
Abstract
Background
Immersive and non-immersive VR technology has been increasingly employed in training. This has encouraged physicians working in skill development to try using it to improve the learning, emotional recognition, and social skills of various disorders. This study aimed to explore the controlled trials employing VR in autism, ADHD, and dyslexia.
Methodology
A literature review has been conducted, on PubMed, Scopus, and Web of Science. Any controlled trial in the pediatric age group, involving the comparison of VR training with other types of therapies in autism, ADHD, and dyslexia was included.
Results
Only 4 controlled trials were identified, comprising a total of 208 patients, with ages ranging from 6 to 16 years. Out of these studies, two involved patients with autism, one with ADHD, and one with dyslexia. VR was successful in improving emotional recognition but not social interaction in autism. All trials did not mention thoroughly possible complications of prolonged use of VR.
Short conclusion
Despite being a promising technology, there is still a long road to prove the validity of using VR in skills development. Few controlled trials have been tailored to explore VR advantages over conventional training and therapies, most of them have a limited sample size, a short training course, and no mention of possible setbacks, such as ocular effects and social isolation.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Several difficulties are faced by atypical children in education as pedagogic settings are developed for typical-developing children. It highlights the importance of experiencing the learning process of children with learning disabilities or cognitive and perceptual impairments, as they may find it challenging to comprehend abstract ideas or representations [1]. Virtual reality (VR) has shown great potential for training life skills in people with intellectual disabilities. By creating immersive and interactive simulations, VR can provide a safe and controlled environment for individuals with intellectual disabilities to learn and practice real-life scenarios in a way that is impossible with traditional training methods. This can improve social, cognitive, motor, and functional skills, ultimately enhancing their quality of life and independence [2, 3].
VR holds several qualities in the development of skills; unlike human tutors, computers are patient, virtual worlds are safe, and can allow learning away from several risks in the real world. However, finally, yet importantly, VR can provide learning regardless of any language and away from the decoding of letters and numbers; the latter can bridge the gap for patients with dyslexia [4].
Despite the many advantages VR has proven, VR does not come without a risk. One of the most important drawbacks currently explored by VR technology is breeding media addiction. This media addiction can slowly result in another problem, which is triggering socially isolating behavior [5].
Our review article aims to explore the fields of learning difficulties, where VR has been tried, and the outcomes of these trials as well as the drawbacks that can result from excessive use of this innovative technology.
Methodology
Scientific libraries
We conducted a computer search for literature listed on PubMed, Google Scholar, Scopus, and Web of Science.
Keywords and inclusion criteria
We employed the following keywords: virtual reality; learning difficulties double arm clinical trials, pediatric age group.
The inclusion criteria were double-arm randomized clinical trials performed on pediatric age groups presenting with one of the following disorders: Autism, ADHD, or dyslexia, to compare the therapeutic effect of VR (immersive and non-immersive) training on their cognitive and social skills to another form of conventional behavioral and skill training.
We excluded all small-scale studies such as case–control and feasibility studies and single-arm or uncontrolled trials involving the same disorders.
-Outcome parameters included: the age range of participants, the scope or area of training, the type of VR used (immersive via head-mounted device or non-immersive), the method to which VR is being benchmarked, and a brief description of results.
Results presentation
-No statistical analysis was conducted, but rather study results were presented in the form of a table summarizing the parameters for each included study.
Results of the included studies
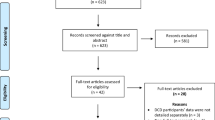
We identified several systematic reviews on ADHD and autism, utilizing results of studies on VR in these respective disorders, notably that of Li and colleagues and Dechsling et al. [6, 7]. They both recognized that studies included in their work, are mostly small-scale case–control or feasibility studies, or to the best single-arm randomized trials. Another review on ADHD showed essentially the same pattern as the included studies. We explored the reports covered by these reviews using our inclusion and exclusion criteria, to determine which of them qualify for our review.
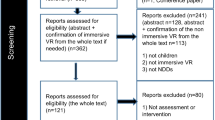
After careful examination, we identified two studies on autism [8, 9], and one on ADHD [10], that fulfill our criteria of selection, to which we added one randomized controlled trial in the context of dyslexia [11]. PRISMA flow chart in Fig. 1 shows the selection process implemented in this study.

PRISMA 2020 flow diagram for our systematic review to show the study selection process. Abbreviations: ADHD: attention deficit hyperactivity disorder, n: number
Regarding autism, Frolli et al. [9] limited the scope of their work to the improvement of emotional recognition, while Ip et al. extended their testing to adaptive skills. Both studies showed that VR might be superior to conventional training in improving emotional recognition, while conventional training was proven better in the context of adaptive skills [8].
In patients with ADHD, Biolac used a computer-based test, to compare the number of omission and commission errors across the study groups. While the occurrence of omission errors has been unchanged between the two groups [10].
In dyslexia, the processing speed index markedly improved in patients under VR training [11].
Table 1 discusses the results of the 4 included trials.
Discussion
During the primary search, to elaborate on this review, we had the initial impression, that VR has been extensively applied and tried in skill development in various disorders; abstracts and conclusions of most of the explored studies tend to showcase the positive effect of this new technology, without acknowledging the fact that of the studies are small-scaled, single-armed, without any control arm. Nevertheless, most of the mentioned reports in systematic reviews do not mention monitoring complications of this technology, as if it comes with pure benefit [6, 7, 12, 13].
In this study, we identified a total of 4 controlled trials on skill development in autism, ADHD, and dyslexia; comprising a total of 208 patients, a sample size that does not match a very large population of interest [8,9,10,11].
Moreover, the age range in the four studies is from 6 to 16 years, which means that VR technology is still not extensively available for early training of patients with learning difficulties. This makes the use of VR unfavorable as it is increasingly recognized that early identification and early childhood intervention can improve cognitive skills and lead to better integration in society and mainstream education [14].
A study that was mainly sight-opening is the controlled trial conducted by Ip and colleagues which did not overlook one of the major setbacks of VR technology. Ip et al. demonstrated, that VR was able to improve emotional recognition in patients with autism, however, it was less efficient than conventional training in developing social and adaptive skills [8].
The use of virtual reality (VR) in educational and therapeutic settings for children with disabilities presents several challenges and potential disadvantages. One disadvantage is its ability to isolate children from other kids and their surroundings. Especially with children with disabilities who might prefer spending time in a closed environment; VR emphasizes that and decreases the opportunities for natural interactions. Hence why it is crucial to find a balance and integrate VR as a supplementary tool rather than a sole means of intervention [15].
We also realize that the controlled studies did not mention thoroughly other drawbacks of VR-prolonged use, such as sensory overstimulation, and myopia in HMD especially if employed in early years of life.
The risk of sensory overstimulation, especially for individuals with auditory processing disorders (APD), due to their intense sensitivity to auditory stimuli, should not be overlooked. Careful consideration and customization of VR experiences are essential to prevent overwhelming sensory input, ensuring a positive and effective learning environment for individuals with APD. Moreover,
A specific drawback that was highlighted in studies was the potential of VR to cause discomfort, anxiety, and fatigue with its prolonged use. Some children expressed unease with VR headsets, and there were fluctuations in pulse rates, suggesting increased anxiety during VR sessions. Additionally, factors such as VR difficulty, potential biases in technologies, and limitations of VR eyewear should be carefully considered. Despite the potential benefits of VR, it may not be suitable for all cases, particularly for children with certain medical conditions. Balancing the integration of VR with real-world experiences and ensuring gradual exposure and supervision are crucial for effective and safe implementation in educational settings [16].
Ocular effects of VR remain unleashed, a study by Turnbull et al. showed that VR use on a short-term basis was not associated with an increased risk of myopia, however, a significant choroidal thickening was noted [17, 18].
High costs can also be a burden, since the expenses associated with VR technology, including both hardware and software, pose a barrier to its widespread adoption and accessibility. Therefore, addressing the cost factor is critical to making VR interventions more accessible [19].
Conclusions
The use of VR in skills development seems to be far from being validated. Few controlled trials were found, with a small sample size, and a short training course. The short duration of training does not allow adequate examination of possible complications, especially the ocular and social isolation effects.
The risk of bias in included studies was performed according to the standard scale and presented in Fig. 2 [20].

Risk of bias assessment of the included studies by their order of distribution in Table 1. Guide and abbreviations: (Study 1: Maresca et al., Study 2: Bioulac et al., Study 3: Frolli et al., Study 4: Ip et al.)
Availability of data and materials
Data will be made available upon request.
Abbreviations
- ADHD:
-
Attention deficit hyperactivity disorder
- ASD:
-
Autistic spectrum disorder
- HMD:
-
Head-mounted device
- VR:
-
Virtual reality
References
Chieffo DPR, Arcangeli V, Moriconi F, Marfoli A, Lino F, Vannuccini S et al (2023) Specific learning disorders (SLD) and behavior impairment: comorbidity or specific profile? Child (Basel, Switzerland) 10(8):1356. Available from: http://www.ncbi.nlm.nih.gov/pubmed/37628355.
Chițu IB, Tecău AS, Constantin CP, Tescașiu B, Brătucu T-O, Brătucu G et al (2023) Exploring the opportunity to use virtual reality for the education of children with disabilities. Children 10(3):436. Available from: https://www.mdpi.com/2227-9067/10/3/436.
Jeffs T (2010) Virtual reality and special needs. Themes Sci Technol Educ 2:253–68. Available from: http://earthlab.uoi.gr/theste/index.php/theste/article/view/34.
Hansen MM (2008) Versatile, immersive, creative and dynamic virtual 3-D healthcare learning environments: a review of the literature. J Med Internet Res 10(3):e26. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18762473.
Sokołowska B (2023) Impact of virtual reality cognitive and motor exercises on brain health. Int J Environ Res Public Health 20(5):4150. Available from: https://www.mdpi.com/1660-4601/20/5/4150.
Li C, Belter M, Liu J, Lukosch H (2023) Immersive virtual reality enabled interventions for autism spectrum disorder: a systematic review and meta-analysis. Electron 12(11):2497
Dechsling A, Orm S, Kalandadze T, Sütterlin S, Øien RA, Shic F et al (2022) Virtual and augmented reality in social skills interventions for individuals with autism spectrum disorder: a scoping review. J Autism Dev Disord. 52(11):4692–707. https://doi.org/10.1007/s10803-021-05338-5
Ip HHS, Wong SWL, Chan DFY, Byrne J, Li C, Yuan VSN et al (2018) Enhance emotional and social adaptation skills for children with autism spectrum disorder: a virtual reality enabled approach. Comput Educ 117:1–15. https://doi.org/10.1016/j.compedu.2017.09.010
Frolli A, Savarese G, Di Carmine F, Bosco A, Saviano E, Rega A et al (2022) Children on the autism spectrum and the use of virtual reality for supporting social skills. Children 9(2):181. Available from: https://www.mdpi.com/2227-9067/9/2/181.
Bioulac S, Micoulaud-Franchi J-A, Maire J, Bouvard MP, Rizzo AA, Sagaspe P et al (2020) Virtual remediation versus methylphenidate to improve distractibility in children with ADHD: a controlled randomized clinical trial study. J Atten Disord 24(2):326–35. Available from: http://journals.sagepub.com/doi/10.1177/1087054718759751.
Maresca G, Leonardi S, De Cola MC, Giliberto S, Di Cara M, Corallo F et al (2022) Use of virtual reality in children with dyslexia. Children 9(11):1621
Corrigan N, Păsărelu CR, Voinescu A (2023) Immersive virtual reality for improving cognitive deficits in children with ADHD: a systematic review and meta-analysis. Virtual Real 27(4):3545–64. https://doi.org/10.1007/s10055-023-00768-1
Di Giusto V, Purpura G, Zorzi CF, Blonda R, Brazzoli E, Meriggi P et al (2023) Virtual reality rehabilitation program on executive functions of children with specific learning disorders: a pilot study. Front Psychol 14:1241860. Available from: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1241860/full.
Smythe T, Zuurmond M, Tann CJ, Gladstone M, Kuper H (2021) Early intervention for children with developmental disabilities in low and middle-income countries – the case for action. Int Health 13(3):222–31. Available from: https://academic.oup.com/inthealth/article/13/3/222/5891235.
Merkx C, Nawijn J (2021) Virtual reality tourism experiences: addiction and isolation. Tour Manag 87:104394. https://doi.org/10.1016/j.tourman.2021.104394
Naef AC, Jeitziner MM, Knobel SEJ, Exl MT, Müri RM, Jakob SM et al (2022) Investigating the role of auditory and visual sensory inputs for inducing relaxation during virtual reality stimulation. Sci Rep 12(1):1–11. https://doi.org/10.1038/s41598-022-21575-9
Turnbull PRK, Phillips JR (2017) Ocular effects of virtual reality headset wear in young adults. Sci Rep 7(1):1–9. https://doi.org/10.1038/s41598-017-16320-6
Yoon HJ, Moon HS, Sung MS, Park SW, Heo H (2021) Effects of prolonged use of virtual reality smartphone-based head-mounted display on visual parameters: a randomised controlled trial. Sci Rep 11(1):1–9. https://doi.org/10.1038/s41598-021-94680-w
Farra SL, Gneuhs M, Hodgson E, Kawosa B, Miller ET, Simon A et al (2019) Comparative cost of virtual reality training and live exercises for training hospital workers for evacuation. Comput Inform Nurs 37(9):446–54. Available from: http://www.ncbi.nlm.nih.gov/pubmed/31166203.
Viswanathan M, Patnode CD, Berkman ND, Bass EB, Chang S, Hartling L et al (2018) Recommendations for assessing the risk of bias in systematic reviews of health-care interventions. J Clin Epidemiol 97:26–34. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0895435617310661.
Acknowledgements
Everyone deserves to feel included, included without a particular way, that would rather makes him/her feel excluded, included without a daily reminder that he is different and that he needs an effort to be included, this is how the authors see what is called "inclusive education", thank you to anyone who is trying to do so casually, and easily, without adding any burden, nor hurt to the souls and minds of others; because others can simply or are simply all of us.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
AA and SAS contributed to the conception of the idea. AA, WAH, HAH, SAH, FAH, and SAS contributed equally to the drafting and revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
AbdelMassih, A.F., AlHammadi, W.I., AlHosani, H.A. et al. Revisiting VR training in developmental disorders, is it a friend or foe? A scoping systematic review of randomized controlled trials. Egypt Pediatric Association Gaz 72, 41 (2024). https://doi.org/10.1186/s43054-024-00281-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43054-024-00281-3