
Abstract
Pediatric colorectal cancer, comprising just 1% of childhood cancers, has surged among young individuals, underscoring its significant health impact. Diagnostic challenges arise from atypical presentation and nonspecific symptoms in 90% of cases, leading to delayed detection in 19%.
Methods A 2-year retrospective study of pediatric colorectal carcinoma cases was conducted across a specialized surgical pediatric center. Data were gathered, including age, symptoms, diagnostics, treatments, and outcomes.
Results Six colorectal carcinoma cases (median age, 16) were documented, mainly in males (66%). Predominant histological types included mucinous adenocarcinoma and signet ring cell carcinoma. Metastasis was present in all cases, with symptoms including hematochezia (83%), abdominal pain (100%), weight loss (66%), and anemia (100%). Diagnosis often faced misidentification, fostering disease progression and metastasis. Various diagnostic and treatment modalities were employed, including surgery and neo-adjuvant or adjuvant chemotherapy.
Conclusion Swift detection and intervention for pediatric colorectal carcinoma are pivotal. Efficient diagnostics and heightened awareness among medical professionals and the public are imperative. Early surgical intervention remains a cornerstone, especially for patients with pertinent family histories and characteristic symptoms. Tailored guidelines for pediatric patients are needed to enhance outcomes and survival.
Highlights
• CC is rare but increasing among young individuals.
• CC is often diagnosed late or misdiagnosed due to atypical presentation and nonspecific symptoms.
• Early detection and treatment of CC are crucial for patient survival.
• CC treatment involves surgery, chemotherapy, and targeted therapies.
• Awareness of CC symptoms and risk factors is vital for early detection and management.
Similar content being viewed by others
Background
Colorectal cancer in children (CC) is a rare disease, but there has been an increase in its incidence among young ages in recent years. While it represents only 1% of all childhood cancers, it is essential to consider this disease due to its significant impact on children’s health [1].
The diagnosis of CC is often delayed or confused due to its atypical presentation and nonspecific symptoms in up to 90% of cases. This complicates timely detection and consequently results in advanced-stage disease diagnosis. Only about 19% of cases have localized disease at diagnosis. It is crucial to note the low level of suspicion among clinicians for this age group [2].
Most cases of CC occur sporadically without any identifiable hereditary cause. However, in 10–30% of cases, there are predisposing factors such as genetic syndromes like familial adenomatous polyposis (FAP), Peutz-Jeghers syndrome (PJS), juvenile polyposis syndrome (JPS), Lynch syndrome, and inflammatory bowel diseases. These syndromes may be associated with chromosomal instability or genetic alterations [3].
The most common types of pediatric adenocarcinoma are mucinous adenocarcinoma and signet ring cell carcinoma, which tend to be more aggressive [4], further complicating surgical management and impacting prognosis [5].
This study aims to share our experience in CC, which may aid in generating research questions for future investigation or developing specific guidelines.
Methods
This is a retrospective, observational study analyzing cases of CC at a pediatric oncology surgical reference center in Mexico over 2 years.
Data from each selected case was collected to conduct this study. Relevant information for each case, including age, symptoms, diagnostic tests, treatments received, and clinical outcomes, was recorded.
The collected data was analyzed to identify patterns, standard features, and potential areas for improvement in the early management of pediatric colorectal carcinoma patients. All patients had a late presentation, and all of them had metastatic disease (Table 1).
Results
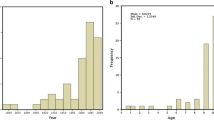
Six cases of CC are included, patients with a median age of 16 years (from 14 to 17 years). The disease was predominant in male patients, representing 66% of the cases. The most frequently encountered histological type was mucinous adenocarcinoma, with signet ring cells in 83.3% (Fig. 1), with the remaining cases being well-differentiated adenocarcinoma. The primary site of involvement predominantly affected the descending colon and rectosigmoid junction in 50% of cases, followed by the ascending colon and vermiform appendix in 16.6% each. All patients presented with metastasis at diagnosis. Regional involvement was observed in all patients, including lymph nodes, peritoneal, diaphragm, and transverse colon carcinomatosis. Three patients had liver metastasis, one had bone metastasis, and another had bone marrow metastasis. One patient had metastasis in their small intestine (duodenum and jejunum), while another patient had metastasis on their spleen and pancreas. All were CC metastasis (Table 1) (Fig. 2).

Histology findings. A A hematoxylin–eosin-stained photomicrograph showing a moderately to poorly differentiated malignant neoplastic lesion of epithelial origin. Cells are arranged in glandular formations and appear as poorly differentiated solitary cells in a solid pattern. B High-power dry magnification reveals loss of cohesiveness in non-glandular neoplastic cells. These cells exhibit enlarged eosinophilic cytoplasm, some containing a single intracytoplasmic vacuole displacing nuclei to the periphery, resulting in hyperchromatic oval and round nuclei with prominent nucleoli resembling a “signet ring” appearance. C The invasion pattern involves infiltrating neoplastic cells into mature adipose tissue with mucin production. This corresponds to a moderately poorly differentiated adenocarcinoma, with some cells displaying a signet ring pattern and reduced cell cohesion within infiltrated tissue

Endoscopy and surgical tumor findings. A Finding on colonoscopy: inflamed and friable sessile polyp. B The same colonoscopy with other less inflamed and friable sessile polyp. C Inflamed, friable colon mucosa with tumor metastasis. D Surgical finding: tumor in the right colon at the ileocecal valve completely obstructing the Intestinal lumen. E Surgical finding: tumoral metastasis to the third duodenal segment and pancreas already resected. F Laparoscopic finding: tumoral implant at the jejunal level
Patients experienced a gradual onset of symptoms, and it took a median of 29.5 days with a median of 24.5 and a mode of 15 days from the first symptom to their initial hospitalization. Patients were admitted with abdominal pain and marked anemia. Hematochezia was present in 83.3%, and 66.6% reported asthenia, discomfort, fatigue, and weight loss. Palpable abdominal tumors were found in 50% of the patients. Three patients were admitted for the first time with acute abdominal symptoms that were surgically explored on an emergency basis. Fifty percent of the patients were managed with surgery for acute pain, while the rest were approached due to a history of abdominal pain and paresthesia in one case. During their hospital course, 50% progressed to third-space leakage with pleural effusions or ascites. Thiry-four percent of patients had a history of gastrointestinal vomiting, and less frequently, more nonspecific symptoms such as oral intolerance, distant adenopathy, and diarrhea were observed. After a fall, a patient experienced progressive paresthesia in their lower extremities; it was found that the symptoms were due to metastasis of the lumbar vertebrae (Tables 2 and 3).
All patients underwent computed tomography to evaluate disease extent, with 50% having a prior abdominal ultrasound and only one patient undergoing magnetic resonance imaging due to symptoms. Four patients underwent endoscopic studies for lesion evaluation and biopsy when they had no abdominal emergency, and an adequate approach was made (Fig. 3). Two patients underwent positron emission computed tomography (PET CT), where primary lesions were visualized. The PET CT was used to identify the primary site of the disease. The use of the radiology modalities was based on the presentation of symptoms, the emergency of each subject, and the evolution.

Imaging findings in pediatric colorectal carcinoma patients. A Abdominal ultrasound of the left colon, demonstrating intestinal wall thickening and luminal occlusion with an isodense lesion with hypodense centers. B Contrast-enhanced chest and abdominal computed tomography showed significant bilateral pleural effusion. C Chest and abdominal computed tomography display thickening of the left colon wall with mural infiltration, accompanied by dilatation of the proximal intestine extending to the stomach. D Abdominal magnetic resonance imaging reveals hypointense lesions with hyperintense capsules in the liver. E Bone scintigraphy shows increased uptake at the site of skeletal metastasis in the lumbar vertebra
Based on the initial presentation of acute abdominal pain, we can differentiate between early and late surgical intervention. When early was a surgical emergency procedure based on the acute abdominal presentation, and late when an adequate approach of the patient could be made.
Two patients underwent laparoscopic procedures for diagnosis, while three were approached by exploratory laparotomy depending on the availability of laparoscopy equipment and the surgeon’s experience. Fifty percent of the patients required surgery: ileostomy, colostomy, hemicolectomy, or appendectomy. Only one patient underwent percutaneous biopsy with a coaxial system. Neoadjuvant and adjuvant chemotherapy was offered to all patients, and only 2 underwent immunomodulatory therapy (Table 1).
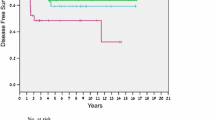
It was discovered that two patients had a significant family history of hereditary conditions (Fig. 4). Five patients had passed away, and only one was still receiving palliative care due to the rapid progression of the disease. On a median, patients lived for 10.5 months after diagnosis, with a median of 13 months and a mode of 15 months until death.

Pedigree of the two patients with a positive family history of cancer
Discussion
Pediatric colorectal carcinoma, due to its distinct characteristics, constitutes a group of rare tumors that have been on the rise within the population. The most common histological types include mucinous adenocarcinoma with signet ring cells and well-differentiated adenocarcinoma, which are more aggressive than unspecified adenocarcinoma. The most common histological type includes mucinous adenocarcinoma with signet ring cells, which are more aggressive than unspecified adenocarcinoma, and well-differentiated adenocarcinoma.
Emphasizing the collaboration between specialized centers for adult and pediatric colorectal carcinoma is crucial, given the absence of specific guidelines for managing this disease in children. Establishing an early and appropriate approach for pediatric patients is imperative, leveraging guidelines and expertise from both areas [6].
Regarding hereditary backgrounds, genetic counseling is recommended for patients with familial cancer syndromes or relevant hereditary histories. This could facilitate timely detection, classification, molecular typing, and identification of potential responders to targeted treatments such as immunomodulators or neoadjuvant radiotherapy [7, 8]. The study highlighted the importance of genetic backgrounds in identifying early intervention for two patients.
Symptomatic patients presented with chronic abdominal pain, weight loss, iron-deficiency anemia, and hematochezia, consistent with existing literature. Acute abdominal presentation occurs in over 20% of cases [9], as observed in one study patient. Preventing misdiagnosis is crucial since approximately 90% of pediatric colorectal carcinoma cases initially receive an inaccurate diagnosis, leading to disease progression and metastasis in 81% of cases [10, 11].
There are several methods to detect colon cancer in its early stages. These include abdominal ultrasound, endoscopy, and colonoscopy. Computed tomography, Tc99 bone gammagraphy, and PET CT determine the cancer stage. Additionally, tumor markers such as carcinoembryonic antigen and carbohydrate antigen 19–9 can help in monitoring and detecting recurrence [12, 13].
Immunomodulatory therapy has shown promise in treating pediatric colorectal carcinoma, especially in cases with hereditary syndromes or DNA microarray instability [14]. The seventh edition of the AJCC staging system (2017), which uses TNM and Duke’s prognostic stages, is used to stage pediatric colorectal carcinoma [15]. The classification shows that 18.4% of cases are stage B, 55.3% are stage C, and 26.3% are stage D. It is essential to note that pediatric patients never reach the more favorable stage A [16]. Patients with stage II to IV diseases involving regional nodes or metastasis benefit from neoadjuvant chemotherapy [17,18,19]. Radiation therapy is typically given after surgery. These findings highlight the significance of staging and prognostic factors in determining appropriate treatment for CC. Adverse effects of chemotherapy enhance outcomes for stage II and advanced stages [6, 20, 21]
Conclusion
Early detection and treatment are crucial for improving the survival and long-term outcomes of CC. Efficient diagnostic algorithms can facilitate patient management and ensure early diagnosis. Surgery is the primary treatment for CC, and early intervention significantly influences patient prognosis. Raising awareness among pediatricians, pediatric surgeons, and the public about CC, its symptoms, and risk factors is fundamental to encouraging early detection and proper management.
Availability of data and materials
The data and materials used in this study are available upon request. Due to restrictions on sharing the data publicly, a direct link to the dataset cannot be provided. However, all relevant data and materials necessary to replicate the study’s findings will be made available to the corresponding author upon reasonable request. Please get in touch with Sofia Brenes Guzmán at sofcxped@gmail.com for further inquiries regarding data and material access.
Abbreviations
- CC:
-
Colorectal cancer in children
- FAP:
-
Familial adenomatous polyposis
- PJS:
-
Peutz-Jeghers syndrome
- JPS:
-
Juvenile polyposis syndrome
References
Sung H, Ferlay J, Siegel RL et al (2021) Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71(3):209–249. https://doi.org/10.3322/caac.21660
Cao X, Luo J, Zhao B, Fu H, Kang W (2022) Pathological complete response after neoadjuvant immunotherapy combined with neoadjuvant chemotherapy in pediatric rectal carcinoma: a case report. Front Immunol 13:1036181. https://doi.org/10.3389/fimmu.2022.1036181. Published 2022 Dec 5
Mathey MD, Pennella CL, Zubizarreta P (2021) Colorectal carcinoma in children and adolescents. Carcinoma colorrectal en niños y adolescentes. Arch Argent Pediatr 119(5):e487–e498. https://doi.org/10.5546/aap.2021.eng.e487
Koh KJ, Lin LH, Huang SH, Wong JU (2015) CARE–pediatric colon adenocarcinoma: a case report and literature review comparing differences in clinical features between children and adult patients. Medicine (Baltimore) 94(6):e503. https://doi.org/10.1097/MD.0000000000000503
Indini A, Bisogno G, Cecchetto G, et al (2017) Gastrointestinal tract carcinoma in pediatric and adolescent age: the Italian TREP project experience. Pediatr Blood Cancer 64(12). https://doi.org/10.1002/pbc.26658
Sultan I, Rodriguez-Galindo C, El-Taani H et al (2010) Distinct features of colorectal cancer in children and adolescents: a population-based study of 159 cases. Cancer 116(3):758–765. https://doi.org/10.1002/cncr.24777
Coutzac C, Bibeau F, Ben Abdelghani M et al (2022) Immunotherapy in MSI/dMMR tumors in the perioperative setting: the IMHOTEP trial. Dig Liver Dis 54(10):1335–1341. https://doi.org/10.1016/j.dld.2022.07.008
Riley RS, June CH, Langer R, Mitchell MJ (2019) Delivery technologies for cancer immunotherapy. Nat Rev Drug Discov 18(3):175–196. https://doi.org/10.1038/s41573-018-0006-z
Cortez-Pinto J, Claro I, Francisco I et al (2020) Pediatric colorectal cancer: a heterogenous entity. J Pediatr Hematol Oncol 42(2):131–135. https://doi.org/10.1097/MPH.0000000000001526
Al-Tonbary Y, Darwish A, El-Hussein A, Fouda A (2013) Adenocarcinoma of the colon in children: case series and mini-review of the literature. Hematol Oncol Stem Cell Ther 6(1):29–33. https://doi.org/10.1016/j.hemonc.2013.02.003
Boardman LA, Vilar E, You YN, Samadder J (2020) AGA clinical practice update on young adult-onset colorectal cancer diagnosis and management: expert review. Clin Gastroenterol Hepatol 18(11):2415–2424. https://doi.org/10.1016/j.cgh.2020.05.058
Vogel JD, Eskicioglu C, Weiser MR, Feingold DL, Steele SR (2017) The American society of colon and rectal surgeons clinical practice guidelines for the treatment of colon cancer. This Colon Rectum 60(10):999–1017. https://doi.org/10.1097/DCR.0000000000000926
Goldberg J, Furman WL (2012) Management of colorectal carcinoma in children and young adults. J Pediatr Hematol Oncol 34(Suppl 2):S76–S79. https://doi.org/10.1097/MPH.0b013e31824e38c1
Kaplan MA, Ozaydin S, Yerlikaya H et al (2019) Clinicopathologic and prognostic differences between three different age groups (child/adolescent, young adults, and adults) of colorectal cancer patients: a multicenter study. Oncol Res Treat 42(10):516–522. https://doi.org/10.1159/000502120
Jessup JM, Goldberg RM, Asare EA et al (2017) Colon and rectum. In: Amin MB, Edge SB, Greene FL, Byrd F et al (eds) AJCC cancer staging manual, 8th edn. Springer, New York, pp 251–274
Benson AB 3rd, Venook AP, Cederquist L et al (2017) Colon cancer, version 1.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Net 15(3):370–398. https://doi.org/10.6004/jnccn.2017.0036
Topalian SL, Taube JM, Pardoll DM (2020) Neoadjuvant checkpoint blockade for cancer immunotherapy. Science 367(6477):eaax0182. https://doi.org/10.1126/science.aax0182
The Lancet Oncology (2017) Colorectal cancer: a disease of the young? The Lancet Oncology 18(4):413. https://doi.org/10.1016/S1470-2045(17)30202-4
Oliveira AF, Bretes L, Furtado I (2019) Review of PD-1/PD-L1 inhibitors in metastatic dMMR/MSI-H colorectal cancer. Front Oncol 9:396. https://doi.org/10.3389/fonc.2019.00396. Published 2019 May 14
Park L, O’Connell K, Herzog K et al (2022) Clinical features of young-onset colorectal cancer patients from a large cohort at a single cancer center. Int J Colorectal Dis 37(12):2511–2516. https://doi.org/10.1007/s00384-022-04286-5
Kunawudhi A, Sereeborwornthanasak K, Promteangtrong C, Siripongpreeda B, Vanprom S, Chotipanich C (2016) Value of FDG PET/contrast-enhanced CT in initial staging of colorectal cancer - comparison with contrast-enhanced CT. Asian Pac J Cancer Prev 17(8):4071–4075
Acknowledgements
Dra. Alicia Georgina Siordia Reyes. Department of Pediatric Pathology. Pediatric Hospital of National Medical Center Siglo XXI, Mexican Social Security Institute. For sharing histopathology pictures.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
JLGC, EMC, and DHM were responsible for data collection, management, sequence alignment, and initial manuscript drafting. EFOG, EGLR, AGBT, and SBG contributed to the clinical aspects of the study and provided patient treatment. EFOG, EGLR, and AGBT participated in patient treatment and sequence alignment, and SBG, JLGC, and JCNE drafted the manuscript. SBG, JLGC, and JCNE contributed to the study design, performed statistical analysis, and provided critical input. SB contributed to the study design, coordination, and manuscript drafting. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This article presents a series of cases involving pediatric patients with colorectal adenocarcinoma and its management. The study complied with the ethical principles outlined in the Declaration of Helsinki. Written informed consent was obtained from the patient’s parents or legal guardians to publish their cases and accompanying images. According to their guidelines, the Hospital Inner Committee (17 CI 09 015 042) approved the study for ethical approval. The confidentiality of patient information was strictly maintained, and all data were de-identified before analysis. This study adheres to our institution’s ethical standards and ensures patients’ privacy and rights.
Consent for publication
Written informed consent was obtained from the patient’s parents or legal guardians to publish their cases and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Guzmán, S.B., García, E.F.O., Rojas, E.G.L. et al. Insights from a retrospective study: an understanding of pediatric colorectal carcinoma. Egypt Pediatric Association Gaz 72, 4 (2024). https://doi.org/10.1186/s43054-024-00246-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43054-024-00246-6