis, and distant metastasis (Table 5).
By PET/CT, gastric recurrence/residual was depicted in 30 patients (44.0%) compared to 46 patients (67.5%) as detected by CECT, and this was statistically significant (P value = 0.006). Nodal metastasis was present in 18 patients (26.5%) compared to 26 patients (38%) as detected by CECT (P value = 0.143), and distant metastasis was present in 18 patients (26.5%) compared to 24 patients (35%) as depicted by CECT (P value = 0.265) (Tables 5 and 6); thus, neither nodal nor distant metastasis had a statistical significance as the P value for each of them was > 0.05.
Discussion
Gastric cancer has a worldwide distribution and is considered as the fourth common cancer worldwide especially in Asians. It has a high mortality rate notably in late and advanced cases; thus, an early detection and tumor staging with proper intervention performance can carry a potential curability [2,3,4].
Due to its availability and its relatively low cost, CT had been widely used in the evaluation of recurrences in gastric cancers; however, its role is limited to detect the suspected gastric recurrences and is often unable to differentiate a true tumor recurrence from the morphological changes that may follow the treatment interventions like operative bed scarring [3].
It worth mentioning that CT depends mainly on the size assessment for evaluation of the tumor response to therapy, and from a practical point of view, this is not accurate and is not feasible in many gastric tumors as most of them are not measurable [3].
Positron emission tomography (FDG PET) had been proven as a useful diagnostic tool for the precise detection of tumor respectability and in the detection of distant hematogenous deposits, but unfortunately, it is lacking the anatomical details that made its use limited in the locoregional staging [6].
FDG PET/CT had offered an accurate diagnostic tool in the primary diagnosis of gastrointestinal malignancies and in the recurrent status as compared to the conventional diagnostic tools [2].
In the current study, we were concerned with the detection of recurrences in the gastric neoplasm in the treated cases in addition to the nodal and distant metastases through a comparative correlation between the image findings of both PET/CT and CECT.
Gastric residual/recurrence as detected by PET/CT in our study was found in 30 patients (44%) of all cases, based on the metabolic activity that was seen in the lesions; this was statistically significant (P value = 0.006) as compared to the results of the CECT where the gastric residual/recurrence was found in 46 patients (67.5%) (Tables 5 and 6) (Figs. 1, 2, 3, and 5), hereby, a discordance with Gedik et al. and Sim et al. studies, where they reported a comparable diagnostic value for the PET/CT with the standard CECT in patients with gastric carcinoma and in evaluation of the gastric recurrences [2, 4]; this difference could be explained by the difference in the sample size as our study was enrolling a relatively larger number of patients (68 patients) compared to their studies that were enrolling 20 and 52 patients respectively; however, Sim et al. had warranted further studies to validate the role of PET/CT in gastric cancer recurrences [4].

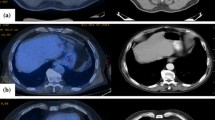
Axial post-contrast CT and fused PET/CT images for a 70-year-old male patient with a history of gastric cancer and had received chemotherapy. Images a and b showed a metabolically active irregular circumferential polypoidal mural thickening involving the gastric body and antrum region (red arrows), measuring 25mm in its maximum thickness with SUVmax ~ 6.3. Images a–d showed multiple metabolically active hypodense metastatic hepatic focal lesions (blue arrows) scattered in both hepatic lobes; the largest is seen in the left hepatic lobe measuring 6.5 cm in its maximum dimension with SUVmax ~ 12.5. Images e and f showed a metabolically active left lower lobe apical segment perihilar region metastatic soft tissue mass lesion (green arrows) measuring 3.2cm with SUVmax ~ 9.8

Axial post-contrast CT and fused PET/CT images for a 68-year-old patient with a history of pathologically proven gastro-esophageal invasive moderately differentiated adenocarcinoma. He received chemotherapy and he was under follow-up. Images a and b showed an irregular circumferential mural thickening involving the gastro-esophageal junction extending to the gastric fundus and proximal body region with no related metabolic activity (yellow arrows). Images c and d showed a right hepatic hypodense focal lesion at segment VI, with no related metabolic activity (red arrows). So PET/ CT had revealed a near complete disease remission despite the presence of the pathological process in CT

Axial post-contrast CT, PET, and fused PET-CT images for a 69-year-old male patient with gastric carcinoma and had received chemotherapy. Images a–c showed FDG avid metabolically active irregular circumferential gastric mural lesions (yellow arrows) reaching 3.2 cm along the gastric fundus and body with SUVmax ~ 19.3, in addition to multiple hypermetabolic gastrohepatic and porta hepatis lymph nodes (red arrows); the largest measures 3.5 cm with SUVmax ~ 8.9. Images d–f showed few FDG avid metabolically active hypodense hepatic dome focal lesions (yellow arrows), the largest and the most active one measures 1.4 cm with SUVmax ~ 6.1
Our study was greatly matching Bilici et al. study who had reported superiority of PET/CT compared to the diagnostic CT for the follow-up of the treated gastric cancers and in the detection of tumor recurrences [7]. A high sensitivity reaching 80% had been described in the literature for detection of the tumor recurrences by PET/CT in gastric cancers as compared to the standard post-contrast CT examinations [2, 8, 9].
Despite having a bad prognosis; tumor recurrences should be carefully evaluated as the early identification of small recurrent masses in the presence of minimal adenopathy could have a better response to chemotherapy or radiotherapy [3].
A good point that could explain why is the PET/CT considered as a superior surveillance diagnostic modality for evaluation of post-therapy gastric malignancies when compared to the CECT is that the former has the ability of detecting the metabolic activity inside the true lesions where the glucose metabolism is elevated but is significantly lower in the postoperative scarring; thus, the use of the PET/CT could be of value in differentiating the two conditions and helping for the clinical decision-making process to be accomplished [3, 7, 10].
Tirumani et al. had reported excellent results for PET/CT in the initial assessment of lymphoma and is considered as a more accurate modality for detection of recurrence/residual lesions than the standard anatomical imaging modalities [11].
Nodal metastasis is another important factor in the prognosis of gastric cancers. PET/CT can detect the metabolic activity of the lymph glands and not only the anatomical details that are given by the conventional CT [2].
In our study, the nodal metastasis was found by PET/CT in 18 patients (26.5%) compared to 26 patients (38%) that were detected by CECT; however, this was statistically insignificant (P value = 0.143) (Tables 5 and 6) (Figs. 3, 5, and 6). This was matching with many studies in the literature and eventually some considered that CECT is more sensitive in detection of metastatic lymph nodes than the PET/CT; however, the role of the PET/CT in the detection of the metabolic activity of normal-sized and mildly enlarged lymph glands has to be considered in this comparison. Moreover, the absence of the metabolic activity in enlarged but tumor-free lymph glands may beneficial in the evaluation of the therapeutic response to chemotherapy and to radiotherapy and sometimes, the detection of metabolically active distant nodal metastasis (like cervical or mediastinal nodes) may preclude unnecessary surgical interventions [2,3,4]; in other words, CECT can give better anatomical details and perfect localization of the nodal metastasis in addition to the pattern of enhancement and the presence of necrosis with high spatial resolution, but the metabolic activity of the malignant nodes could be better assessed by PET/CT, especially the nodes that are not or mildly enlarged. However, the high cost of the PET/CT in comparison to its benefit in the assessment of the nodal metastasis should be carefully weighed when a diagnostic modality is to be chosen.
Distant metastasis including the solid organ hematogenous metastasis and the peritoneal seeding was found in 18 patients (26.5%) by PET/CT in our study compared to 24 patients (35%) that were detected by CECT; this was also considered statistically insignificant (P value = 0.265) (Tables 5 and 6) (Figs. 1, 2, 3, 4, 5, and 6). In agreement with Gore and Miller et al.’s studies, the hepatic metastasis (portal vein born metastasis) [12, 13] was dominating in our study being found in 16 patients (23.5%) form a total of 18 patients with distant metastasis (Figs. 1, 2, and 3).

Axial post-contrast CT, PET, and fused PET/CT images for a 50-year-old male patient with gastric antrum adenocarcinoma and had received chemotherapy. Images a–c showed an ill-defined gastric antrum metabolically active lesion (red arrows) merging with metabolically active omental soft tissue sheet (blue arrows) with SUVmax ~ 13.8. Images d–f showed multiple metabolically active peritoneal nodular lesions (blue arrows) with SUVmax ~ 17.8; moreover, a moderate to marked low grade metabolically active ascites (yellow arrows) was seen

Axial and coronal post-contrast CT, PET, and fused PET/CT images for a 52-year-female patient with gastric neoplasm; she had received chemotherapy. Images a–c showed no metabolically active residual/recurrent gastric lesions (yellow arrows). Images d–f showed no metabolically active nodal or metastatic lesions

Axial and coronal post-contrast CT, PET, and PET/CT images for a 42-year-old female patient diagnosed as distal oesophageal and gastric fundus mural thickening by the upper endoscopy and this was pathologically proven to be lymphoma. Images a–c showed an ill-defined metabolically active lower oesophageal, gastro-oesophageal and gastric fundus mural thickening (yellow arrows) with SUVmax = 5.4. Images d–f showed multiple metabolically active supradiaphragmatic and infradiaphragmatic lymphadenopathy (red arrows), the most active lesion is seen in the mediastinal group with SUVmax = 13.8. Images g–i showed metabolically active bilateral iliac bone lesions with no gross corresponding CT findings (blue arrows); their measured SUVmax = 10.4
Chung et al., Kinkel et al., and Lim et al. had reported a high sensitivity of the PET/CT in the detection of distant metastasis in the solid organs, and this was considered as a major advantage of the PET/CT over other imaging modalities [3, 14, 15]. However, Gedik et al. had found a higher specificity for PET/CT in the detection of the distant metastasis than the CECT in patients with metastatic gastric carcinoma but in concordance with our study, and they reported that the difference could not be considered as statistically significant (P > 0.05, McNemar’s test) [2].
There is a trend in the literature of the low sensitivity of PET/CT in relation to the CECT in the detection of the peritoneal seeding [2,3,4]; however, in our study, the peritoneal seeding was seen in six patients (8.8%) (Fig. 5). Nevertheless, the presence of the peritoneal seeding may be considered as a sign of advanced disease and may imply incurability and often carry a bad prognosis; however, some studies had shown that the peritoneal seeding is usually detected intraoperative and may be overlooked or under detected by the CT [3].
CECT can show ascites in cases of peritoneal metastasis, and this was seen in two of our cases (2.9%) (Fig. 6). Other CECT findings include focal nodular thickening of the peritoneal fat, thickening and enhancing parietal peritoneum, and distorted small bowel walls. In PET/CT, two patterns are recognized, the first one is a diffuse even uptake delineating the visceral surfaces in the abdominal and pelvic cavities and the second one is scattered focal nodules that are randomly distributed in the abdominal and pelvic cavities [3], the latter was identified in our study (Fig. 6).
In our study, two patients had small pulmonary nodules as detected by CECT; however, their sizes were too small to demonstrate FDG uptake by PET/CT (beyond the PET resolution). On the other hand, one of our cases with lymphoma and had a gastric recurrence and mediastinal nodes metastases is detected by both CECT and PET/CT. There was an additional finding—not identified by the CECT—that was added by the PET/CT which was the osseous deposits affecting both iliac blades (Fig. 6), denoting the presence of blood-borne bone metastasis, and consequently, this may imply a different treatment decision.
A lower survival rate had been reported in the patients who had high SUV values (FDG avidity) either in their recurrent primary tumor or in the distant metastatic lesions as compared to those who had lower SUV values. However, the mucinous and the signet ring cell carcinomas (both are reported as aggressive types of tumors) may typically present a low FDG uptake; thus, a low FDG uptake does not necessarily mean a better prognosis [16]. It was also reported that a negative PET scan after a curative surgical treatment with curative intent was significantly associated with a longer survival rate [17].
There were some limitations in our study including the following: the first one was its retrospective nature with a relatively small sample size. The second one was the lacking data about the size of the primary tumor and the histopathological confirmation of the recurrent gastric lesions and nodal and distant metastatic deposits.
Despite these limitations, our study had provided a significant role of PET/CT as postoperative surveillance and in the decision-making regarding the gastric recurrence/residual lesions. However, further prospective studies with a larger sample size are warranted and a gold standard reference like the histopathology examination of the recurrent and the metastatic lesions should be included for the accuracy measures.
Conclusion
PET/CT offered a useful diagnostic modality as compared to CECT for follow-up evaluation of the cases with treated gastric malignancies through a precise detection of the gastric lesions, but it had rather comparable results in the detection of nodal and distant metastases.
Availability of data and materials
All data are available on a software system owned by each of the authors and the corresponding author has the authority to respond if there is any query.
Abbreviations
- CECT:
-
Contrast-enhanced computed tomography
- FDG:
-
Fluoro-2-deoxy-d-glucose
- PET/CT:
-
Positron emission tomography/computed tomography
- SUV:
-
Standardized uptake value
References
Weissleder R, Weissleder R, Weissleder R (2007) Primer of diagnostic imaging, 5th edn. Mosby, St. Louis, p 126
Gedik GK, Yılmaz F, Koplay M, Sari O (2017) Role of 18F-FDG PET/CT in gastric carcinomas: comparison with contrast enhancement computed tomography. Clin Oncol 2:1221
Lim JS, Yun MJ, Kim MJ, Hyung WJ, Park MS, Choi JY et al (2006) CT and PET in stomach cancer: preoperative staging and monitoring of response to therapy. Radiographics 26:143–156
Sim SH, Kim YJ, Oh DY, Lee SH, Kim DW, Kang WJ et al (2009) The role of PET/CT in the detection of gastric cancer recurrence. BMC Cancer 9:73
Chan (2003) Biostatistics 103: Qualitative Data –Tests of Independence. Singap Med J 44(10):498–503
Kole AC, Plukker JT, Nieweg OE, Vaalburg W (1998) Positron emission tomography for staging of oesophageal and gastroesophageal malignancy. Br J Cancer 78:521–527
Bilici A, Ustaalioglu BB, Seker M, Kefeli U, Canpolat N, Tekinsoy B et al (2011) The role of 18F-FDG PET/CT in the assessment of suspected recurrent gastric cancer after initial surgical resection: can the results of FDG PET/CT influence patients’ treatment decision making? Eur J Nucl Med Mol Imaging 38:64–73
Park MJ, Lee WJ, Lim HK, Park KW, Choi JY, Kim BT (2009) Detecting recurrence of gastric cancer: the value of FDG PET/CT. Abdom Imaging 34:441–447
Nakamoto Y, Togashi K, Kaneta T, Fukuda H, Nakajima K, Kitajima K et al (2009) Clinical value of whole-body FDG-PET for recurrent gastric cancer: a multicenter study. Jpn J Clin Oncol 39:297–302
Hopkins S, Yang GY (2009) Positron emission tomography’s utility in esophageal cancer management. J Thorac Dis 1:29–33
Tirumani S, LaCasce A, Jacene H (2015) Role of 2-deoxy-2-[18F]-fluoro-d-glucose-PET/computed tomography in lymphoma. PET Clinics 10(2):207–225
Gore RM (1997) Gastric cancer: clinical and pathologic features. Radiol Clin N Am 35:295–310
Miller FH, Kochman ML, Talamonti MS, Ghahremani GG, Gore RM (1997) Gastric cancer: radiologic staging. Radiol Clin N Am 35:331–349
Chung HW, Lee EJ, Cho YH, Yoon SY, So Y, Kim SY et al (2010) High FDG uptake in PET/CT predicts worse prognosis in patients with metastatic gastric adenocarcinoma. J Cancer Res Clin Oncol 136:1929–1935
Kinkel K, Lu Y, Both M, Warren RS, Thoeni RF (2002) Detection of hepatic metastases from cancers of the gastrointestinal tract by using noninvasive imaging methods (US, CT, MR imaging, PET): a meta-analysis. Radiology 224:748–756
Mochiki E, Kuwano H, Katoh H et al (2004) Evaluation of 18F–2-deoxy-2-fl uoro-D-glucose positron emission tomography for gastric cancer. World J Surg 28(3):247–253
De Potter T, Flamen P, Van CE et al (2002) Whole-body PET with FDG for the diagnosis of recurrent gastric cancer. Eur J Nucl Med Mol Imaging 29(4):525–529
Acknowledgements
Not applicable, as all authors are coauthors for this research.
Funding
All authors had no fund for this research and had no competing interests.
Author information
Authors and Affiliations
Contributions
AAB, the corresponding author, had contributed by data collection and some interpretation of the image studies in the research work and in the editing of the manuscript and reference collection. TAH had introduced the idea of the current study and helped in the image selection and in the final revision of the submitted version. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The protocol was reviewed and approved by the local ethics committee of the radiology department, Kasr Aliny hospital, Cairo University.
The reference number was not applicable in our department at the time of the start of the study.
All patients had given their written consent to participate in this work.
Consent for publication
All patients had given their written consent for publication of this work.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Baz, A.A., Hassan, T.A. Role of fused PET/CT compared to the standard contrast-enhanced CT in the follow-up assessment of the treated gastric malignancy. Egypt J Radiol Nucl Med 50, 95 (2019). https://doi.org/10.1186/s43055-019-0093-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-019-0093-9