
Abstract
Background
Mother experiences variety of stressors related to premature birth, baby’s medical condition, unpleasant neonatal intensive care unit (NICU) environment and intuit liability of the infant. Identifying factors that causes stress may be useful in assisting health personnel in understanding their importance and in improving the quality of care. Objective of the study is to assess the stress levels of mothers whose neonate is admitted to the NICU as measured by Parental Stress Scale: Neonatal Intensive Care Unit (PSS: NICU).
Methods
This prospective analytical study was conducted in NICU of a tertiary care hospital over a period of 12 months after obtaining permission from the institutional ethics committee. The self-administered questionnaire comprising questions on: sights and sounds experienced in NICU, baby’s looks and behaviour, parental role and relationship with her baby were collected. The mean score and standard deviation were calculated for each component of PSS: NICU Scale and mean scores are compared.
Results
Mothers having full term babies have experienced more stress than those having pre-term babies. As measured by PSS-NICU scale the highest mean scores of 2.3 ± 0.57, 4.36 ± 0.53, 4.43 ± 0.58 were obtained for questions “The other sick babies in the room” component of Sight and Sound, “Seeing my baby looking sick” Component of Looks and Behaviour, “Being separated from my baby” Component of Parental Role and Relationship respectively.
Conclusion
Present study summarises the overall impact of NICU environmental stressors affecting mothers in a developing country and also emphasises the need for further studies in this area for identification of factors that contribute to maternal stress. It may enable health professionals to facilitate mothers’ adaptation, thereby promoting optimal mother–infant relationships and subsequent infant development.
Similar content being viewed by others

Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Everyone in the modern world experiences stress at least occasionally in life. Stress has devastating effects on individual, interpersonal and societal levels; therefore, it is important to understand its nature to assist development of interventions to mitigate these effects. One potentially stressful life event, which is the focus of this study, is the birth of an infant who is then cared for in a neonatal intensive care unit (NICU) [1]. The hospitalisation of a neonate in NICU is usually stressful for the mother and other family members [1]. One way to conceptualise parental stress from the NICU is in terms of factors contributing to this response [2, 3]. The Parental NICU Stress model identifies multiple factors in this response, which includes personal characteristics (age, level of education), situational factors (mode of delivery, preterm/term delivery, gravida), personal resources (occupation, socioeconomic status), environmental support (NICU environment, health care worker, use of instruments and length of stay) and stress response [4]. It is also the only model designed specifically for parents of NICU infants which was adapted from the Parental Intensive Care Unit Stress model. Parental stress especially maternal stress may have effect on neuro-cognitive development, emotional regulation and health of an infant. Mothers may experience depression, fatigue, altered parental behaviour and perception, maladapted mother-infant interaction and parental competency. A systematic examination of the sources of stress in the NICU environment will be useful in leading to solutions [5].
This study was conducted to determine levels of stress in mothers of babies admitted in NICU using Parental Stress Scale: Neonatal Intensive Care Unit (PSS: NICU) scale and to identify infant and maternal characteristics which significantly influence their stress level [4]. Environmental factors that can influence mother’s reaction to having an infant in NICU might include (a) difficulty in fulfilling her maternal role, (b) medical equipment used for intervention and (c) communication patterns and behaviour of the staff [4, 6].
This study was conducted in one of the developing countries, where only few studies are conducted on stressors that affect short term and long term outcome of patients admitted to intensive care unit. Increased information about how mothers of hospitalized high-risk infants perceive NICU, also an understanding of the needs of such mothers may enable NICU staff to identify parents at risk and plan interventions for improving mental health in NICU mothers [7, 8].
Methods
Patient and public involvement: not involved.
This was a prospective analytical study conducted in NICU of a tertiary care hospital over a period of 12 months from February 2019 to January 2020 after obtaining permission from the institutional ethics committee. It is a 10-bedded high dependency unit NICU with annual admission rate of 150 to 200 patients. Inclusion criteria: mothers whose neonate had completed 24 h after the admission in the NICU (in higher dependency unit) with willingness to participate. Exclusion criteria: mothers who were known to be diagnosed with temporary or long-standing psychiatric illness, who cannot come to the NICU and those with NICU stay of less than 24 h. Candidates whose baby died after taking consent were withdrawn from the study. Non-probability sampling method was used for selecting samples. To measure the mother’s perception of stress, PSS: NICU Questionnaire was used, which is a self-report instrument consisting of 27 items [9]. It has 3 subscales which measures stress related to (A) Sight and Sound in the unit (6 items), (B) Appearance and Behaviour of the Infant (11 items), (C) Parental Role and Relationship with their baby (10 items). The questionnaire was translated into Hindi and Marathi by non-medical language expert. The responses to the PSS: NICU were scored on a 5-point Likert scale on which the mothers could rate the level of stress for each item from 1 (not at all stressful) to 5 (extremely stressful) [10, 11]. There was also a not applicable (N/A) option, which was scored 0 when using one of the scale’s scoring methods. Data were collected from mothers whose babies were admitted to NICU under high dependency unit, on a predesigned questionnaire (PSS: NICU) in the morning hours in the NICU counselling room. Qualitative data was represented in form of frequency and percentage. Among qualitative data, nominal data included mother’s details, i.e. age (less than 25 years/25 years or more), gravida (primigravidae/multigravida), education (illiterate/primary/high school/graduate), occupation (unemployed/unskilled/semi-skilled/semi-professional/clerk), type of delivery (vaginal/caesarean), baby’s details, i.e., gestational age (preterm/term), length of stay (< 7 days/>= 7 days), various ‘sights and sounds’ in NICU (e.g. monitors and equipment and their constant noises, other sick babies in the room), the ‘looks and behaviour’ of the baby (e.g. tubes and equipment near the baby, seeing the needle put in the baby, baby being fed by the tube/iv line, seeing the baby in pain), ‘parental role and relation’ (e.g. being separated from the baby, not able to feed/hold the baby, feeling staff is closer to baby). Demographic data and perceived stress of the mothers was evaluated statistically using descriptive statistics. To obtain mean scores that could be compared among the scales, an individual’s total score for each subscale and the total scale was divided by the number of items experienced in the particular scale by that individual. Individual’s scores were then added together according to each subscale and the total scale, and these totals were divided by the number of individuals who had experienced at least one item on the particular scale. The possible range of these mean scores was 1–5. The overall stress levels for each of the three subscales were used to compare with the socio-demographic and clinical characteristics of the mothers and infants.
The data was processed and analysed using the IBM Statistical Packages for Social Sciences, SPSS software version 22. Results of continuous data were measured as frequency mean and standard deviation. Results of categorical data were presented as number (%). Kruskal–Wallis test and Mann Whitney U test was used to compare the different types of data. P value less than 0.05 was considered as statistically significant.
Results
Study included 120 mothers whose babies were admitted in NICU fulfilling inclusion criteria. In the study 88 (73.3%) participants had babies with low birth weight while 32 (26.6%) had birth weight of > 2500 g. Mean birth weight was 2022 g ranging from 535 g to 3510 g. Mean age of mothers participating in the study was 26.5 years with a range between 17 and 42 years of which 40 (33.3%) mothers were primigravidae and 80 (66.6%) were multigravida. No statistically significant difference was observed in mean stress scores for maternal age, gravida, educational status, mode of delivery and the length of the stay the baby indicating that stress levels were independent of these factors (Tables 1 and 2).
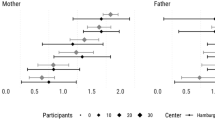
As depicted in Table 3, the domain of Sight and Sound demonstrates a statistically significant (p value = 0.03) difference between different subgroups signifying that in this particular domain mother’s stress level depended on the occupation with mothers having semi-professional and clerical jobs experiencing greatest level of stress. Table 4 illustrate that mothers’ greatest subscale score occurred on the Parental Role and Relationship subscale in both the subgroups followed by looks and behaviour subscale and least score for Sights and sound subscale. Table 4 also shows a statistically significant association between mean stress scores in domain 2 (Looks and Behaviour of the Infant) and 3 (Parental Role and Relationship) in relation to maturity of the baby, signifying that mothers having full-term babies have experienced more stress than those having pre-term babies. Table 5 illustrates maternal stress as measured by PSS-NICU scale. The mean score was highest for question “Being separated from my baby” (4.43 ± 0.58) followed by question “Feeling staff is closer to my baby than I am” (4.39 ± 0.60). Figure 1 shows mean value for each question of the domain 1, i.e. Sight and Sound of the unit. The mean score was highest for question “The other sick babies in the room” (2.3 ± 0.57) followed by question “The sudden noises of monitors and alarms” (2.09±1.41). Figure 2 shows mean value for each question of the domain 2 (Looks and Behaviour of the Infant). The mean score was highest for question “Seeing my baby looking sick” (4.36 ± 0.53) followed by question “The baby being fed by an intravenous line or tube” (4.18 ± 0.67).

Mean Stress Scores of each component of Sight and Sound domain (domain 1) of PSS: NICU scale

Mean Stress Scores of each component of Looks and Behaviour of the baby domain (domain 2) of PSS: NICU scale
Figure 3 shows mean value for each question of the domain 3 (Parental Role and Relationship). The mean score was highest for question “Being separated from my baby” (4.43 ± 0.57) followed by question “Feeling staff is closer to my baby than I am” (4.39 ± 0.60).

Mean Stress Scores of each component of Parental role and Relationship domain (domain 3) of PSS: NICU scale
Discussion
Maternal stress in NICU setting is often a neglected area. There are only few Indian studies quantifying stress among NICU mothers. It is very crucial for NICU staff and doctors to identify specific stressors among NICU mothers so that appropriate intervention protocols can be developed to address the mother’s fear, reduce their stress and enhance their ability to understand and cope up with the complex NICU environment. Present study was a step in that direction. In a study by Dudek-Shriber, titled “Parent Stress in the Neonatal Intensive Care Unit and the Influence of Parent and Infant Characteristics” and by Reid T titled “Using the Parental Stressor Scale: NICU with a British sample of mothers of moderate risk preterm infants”, younger parents experienced more stress owing to their less experience in the parental role [9, 12, 13]. However, the results of a study by Pichler-Stachl E titled “Parental Stress Experience and Age of Mothers and Fathers After Preterm Birth and Admission of Their Neonate to Neonatal Intensive Care Unit; A Prospective Observational Pilot Study” were directly opposite [2]. A study by Trombini E titled “Environmental factors associated with stress in mothers of preterm newborns” and by Franck L titled “Measuring neonatal intensive care unit-related parental stress” no correlation was found between age of parents and stress levels [14, 15]. Present study did not show any correlation between maternal age and degree of stress. Mean stress scores for all the 3 domains were compared for all the subgroups to look for statistically significant association between the occupation of mother and degree of stress. It showed a statistically significant difference in the mean stress scores of the “Sights and Sounds of the Unit” domain among different occupation with mothers having clerical job experiencing highest level of stress (1.92 ± 1.53) followed by mothers with semi-professional occupation (1.67 ± 1.16). In a study by Dudek-Shriber, parents who were working non-professionals obtained a significantly higher frequency score in the NICU sight and sound than parents who were home-makers-unemployed [12]. Our study showed the similar results. Possible explanation for this could be that these groups of mothers have a better understanding of the technology and equipment owing to their level of education and knowledge and that these equipment and sounds represent the criticality of their baby. Significantly higher frequency mean stress scores were obtained for domain 2 (Looks and Behaviour of the Infant) and domain 3 (Parental Role and Relationship) for term babies.
As per studies by Chourasia N, Schappin R, Dudek-Shriber, Carter J, Minde K and Trause M having preterm baby resulted in significantly higher stress scores and was predictive of stress, and these findings seem sensible also since extremely premature babies are physiologically unstable, demonstrate many aspects in their physical appearance that are different and are less responsive to social interaction than infants who are born later in a pregnancy [1, 5, 12, 16,17,18]. Present study however did not show any such correlation which is contradictory when compared to above studies. The principal reason behind this contradictory finding appears to be the nature of study population, our study included almost equal proportion of term (n = 62) and preterm neonates (n = 58), whereas in all of the above studies proportion of the pre-term babies was more. Also, in our study term, babies were more critical with diagnosis of birth asphyxia, congenital heart disease, congenital malformation and pneumonia being more common in them when compared to preterm babies. The preterm babies with prematurity and small for gestational age as a criteria for admission also included babies having birth weight less than 1500 g who were kept in the higher dependency unit for observation, as per our NICU protocol and that might have caused less stress in mothers of such babies when compared to mothers having term baby with a more critical diagnosis. This appeared to be the reason behind mothers having term babies experiencing greater levels of stress in comparison to those having preterm babies.
There were 111 out of 120 (92.5%) mothers with high level of stress in domain 3 (Parental Role and Relationship). There were 89 out of 120 (74.1%) mothers with medium level of stress in domain 2. There were 110 out of 120 (91.6%) mothers with low level of stress in domain 1.
Using the PSS: NICU, Kegler JJ et al. identified that most stressful domain for parents (n = 204) in their study was alteration the parent-infant relationship and the appearance of the infant while the sights and sounds of the unit domain caused relatively lesser stress [4]. Study by Chourasia N et al. and Franck L also showed similar pattern of results in their study [1, 15]. The findings of present study are consistent to that of above studies. In present study the mean subscale stress score was highest for Parental Role and Relationship domain (4.19), followed by Looks and Behaviour of the Infant domain (3.75) and least for Sights and sound of the unit the domain (2.20). Among the individual items, “Being separated from my baby” (4.43) and “Feeling staff is closer to my baby than I am” (4.39) were the questions with maximum scores.
There are certain limitations to the present study such as Present study measures only mother’s stress levels and father’s stress is not measured or compared. As mother and father both are involved in up-bringing of the child hence stress experiences of fathers is equally important. Furthermore, improvement in paternal perception of neonates suggests that father can actively engage in caring for mothers and sick infants more readily than in past. Further study is required to compare motherhood and fatherhood, to compare culture-sensitive training and thus support medical environment in better care of NICU admitted babies. Another limitation of is that findings of the study cannot be generalised because of the small sample size, study population restricted to one hospital and to one geographical location. Recommendations of future research would include using a larger, randomly selected sample of parents in NICUs that represent different geographical locations of India. Finally, in applying this study finding in practice, this needs to be kept in mind that environment of each NICU has its own unique set of circumstances that can potentially contribute to the stress that parents’ experience.
Conclusion
Maternal stress assessment is a crucial part of overall quality care of newborns. It was not given much emphasis few years back but maternal stress assessment is of paramount importance given its key role in overall neonatal outcome. Our study summarises the impact of intimate environmental factors in the NICU on mothers and benchmarks its importance.
Availability of data and materials
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
References
Chourasia N, Surianarayanan P, Adhisivam B et al (2013) NICU admissions and maternal stress levels. Indian J Pediatr 80(5):380–384
Pichler-Stachl E, Urlesberger P, Mattersberger C et al (2019) Parental stress experience and age of mothers and fathers after preterm birth and admission of their neonate to neonatal intensive care unit; a prospective observational pilot study. Front Pediatr 7(439):1–4
Morgan B, Kayleigh S, Lauren T (2013) Parental responses to stress: PROMIS in the NICU. Crit Care Nurse 33(4):52–60
Kegler JJ, Neves ET, da Silva AM et al (2019) Stress in parents of newborns in a neonatal intensive care unit. Esc Ann Nery 23(1):1–6
Schappin R, Wijnroks L, Venema U et al (2013) Rethinking stress in parents of preterm infants: a meta-analysis. PLoS One 8(2):e54992
Jones L, Woodhouse D, Rowe J (2007) Effective nurse parent communication: a study of parents’ perceptions in the NICU environment. Patient Educ Couns 69(1):206–212
Heidari H, Hasanpour M, Fooladi M (2017) Stress management among parents of neonates hospitalised in NICU. J Caring Sci 6(6):29–38
Carter J, Mulder R, Bartram A, Darlow B (2005) Infants in a neonatal intensive care unit: parental response. Arch Dis Child Fetal Neonatal Ed 90(2):109–113
Reid T, Bramwell R (2003) Using the parental stressor scale: NICU with a British sample of mothers of moderate risk preterm infants. J Reprod Infant Psychol 21(4):279–291
Ganguly R, Patnaik L, Sahoo J et al (2020) Assessment of stress among parents of neonates admitted in the neonatal intensive care unit of a tertiary care hospital in Eastern India. J Edu Health Promot 9(1):1–7
Cekin B, Turan T (2018) The stress levels of parents of premature infants and related factors in Nenoatal Intensive Care Units. Turkish J Pediatr 60(2):117–125
Dudek-Shriber L (2004) Parent Stress in the Neonatal Intensive Care Unit and the Influence of Parent and Infant Characteristics. Am J Occup Therapy 58(5):509–520
Carter J, Mulder R, Frampton C et al (2007) Infants admitted to a neonatal intensive care unit: parental psychological status at 9 months. Acta Paediatrica 96(9):1286–1289
Trombini E, Surcinelli P, Piccioni A et al (2008) Environmental factors associated with stress in mothers of preterm newborns. Acta Paediatrica 97(7):894–898
Franck L, Cox S, Allen A et al (2005) Measuring neonatal intensive care unit-related parental stress. J Adv Nurs 49(6):608–615
Carter J, Mulder R, Darlow B (2007) Parental stress in the NICU: the influence of personality, psychological, pregnancy and family factors. Personal Ment Health 1(1):40–50
Minde K, Whitelaw A, Brown J, Fitzhardinge P (2008) Effect of Neonatal complications in premature infants on early parent-infant interactions. Dev Med Child Neurol 25(6):763–777
Trause M, Kramer L (2008) The effects of premature birth on parents and their relationship. Dev Med Child Neurol 25(4):459–465
Acknowledgements
We wish to acknowledge and thank the Dean of our institute, Dr. Ramesh Bharmal, for giving permission to publish this article.
Funding
None.
Author information
Authors and Affiliations
Contributions
Tazeem Fatima Ansari: conceptualization, methodology, software, data curation, writing—original draft preparation, writing—reviewing and editing. Poonam Wade: visualization, investigation, supervision, software and validation. Vinaya Singh: reviewing and editing. Sushma Malik: visualization, investigation, supervision, reviewing and editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Ethical approval was obtained from the institutional ethics committee (Topiwala National Medical College) ECARP (IEC) number- ECARP/2018/58. Written informed consent was obtained from parents/guardian of the children enrolled in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ansari, T.F., Wade, P., Singh, V. et al. Maternal stress experiences with neonatal intensive care unit admissions. Egypt Pediatric Association Gaz 70, 47 (2022). https://doi.org/10.1186/s43054-022-00138-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43054-022-00138-7